From Tianjin Digital Health Community to HMO: The Localization of Health Maintenance Organizations in China
In October 2021, the Leading Group for Healthcare Reform of the State Council issued the “Implementation Opinions on Deepening the Promotion of Sanming City’s Experience in Fujian Province and Furthering Healthcare System Reform” (Guo Yi Gai Fa [2021] No. 2) (hereinafter referred to as “Document No. 2”), which mentioned “advancing the development of medical consortia” sixteen times and emphasized strengthening performance evaluations of medical consortia centered on “people’s health.”
The healthcare service system, once “treatment-centered,” now stands at a crossroads of transformation. Industry insiders point out that building health maintenance organizations (HMOs) centered on “health” through digital technology will provide new directions for further deepening healthcare reform.
Notably, among the “Top Ten New Measures to Advance Healthcare Reform and Serve Public Health” for 2020, released at the 2021 National Conference on Promoting Experience in Deepening Healthcare Reform, the top-ranked initiative was the digital healthcare-led reform model known as the “Tianjin Primary Care Digital Health Consortium.” Its hallmark achievement lies in establishing a tightly integrated internet-based medical consortium within a provincial-level administrative region, thereby forming a highly effective digital health stewardship organization.
In line with the spirit of Sanming’s healthcare reform, Tianjin’s exploratory practices have provided a practical pathway for promoting the Sanming model across China and for implementing digitalized health stewardship organizations on a broader scale.
According to statistics from the National Healthcare Security Administration, the surplus rate of the urban and rural resident basic medical insurance fund decreased from 33.7% in 2009 to 4.5% in 2019. Meanwhile, driven by socioeconomic development, improvements in living standards, and an accelerating trend of population aging, demand for medical services across China has grown rapidly.
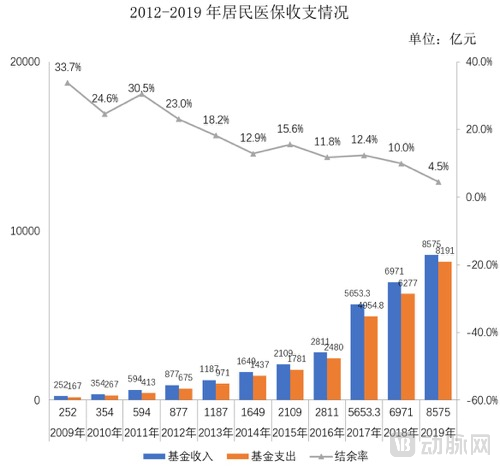
Image source: 2019 Statistical Bulletin on the Development of China's National Healthcare Security
Amidst the continuously growing demand for medical services and the declining surplus rate of medical insurance funds, the interplay between these two factors makes it both a practical necessity and a historical inevitability to establish a healthcare delivery model that facilitates a shift from being “disease-centered” to “health-centered.”
The “Three-Medical Linkage” reform launched in Sanming in 2012 has anchored a new coordinate system for China’s healthcare reform. After experiencing the 1.0 phase of “addressing chaos and curbing waste” and the 2.0 phase of “establishing rules and instituting systems,” the current Sanming healthcare reform has entered the 3.0 phase, which is “health-centered.”
In September this year, Sanming issued the Action Plan for Implementing the “Six Major Projects” to Relaunch Healthcare Reform in Sanming City, which calls for further implementation of the project to improve the universal health stewardship system, establish a rational order for tiered diagnosis and treatment, strengthen the health stewardship system, and refine health stewardship regulations. It also specifies that surplus funds from bundled payments of the basic medical insurance fund may be included in medical service revenue and used for health stewardship, chronic disease management, health promotion, and related activities.
By establishing close-knit county-level medical consortia, Sanming has integrated healthcare resources and improved the mechanism for health performance evaluation, guiding the shift of healthcare focus and resources to the grassroots level, promoting collaboration between clinical care and disease prevention, and establishing a "gatekeeper" system for health. Meanwhile, medical insurance funds, basic public health service subsidies, and government grants are bundled and allocated to general hospitals, with surpluses retained for use and reasonable overspending shared, thereby realizing a health management and protection system centered on “preventive treatment” and “holistic health.”
