The Golden Decade of Heart Failure Device Therapy: Cardiovascular Medicine's Final Frontier
The Final Frontier in Cardiovascular Care: New Multi-Billion Dollar Opportunities in Device-Based Therapy
Aging Population and High Prevalence of Chronic Diseases Drive Growth in the Heart Failure Patient Pool
Heart Failure (HF), abbreviated as heart failure, is not an independent disease but rather a severe manifestation of various cardiac conditions or the terminal stage of their progression. Due to demographic shifts in China, particularly the intensifying aging of the population, and the rising prevalence of chronic diseases such as coronary heart disease, hypertension, diabetes, and obesity, coupled with advances in medical care that have extended the survival of patients with cardiac disorders, the prevalence of heart failure—as the end-stage outcome of various cardiovascular diseases—has continued to rise, with persistently high mortality and readmission rates.
Nearly 30 million patients worldwide:
In 2019, the global number of patients with heart failure reached 29.7 million, and it is projected to further increase to 38.7 million by 2030, representing a compound annual growth rate (CAGR) of 2.5% from 2024 to 2030. The prevalence of heart failure in developed countries ranges from 1.5% to 2.0%, while the prevalence among individuals aged ≥70 years is ≥10%.[1]。
In the United States, the number of heart failure patients reached 6.578 million in 2019 and is projected to reach 7.284 million in 2024, representing a growth rate of 2.1%. The annual growth rate from 2024 to 2030 is expected to be 2.0%, with the patient population reaching 8.208 million by 2030.
Global Aging Drives Up Heart Failure Prevalence:
For individuals aged 20 years and older, the prevalence of heart failure approximately doubles with each 10-year increase in age.[2]. Among US men, the prevalence of heart failure is 0.2% in those aged 20–39 years, 1.5% in those aged 40–59 years, 7.8% in those aged 60–79 years, and 8.6% in those aged 80 years and older. Among patients with heart failure, 88% are over 65 years of age, and 49% are over 80 years of age.[3]. From 2017 to 2030, the absolute number of patients with heart failure is projected to increase by 46%.[4]。
China Exhibits High Prevalence and Incidence Rates:
The 2003 epidemiological survey showed that the prevalence of heart failure among adults aged 35–74 years in China was 0.9%.[5], with approximately 13.7 million patients in 2021. There were 2.14 million new cases in 2019, representing a growth rate of 1.6% from 2014 to the present.
Compared with other heart failure study populations in China, it has been found that the average age of hospitalized heart failure patients is on the rise, currently standing at 65 years. In 2019, the number of heart failure patients rapidly increased to 10.678 million, and is projected to reach 16.14 million by 2030, representing a growth rate of 3.6%.
China-HF Study[6]The data show that the case fatality rate among hospitalized heart failure patients is 4.1%. In 2019, the number of deaths due to heart failure reached approximately 1.709 million, and it is estimated to reach 1.934 million by 2030. As the growth rate of mortality is slightly lower than that of prevalence, the pool of heart failure patients is expected to increase significantly in the future.
Currently, heart failure is considered a chronic, spontaneously progressive disease. Early myocardial remodeling can partially compensate for cardiac function, but as myocardial remodeling worsens, cardiac function gradually transitions fromTransition from Compensation to Decompensation, with obvious symptoms and signs.
Therefore, based on the onset and progression of heart failure, it is classified intoEarly Stage, Progressive Stage, End-Stagestages. The management of patients with heart failure should be patient-centered, encompassing multiple phases including pre-hospitalization, during hospitalization, and post-discharge. This includes acute-phase treatment, initiation and optimization of chronic heart failure therapy, diagnosis and management of comorbidities, planned and targeted long-term follow-up, cardiac rehabilitation, lifestyle interventions, health education, and patient self-management. These measures are of significant importance in improving patients' quality of life, delaying disease progression, and reducing readmission rates. The therapeutic focus varies across different stages:
① Early-stage heart failure: The patient is at high risk of developing heart failure; early prevention of related risk factors is emphasized during this stage;
② Progressive Stage of Heart Failure: The focus lies on the comprehensive optimization of treatment regimens and enhanced management to slow the progression of heart failure and reduce readmission rates (by preventing the progression of structural heart disease, including valvular and myocardial disorders), prevent sudden cardiac death (using ICDs, WCDs, etc.), and rapidly stabilize hemodynamics, increase cardiac output, and maintain tissue and organ perfusion during acute decompensated heart failure episodes (through pharmacotherapy and ventricular assist devices, VADs).
