Perioperative ctDNA-Based MRD Detection Effectively Predicts Postoperative Recurrence in Non-Small Cell Lung Cancer: Findings from the Prospective Multicenter LUNGCA-1 Study
In November 2021, the journal Clinical Cancer Research (a CAS Q1 TOP journal, IF = 12.531) published a study byProfessor Liu Lunxu’s Team from West China Hospital of Sichuan University, in Collaboration with Sichuan Provincial People’s Hospital, Chengdu Shangjin Nanfu Hospital, and Wuxi Zhenhe Biotechnology Co., Ltd.(hereinafter referred to as “Zhenhe Technology”) in collaboration on the research findings titled “Perioperative ctDNA-based Molecular Residual Disease Detection for Non-Small Cell Lung Cancer: A Prospective Multicenter Cohort Study (LUNGCA-1)”.
The LUNGCA study is a large-scale, multicenter, prospective investigation into molecular prognostic biomarkers for lung cancer, led by Professor Liu Lunxu’s team. The currently published article presents the analytical findings from the LUNGCA-1 cohort, revealing that perioperative circulating tumor DNA (ctDNA) can effectively predict postoperative recurrence in patients with non-small cell lung cancer (NSCLC), thereby serving as a reliable indicator for early detection of minimal residual disease (MRD) after surgery in NSCLC patients.
1. Large sample size: The total cohort comprised over 400 cases; the perioperative LUNGCA-1 cohort included 330 patients with stage I–III non-small cell lung cancer (NSCLC) for analysis, with 330 tissue samples and 950 plasma samples collected;
2. The composition of enrolled patients aligns with the distribution of real-world lung cancer surgical patients: Stage I accounted for 67.0%, and lung adenocarcinoma accounted for 84.8%;
3. Long follow-up duration: median follow-up time of 1,068 days (range: 341–1,340 days);
4. The study results validated that ctDNA within one month postoperatively can serve as a biomarker for predicting recurrence and detecting MRD; perioperative postoperative ctDNA-MRD positivity is an independent risk factor for shortened RFS in patients; the relative contribution of ctDNA-MRD status to RFS prediction in multivariate Cox analysis was higher than the sum of clinical variables such as TNM staging;
5. Correlation between ctDNA-MRD status and adjuvant therapy outcomes: Multivariate analysis revealed that in MRD-positive patients, adjuvant therapy was significantly associated with recurrence-free survival (RFS), and adjuvant therapy improved patient RFS; in MRD-negative patients, adjuvant therapy showed no significant correlation with patient RFS.
This study included 330 patients with stage I–III non-small cell lung cancer (NSCLC) enrolled in the LUNGCA cohort from September 2017 to May 2020, using Geneseeq’s 769-gene NGS panel (product: BestPro®), tumor tissue samples (n=330) and perioperative plasma samples (preoperative, 3 days postoperative, and 1 month postoperative; n=950) from these patients were analyzed. A tissue-first strategy was employed, supplemented by Genetron Health’s MRD-MinerVa algorithm, to determine ctDNA positivity. The primary endpoints were perioperative ctDNA positivity status and relapse-free survival (RFS).
1. Characteristics of NSCLC Patients and Perioperative ctDNA Status
Among the enrolled patients, 67.0% were at stage I, and 84.8% had lung adenocarcinoma. The median follow-up time was 1,068 days (range: 341–1,340 days), with 21.2% of patients experiencing local recurrence or distant metastasis. The predominant mutation type detected in tumor tissues was point mutations, accounting for 90.28%, while copy number variations (CNVs) and fusions accounted for a lower proportion of 9.72%. The driver genes with the highest mutation frequencies in both tumor tissues and plasma circulating tumor DNA (ctDNA) were TP53 and EGFR; other frequently mutated genes included KMT2D, CDKN2A, PTEN, and PIK3CA (Figure 1). Patients with a tumor diameter greater than 3 cm, pathological stage II or III non-small cell lung cancer (NSCLC), or lung squamous cell carcinoma (LUSC) were more likely to test positive for preoperative plasma ctDNA. Across all three perioperative time points, only pathological stage was significantly associated with ctDNA status.