Guided by the goals and direction of the “Sanming Healthcare Reform 3.0,” a health-centered healthcare management and protection system is rapidly taking shape, with localized implementation expanding across broader scopes and greater depths.
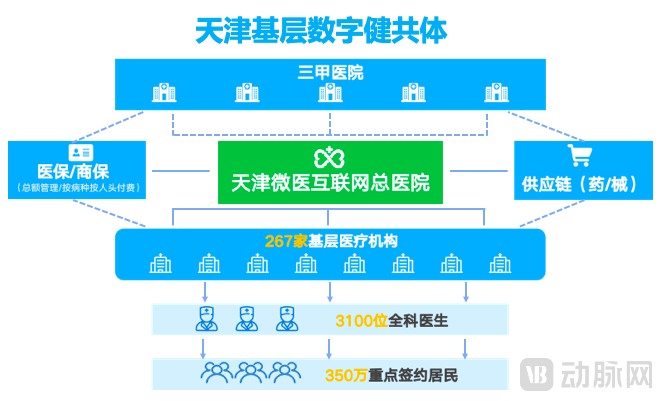
In January 2020, the Tianjin Municipal People’s Government and WeDoctor signed the “Strategic Cooperation Agreement on Digital Health.” Under the leadership of the Tianjin Municipal Health Commission, WeDoctor General Hospital in Tianjin took the lead in collaborating with 267 primary healthcare institutions across the city to jointly establish the “Tianjin Primary Care Digital Health Consortium,” with full-scale construction launched by the end of April that year. By implementing the “Four Clouds”—namely “Cloud Management,” “Cloud Services,” “Cloud Pharmacy,” and “Cloud Diagnostics”—to empower primary care, the Consortium has created an efficient health maintenance system that covers the entire life cycle and all stages of health for residents.
Unlike traditional medical institutions, the Tianjin Grassroots Digital Health Consortium has set its primary goal not merely on treating patients’ illnesses, but on tangibly improving residents’ health indicators. In simple terms, the aim is to help people avoid falling ill, reduce the incidence of disease, and ensure that when illness does occur, it is treated at the lowest possible cost.
Based on this premise, the Healthcare Community leverages digital technology to empower the existing healthcare system. By revitalizing local medical resources and using chronic disease management as an entry point, it has explored payment models such as “global bundled payments” and “capitation/diagnosis-related group (DRG) payments” for medical insurance, thereby implementing a performance constraint mechanism characterized by “retention of surpluses and no compensation for deficits.”
This model has effectively driven the transformation of the healthcare service system from a “price differential” to an “efficacy differential.” The former is disease-centered, operates on a fee-for-service basis, fragments medical services from patient data, and bases healthcare providers’ performance compensation on a “piece-rate” model derived primarily from price differentials in the supply chains of pharmaceuticals and consumables. In contrast, the latter is health-centered, adopts case-based or capitation payment methods, delivers integrated online-and-offline services across the entire life cycle, and derives performance incentives from the “efficacy differential” generated by improvements in patient health outcomes and reductions in medical expenditures.
Drawing on the practical experience of the Sanming health stewardship system, Tianjin’s grassroots digital health community has leveraged digital technologies to establish a tightly integrated medical consortium on a broader scale, driving a shift in health insurance payment models from “paying for specific medical services” to “paying for population health.” The enhancement of healthcare accessibility, affordability, and effectiveness by technology-enabled Health Maintenance Organizations (HMOs) has already yielded visible results.
Statistical data show that after more than a year of development, the standardized management rate for diabetic patients in primary healthcare institutions participating in the Medical Community pilot reached 76.68%. Analysis of patient samples managed for over three months revealed a 21.58% increase in the blood glucose control rate. Meanwhile, primary healthcare institutions that have implemented capitation-based payment achieved medical insurance surplus rates ranging from 16% to 31%. Furthermore, driven by the dual improvement in primary care service capacity and accessibility for patients, outpatient visits at pilot primary hospitals within the Medical Community increased by 120%.