③ End-Stage Heart Failure: Palliative care, heart transplantation, or long-term VAD.
Unlike the treatment of primary cardiovascular diseases, the systematic management of heart failure across its various stages involves multifaceted assessment and intervention. Ranging from early identification of risk factors to control of disease progression, it requires the selection and comprehensive application of multiple therapeutic options tailored to individual patient conditions, thereby facilitating optimization of cardiac function at different stages of the disease course. Although the goals and methods of treatment for each stage of heart failure overlap, they also have distinct characteristics. Therefore, a clear understanding of the overall natural history of the disease, the disease spectrum, and the patient’s position within the clinical care pathway is crucial.

Figure 1. The Evolution of the Disease Spectrum Drives 30 Years of Change in Cardiovascular Devices
As the domestic disease spectrum evolves, China’s cardiovascular device industry is poised to experience a third wave of blockbuster products—ventricular assist devices (VADs)—unlocking a market opportunity worth tens of billions of yuan.
①PCI:Since China’s reform and opening-up, changes in people’s lifestyles driven by economic development have led to a rapid increase in the prevalence of chronic diseases, represented by coronary heart disease (CHD) and diabetes, since the 1990s. This trend has significantly spurred the development of corresponding pharmaceutical and medical device therapies. Percutaneous coronary intervention (PCI) for CHD was introduced into China in 1983, underwent widespread adoption from 1996 to 2005, and achieved procedural maturity, standardization, and scale-up during 2000–2010. These developments created a multi-billion-yuan opportunity for the domestic PCI industry, enabling listed companies such as MicroPort and Lepu Medical to successfully achieve import substitution with domestically produced alternatives.
②Valve Intervention:As the first wave of China’s “baby boomers”—those born in the 1950s—began turning 60 around 2010, the country’s demographic structure entered an aging society. The rapidly rising incidence of age-related valvular heart disease has shifted the historical etiological profile of valvular disorders, which was previously dominated by rheumatic valvular disease. Furthermore, because elderly patients often have poor tolerance for surgical trauma, this trend has accelerated the domestic development of interventional valve products. In 2018, Hong Kong Stock Exchange’s Chapter 18A listing rules removed the IPO bottleneck for pre-revenue medical device companies, enabling a cohort of TAVR-focused listed companies represented by Venus Medtech, MicroPort CardioFlow, and Peijia Medical to emerge amid vast market opportunities. Looking ahead, the even larger market potential for transcatheter mitral and tricuspid valve repair will likely drive the listing of more valvular heart disease companies.
③ Ventricular Assist Device (VAD)): Over the past two decades, the disease progression of cardiovascular chronic conditions in China has evolved. Cardiovascular diseases, represented by hypertension and coronary heart disease, are entering the final battleground of cardiovascular pathology—heart failure—as the population ages. The continuously rising incidence and prevalence rates are imposing a growing burden on the healthcare system. As heart failure progresses to stages where pharmacological interventions become ineffective, medical devices for heart failure treatment, particularly Ventricular Assist Devices (VADs), will see significant development. Furthermore, bolstered by the accumulation of manufacturing capabilities over the past decade and the "engineer dividend" resulting from the expansion of higher education, there is strong potential for the domestic production of VADs, often referred to as the "crown jewel of medical devices." In the next ten years, against the backdrop of national policies and innovation and development in the domestic capital market, Chinese-made VADs are expected to achieve large-scale market share surpassing imported products, leading to the emergence of multiple publicly listed companies in this sector.
Normal cardiac function relies on regular electrical rhythms to ensure coordinated myocardial contraction and effective blood pumping. In the setting of acute or chronic heart failure, myocardial dysfunction manifests in three key aspects: structural abnormalities (involving the myocardium and valves), electrical disturbances, and impaired myocardial contractility (mechanical activity), leading to pump failure. Device-based therapies for heart failure are specifically designed to address these three domains, offering a diverse range of combination solutions. Clinical application requires selecting appropriate devices based on the patient’s disease stage, specific clinical presentation, and comorbidities.