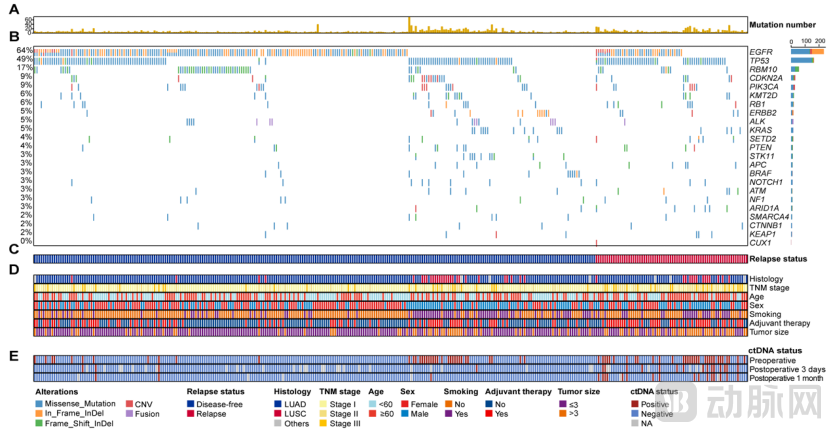
Figure 1. Patient characteristics, somatic mutations in tumor tissue, and perioperative ctDNA detection status
(A) Number of somatic mutations in tumor tissues. (B) Frequently mutated driver genes in tumor tissues. (C) Patient recurrence status. (D) Clinicopathological characteristics of patients. (E) ctDNA status detected preoperatively, 3 days postoperatively, and 1 month postoperatively.
2. Correlation Between Preoperative ctDNA Status and Prognosis in NSCLC
Among patients with preoperative ctDNA positivity, 46.4% (32/69) experienced postoperative recurrence, whereas only 14.6% (38/261) of those with negative results had recurrence (P<0.001) (Figure 2A). Patients with preoperative ctDNA positivity had significantly shorter recurrence-free survival (RFS) than those with negative ctDNA status (HR 4.2; 95% CI, 2.6–6.7; P<0.001) (Figure 2B). Preoperative ctDNA status was an independent risk factor for RFS (HR 2.6; 95% CI, 1.3–5.1; P=0.005).
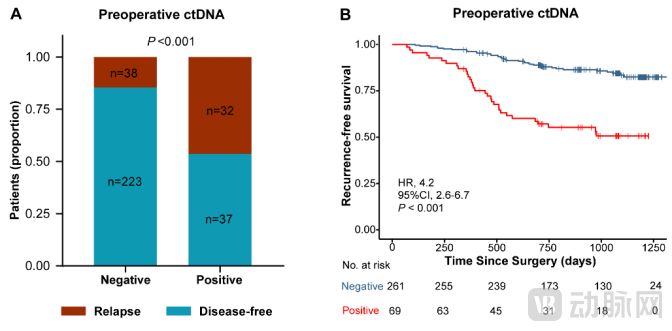
Figure 2. Prognostic Value of Preoperative ctDNA in NSCLC Patients
(A) Comparison of the overall recurrence rate between patients with negative preoperative ctDNA and those with positive preoperative ctDNA.
(B) Kaplan-Meier curves showing RFS stratified by preoperative ctDNA status.
3. Postoperative ctDNA as a Biomarker for MRD Detection and Recurrence Prediction
Within one month postoperatively, the recurrence rate among patients with positive ctDNA-MRD was 80.8% (21/26), significantly higher than the 16.2% (49/303) observed in negative patients (P < 0.001) (Figure 3C). Postoperative ctDNA-MRD status was a significant predictor of recurrence in postoperative patients (HR, 11.1; 95% CI, 6.5–19.0; P < 0.001) (Figure 3D). Multivariate Cox analysis revealed that positive postoperative ctDNA-MRD was an independent risk factor for shortened recurrence-free survival (RFS) (P < 0.001). Furthermore, in the multivariate Cox analysis, the relative contribution of ctDNA-MRD status to RFS prediction exceeded the combined contribution of clinical variables such as TNM staging (Figure 3E).
Note: Postoperative ctDNA-MRD positivity is defined as the detection of ctDNA in plasma at 3 days and/or 1 month after surgery; postoperative ctDNA-MRD negativity is defined as the absence of detectable ctDNA in plasma at both 3 days and 1 month after surgery.