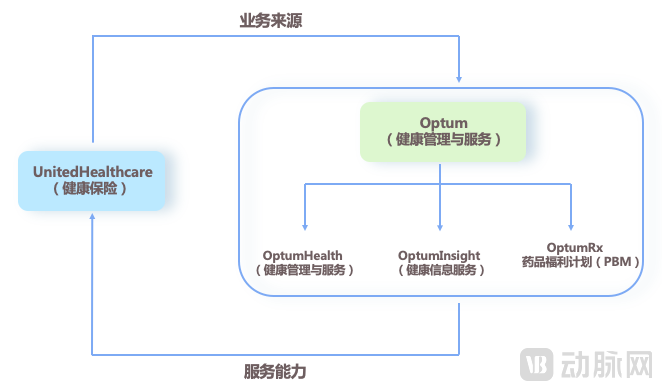
In 1973, the United States enacted the Health Maintenance Organization Act, encouraging the rapid development of Health Maintenance Organizations (HMOs) and significantly advancing the growth of managed care in the country. UnitedHealth Group stands out as the most representative example. Its defining feature is the strategic synergy between its two major segments: UnitedHealthcare, which provides health insurance, and Optum, which delivers health management and services. Optum is further divided by business type into OptumHealth (providing healthcare services), OptumInsight (providing health information services), and OptumRx (providing pharmacy benefit management, or PBM). As evident, its HMO model’s key components correspond to four core capabilities: insurance, healthcare delivery, pharmaceuticals, and digitalization.
Although the healthcare systems of China and the United States differ significantly, they share a common core objective: to reduce costs and enhance efficiency across the entire health service system by establishing a health stewardship framework that strengthens effective oversight of hospitals, physicians, and other stakeholders while prioritizing patient health maintenance. Therefore, a comparison with Tianjin’s Digital Health Community practice reveals that both approaches converge on the same foundational capability model.
First is payment capacity. Similar to UnitedHealth’s model of “charging fixed prepaid insurance premiums,” the Tianjin Primary Care Digital Health Consortium adopts payment methods such as “global bundled payments” and “capitation/disease-based bundled payments,” thereby enabling healthcare payers to cover health outcomes at predetermined costs.
Medicare, the federal health insurance program for the elderly and disabled in the United States, and Medicaid, the medical assistance program administered by state governments, account for two-thirds of UnitedHealth’s business. In China, where the basic medical insurance system is implemented and serves as the most critical component of the insurance framework, the core of building a Chinese-style HMO lies in securing large-scale purchasing power from medical insurance funds.
Next is healthcare service capacity. Through the “Cloud Services” platform, which features centralized operations, unified management, division of responsibilities, and tiered service delivery, and the “Cloud Examinations” platform, which enables mutual recognition of laboratory and imaging test results, 267 primary healthcare institutions have achieved service coordination. This facilitates residents’ enrollment in localized grid-based management, standardizes medical quality control criteria, establishes a standardized healthcare service system, and provides the public with multi-form, multi-level, and diversified healthcare services.
Next is pharmaceutical service capability. The unified “Cloud Pharmacy” platform effectively aligns the drug formularies of primary healthcare institutions with those of secondary and tertiary medical institutions, extending chronic disease management and long-prescription systems at the grassroots level. By strengthening prescription review and regulation, facilitating prescription outflow, optimizing logistics and distribution, and providing medication guidance, this approach addresses issues such as inadequate drug supply and irregular usage in primary healthcare institutions, while also effectively controlling drug costs.
Lastly, digital capabilities. The “Four Clouds” platform provides digital support for all operations of the Healthcare Community, enabling the mobilization and circulation of medical resources on a broader scale and optimizing their allocation. Furthermore, through intelligent analysis of big data from healthcare, health insurance, and pharmaceutical sectors, it has significantly enhanced the overall operational efficiency of medical services, pharmaceuticals, and health insurance.
A comparison of HMO practices in China and abroad reveals that building capabilities in four key areas—medical care, pharmaceuticals, insurance, and data—is critical to realizing value. Represented by the experience in Tianjin, these initiatives not only possess these four fundamental capabilities but also explore the establishment of a Chinese-style health stewardship system tailored to the characteristics of China’s healthcare delivery framework. As healthcare reform deepens and the digital health industry rapidly expands, such practices are expected to be implemented across more regions, providing the public with higher-quality, accessible health maintenance services and shaping a “sustainable future” for the medical and health industry.