From the perspective of the disease stage,Early-stage heart failureThe focus is on patient management and prevention of risk factors, with devices primarily used for remote monitoring and adherence management. From the perspective of device categories based on electrical and mechanical energy principles, there are similarShort-Term Bridging Therapy vs. Long-Term Implantable Therapyrequirements.Progressive Stage of Heart FailureDue to the frequent acute exacerbations of chronic heart failure and the short-term high risk of rehospitalization and sudden cardiac death, there is a substantial demand for transitional therapies (short-term VAD and WCD); similarly,In End-Stage Heart FailureIt also shares common features with replacement therapy (long-term VAD) and long-term management (ICD). (See “Stages of Heart Failure Progression” and “Device-Based Therapies” in Figure 2.)
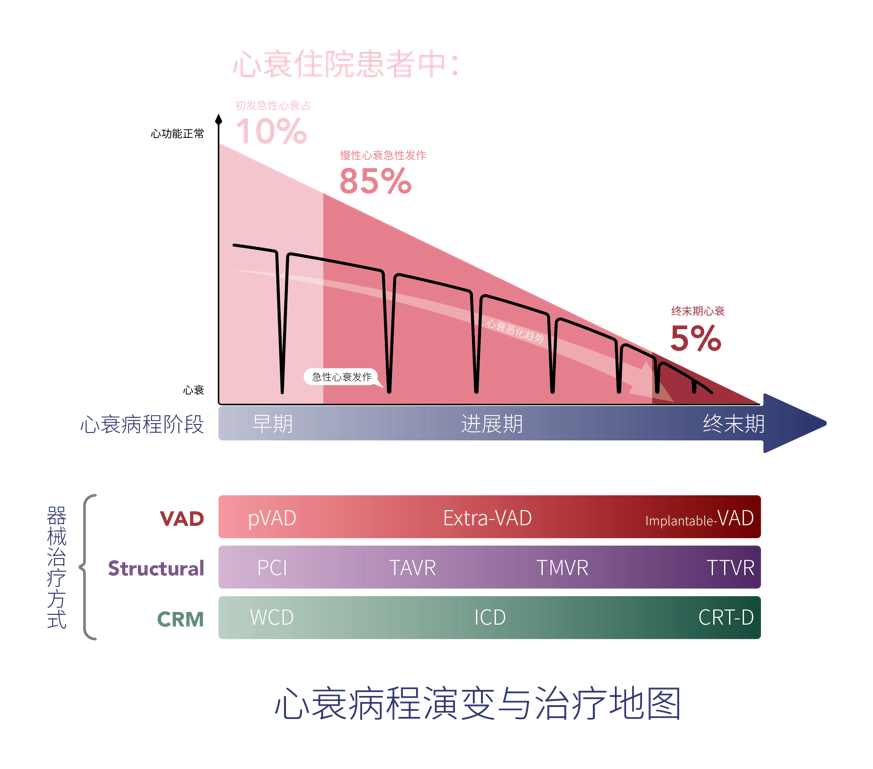
Figure 2. Disease Progression and Treatment Landscape in Heart Failure
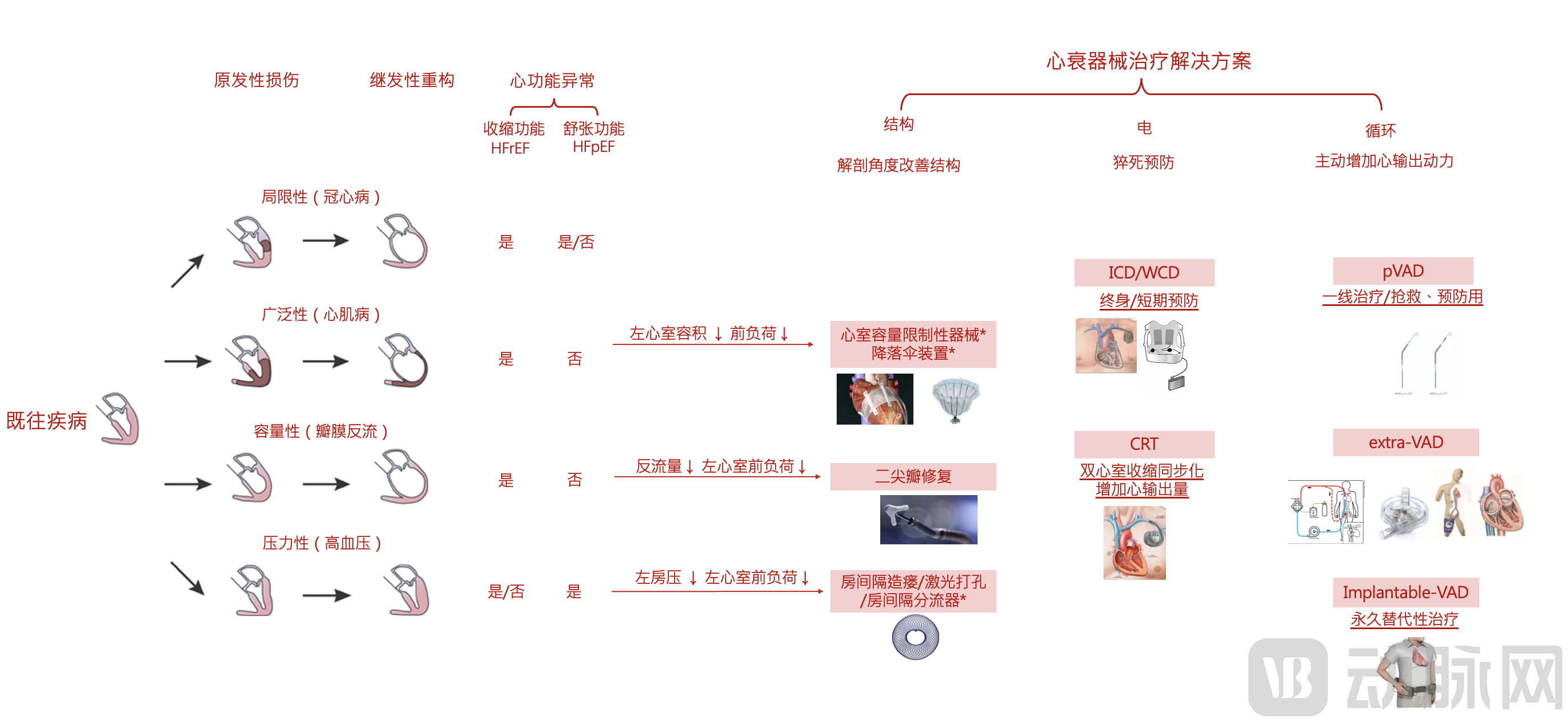
Figure 3. Major Pathogenic Mechanisms of Heart Failure and Principles of Device-Based Therapy (Note: *Evidence-based medical support for the treatment regimen awaits further refinement)
① Structural Cardiology (Structural Improvement in Heart Failure): The Evolution of the Disease Spectrum from Coronary Artery Disease to Ischemic Cardiomyopathy and Then to Heart Failure Drives Iterative Advancements in the Structural Heart Disease Industry
Since a large proportion of heart failure patients suffer from ischemic cardiomyopathy caused by coronary artery disease, leading to symptomatic relative mitral regurgitation (also known as functional mitral regurgitation, FMR) due to ventricular dilation, mitral valve repair devices are primarily used to treat heart failure patients. The recent rise of the percutaneous mitral valve repair market further highlights the substantial demand among heart failure patients in China. Meanwhile, the advancement of emergency percutaneous coronary intervention for ST-elevation myocardial infarction (STEMI) in recent years also demonstrates the significant clinical need for treating the primary underlying conditions of acute heart failure in China.
As heart failure progresses from left-sided to combined right-sided involvement, some patients with mitral regurgitation advance to a stage featuring both mitral and tricuspid regurgitation. The high mortality rate associated with surgical tricuspid valve repair has driven the market development of transcatheter tricuspid valve repair.