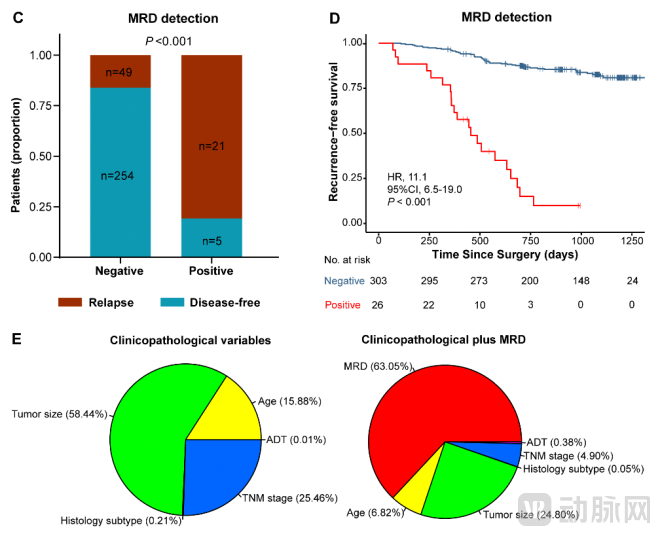
Figure 3. Prognostic Value of Perioperative ctDNA in Patients with NSCLC
(C) Comparison of the overall recurrence rate between patients with ctDNA-based MRD negativity and those with MRD positivity. (D) Kaplan-Meier curves showing RFS stratified by ctDNA-based MRD status. (E) Multivariate Cox analysis of the relative contribution of each parameter to RFS prediction, including clinicopathological variables (left) and clinicopathological variables plus ctDNA-based MRD (right).
4. Correlation between ctDNA-based MRD and Adjuvant Therapy Outcomes
Among the 26 patients who were ctDNA-MRD positive within one month after surgery, all 9 patients who did not receive adjuvant therapy experienced recurrence; among the 17 patients who received adjuvant therapy, 5 did not experience recurrence (Figure 4A). Univariate analysis revealed that adjuvant therapy improved relapse-free survival (RFS) in MRD-positive patients (HR, 0.3; 95% CI, 0.1–0.8; P = 0.008); conversely, adjuvant therapy was associated with worse RFS in MRD-negative patients (HR, 3.1; 95% CI, 1.7–5.5; P < 0.001) (Figure 4B). Multivariate analysis, which included clinical stage and other factors, demonstrated that adjuvant therapy was significantly associated with RFS in MRD-positive patients, whereas no significant association was observed between adjuvant therapy and RFS in MRD-negative patients.
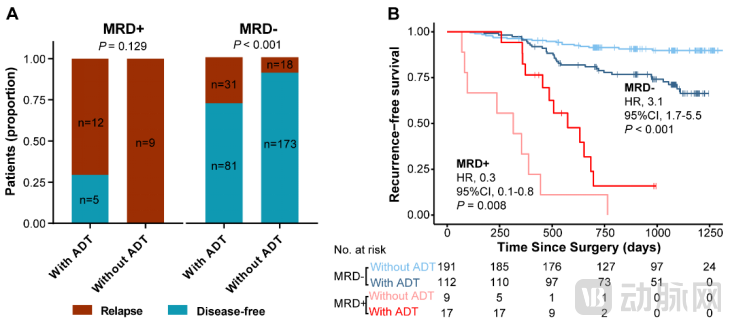
Figure 4. Correlation between RFS and adjuvant therapy in MRD-positive and MRD-negative patients
(A) Comparison of the overall recurrence rates between MRD-positive patients who received adjuvant therapy and those who did not (left); comparison of the overall recurrence rates between MRD-negative patients who received adjuvant therapy and those who did not (right).
(B) Kaplan-Meier analysis comparing RFS in MRD-positive patients who received adjuvant therapy (dark red line) versus those who did not (light red line), and in MRD-negative patients who received adjuvant therapy (dark blue line) versus those who did not (light blue line).
This large-scale, prospective, multicenter cohort study of non-small cell lung cancer (NSCLC) demonstrates that perioperative circulating tumor DNA (ctDNA) can effectively detect minimal residual disease (MRD) and identify patients at high risk of recurrence. ctDNA-MRD testing provides critical reference for postoperative treatment decision-making in lung cancer and holds substantial clinical utility in postoperative patient management.
Expert Profile