Meanwhile, structural therapies for heart failure are continuously evolving, increasingly exhibiting the characteristics of "non-standardized" medical devices. The market offers a variety of mitral valve repair and replacement devices with diverse structural configurations, such as edge-to-edge repair, artificial chordae tendineae, annuloplasty, and valves with various designs for replacement. Additionally, there are devices targeting heart failure with preserved ejection fraction (HFpEF), including interatrial shunts and fistula-creation systems, as well as restrictive pericardial devices and parachute-like implants aimed at left ventricular remodeling. These interventions fundamentally work by reducing left ventricular preload to alleviate or treat heart failure. On one hand, structural therapy for heart failure provides substantial room for innovation in novel devices, particularly at the conceptual level. On the other hand, the diversity of these devices has led to smaller clinical sample sizes, leaving evidence-based medical data incomplete. Currently, only Abbott’s MitraClip has achieved large-scale, mature global application (see Figure 3).
② Rhythm Management (Sudden Cardiac Death Prevention): The high incidence of sudden cardiac death in the progression from ischemic cardiomyopathy to heart failure drives the demand for early-stage prevention.
Heart failure is a relatively common cause of sudden cardiac death, with 30%-50% of deaths in heart failure patients attributed to sudden cardiac death; furthermore, the incidence of sudden cardiac death increases during periods of worsening heart failure symptoms.
The progression of heart failure is correlated with the incidence of sudden cardiac death: as heart failure advances from the initial stages (Stages A and B, or NYHA Class II) to the moderate and terminal stages (Stages C and D, or NYHA Classes III and IV), the incidence and probability of sudden death increase progressively. Among the causes of death in patients with heart failure, progressive pump failure, unexpected sudden cardiac death, and sudden cardiac death occurring during episodes of clinical deterioration each account for approximately one-third of all heart failure-related deaths. Arrhythmias are considered the cause of sudden death in 39% of patients with heart failure.
Currently, the time window for primary prevention of sudden cardiac death involves evaluating and considering ICD implantation more than three months after revascularization. However, patients remain at high risk within the first three months, with significantly higher early mortality rates observed in those with left ventricular dysfunction (e.g., LVEF ≤30%) following PCI or CABG. For patients at short-term high risk during this initial three-month period, a non-invasive wearable cardioverter-defibrillator (WCD) can be used as a transitional preventive measure. Subsequently, an ICD may be implanted for patients identified as having a long-term high risk of sudden cardiac death.
③ Mechanical Kinetic Energy (Circulatory Support): Short-Term Support for Acute Heart Failure and Long-Term Supportive Therapy Needs for End-Stage Heart Failure
Similar to electrical abnormalities in the progression of heart failure, mechanical kinetic dysfunction in heart failure also exhibits characteristics of frequent occurrences during the advanced stages and persistence in the end-stage. During the progression of chronic heart failure, there are multiple acute exacerbations, with the frequency increasing as the disease advances, ultimately evolving into persistent cardiac insufficiency characteristic of end-stage heart failure. Since recovery from an acute heart failure episode is highly likely within a short term (within one month), the window for circulatory support generally requires only short-term support (within three months). Long-term implantable ventricular assist devices (VADs) are rarely needed, considering the comprehensive trade-offs between traumatic risks and costs. This clinical scenario prioritizes short-term VADs as first-line rescue or bridge therapy; patients can be weaned off and discharged upon recovery without the need for long-term implantation. In contrast, patients with end-stage heart failure require long-term circulatory support, making heart transplantation or long-term implantable VADs more suitable options (see Figure 5).
Target Market Size for Heart Failure: Acute and Chronic Heart Failure
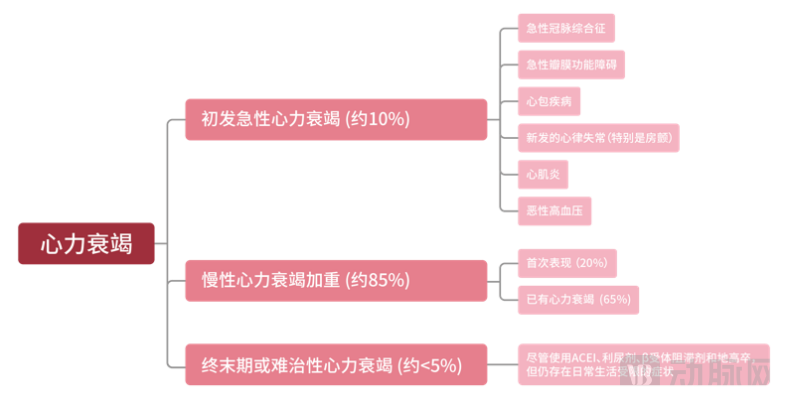
Figure 4. Market Size of Heart Failure Subsegments
Among hospitalized patients with heart failure, the vast majority are those experiencing acute decompensation of chronic heart failure or their first acute episode; these patients account for 95% of all hospitalized cases (see Figure 4). All admitted heart failure patients comprise three groups:
① Initial acute heart failure caused by various primary diseases:including acute coronary syndrome (withAcute Myocardial Infarctionas representatives),Atrial FibrillationInitial acute heart failure often leads patients to seek emergency care. In China, treatment for the underlying condition (emergency PCI) is frequently administered directly in chest pain centers within emergency departments. In recent years, the etiological composition of heart failure in China has undergone significant changes: the proportion of valvular heart disease (particularly rheumatic valvular disease) has declined year by year, while coronary artery disease, hypertension, and dilated cardiomyopathy have become the predominant causes of heart failure.
② Acute exacerbation of chronic heart failure:During the gradual worsening of heart failure, advanced heart failure is often characterized byMultiple episodes of acute decompensation ((see the curve in Figure 2, “Trend of Heart Failure Deterioration”),Each episode may be caused by multiple factors., these patients often have high-risk factors for heart failure (e.g., hypertension or ischemic cardiomyopathy). Sixty-five percent of hospitalized heart failure patients have known heart failure but are not in a state of end-stage or refractory heart failure.[7, 8, 9]。
③ End-stage heart failure:It accounts for approximately 5% of all hospitalized heart failure patients. These patients are refractory to standard pharmacological therapies, including ACE inhibitors and inotropic-diuretic regimens, and exhibit symptoms that limit their activities of daily living.
The 2019 National Report on Medical Services and Quality Safety (based on data from the National Clinical Quality Control Information System [NCLS] and the National Hospital Quality Monitoring System [HQMS], which collected face sheet data from 295,230,818 inpatient medical records across 1,861 tertiary hospitals and 2,151 secondary hospitals between 2016 and 2018) showed that the number of discharges for heart failure patients in general hospitals nationwide was 2,830,134 (sampled from 1,272 tertiary general hospitals with a total of 67,305,874 discharges) and 832,548 (sampled from 1,680 secondary general hospitals with a total of 26,441,935 discharges). The average length of stay ranged from 8.96 to 9.64 days, and the cost per hospitalization ranged from RMB 7,211.68 to RMB 12,092.71.[10]In 2019, the number of discharges from tertiary hospitals in China was 104,830,000, and from secondary hospitals was 83,800,000. Based on this, it is estimated that the total number of heart failure discharges in China in 2019 was approximately 7,046,498.In China, there are approximately 5.99 million hospitalizations for acute exacerbation of chronic heart failure and about 350,000 patients with end-stage heart failure. Furthermore, the number of cases involving the primary causes of acute de novo heart failure—namely, acute myocardial infarction and high-risk percutaneous coronary intervention (PCI)—exceeds one million.
Acute Heart Failure (acute heart failure, AHF)It refers to symptoms and signs that develop or worsen rapidly secondary to cardiac dysfunction. It can present as an acute onset (e.g., acute myocardial infarction complicated by acute heart failure) or as acute decompensated heart failure (ADHF) in the setting of chronic heart failure, with the latter being more common, accounting for approximately 70%–80%. As shown in Figure 2, most patients with chronic heart failure in the progressive stage often experience exacerbations due to various precipitating factors (such as arrhythmias, respiratory tract infections, etc.).Recurrent Hospitalizations Due to Acute ExacerbationsTreatment—Acute exacerbation of chronic heart failure: In most cases, symptoms are partially alleviated after treatment, and the condition reverts to the course of chronic heart failure. Acute heart failure (AHF) is a common emergency that is often life-threatening. For patients with suspected AHF, rapid diagnosis and emergency resuscitation must be initiated; pharmacological and device-based therapies (such as ventricular assist devices, VAD) should be commenced concurrently with diagnostic workup.
AHF has the following characteristics:
●High Mortality and High Readmission Rates: AHF carries a poor prognosis, with an in-hospital mortality rate of 3%, a 6-month readmission rate of approximately 50%, and a 5-year mortality rate as high as 60%. In China, the mortality rate among patients hospitalized for acute heart failure is 3.2% during hospitalization or within 3 days after discharge, and the mortality rate from day 4 post-discharge until the first follow-up visit isThe readmission rate was 22.4%. Within 30 days of hospitalization for acute heart failure, 2% of patients experienced cardiac sudden death, cardiopulmonary resuscitation, or ventricular tachycardia/ventricular fibrillation.[11]。
● Frequency of Episodes——Once heart failure progression necessitates hospitalization, the frequency of hospital admissions increases.: A study analyzing data on patients newly diagnosed with chronic heart failure between 1987 and 2006 found that,5 YearsDuring the follow-up period, 1,077 patients underwent 4,359 hospitalizations. Eighty-three percent of the patients were hospitalized at least once.67% Multiple Hospitalizations. Moreover, the more frequent the hospitalizations for heart failure, the significantly higher the probability of readmission and subsequent hospitalizations. Patients hospitalized for any reasonThe readmission rate within one year is 60%-69%.. Among heart failure patients who have undergone two or more hospitalizations, 60% are rehospitalized within one year; of these, 90% are due to cardiovascular diseases, and 60% are caused by heart failure.[12, 13]。
● Severity——Mortality Risk Increases with Each Hospitalization for Heart Failure: Hospitalization for heart failure patients is itself a marker of disease worsening, thereby increasing the risk of mortality and early readmission.[11, 14, 15, 16], the mortality rate among hospitalized heart failure patients was 5.22 times that of non-hospitalized patients (P<0.001)[14]. Analysis of the Canadian health insurance database shows that among patients hospitalized for heart failure, each readmission leads to an increased mortality rate[16]. For patients with chronic heart failure seen in outpatient clinics, hospitalization due to disease exacerbation significantly increases mortality. It is an established fact that mortality among heart failure patients rises with each hospital admission, regardless of whether they have systolic or diastolic heart failure.
The clinical manifestations of acute heart failure (AHF) are characterized by various symptoms and signs of pulmonary congestion, systemic circulatory congestion, and hypoperfusion of tissues and organs, complicated by cardiogenic shock. The treatment goals for AHF vary according to the different stages of heart failure; during the early emergency resuscitation phase, the focus is onRapidly Stabilize Hemodynamic Status, correct hypoxia, improve symptoms,Maintain perfusion and function of vital organs- The primary treatment goal is the prevention of thromboembolism; in the subsequent phase, further clarification of the etiology and precipitating factors of heart failure should be pursued to provide appropriate management, control symptoms and congestion, optimize blood pressure, develop a follow-up plan, and improve long-term prognosis.The principle of AHF treatment is to reduce cardiac preload and afterload., improve cardiac systolic and diastolic function, actively eliminate precipitating factors, and treat the underlying pathology.
VAD Clinical Need Segmentation
VThe principle of AD dictates that clinical application requires a comprehensive consideration of flow rate, duration, and trauma:The normal cardiac output in humans is approximately 4 L/min. Due to differences in operating principles, common ventricular assist devices (VADs) are categorized into partial-flow (2–3 L/min) and full-flow (>4 L/min) support systems. In the event of heart failure, a sudden drop in cardiac output necessitates circulatory support. The suitability of VAD access routes varies between medical and surgical patients based on their respective inflow conditions. There are three common scenarios:
Acute heart failure is a common clinical scenario (see Figure 5).: ① During the progression of chronic heart failure, even in its early stages, concurrent respiratory tract infections can precipitate acute heart failure episodes. ② In patients with sudden cardiovascular events such as acute myocardial infarction, or in those with specific high-risk coronary artery disease lesions (e.g., severe stenosis of the left main trunk or the proximal segments of the left anterior descending and circumflex arteries), balloon dilation during percutaneous coronary intervention (PCI), also known as high-risk PCI, may cause extensive left ventricular ischemia leading to cardiogenic shock. ③ Low cardiac output syndrome following cardiac surgery. ④ Among patients awaiting heart transplantation, pre-transplant optimization of overall cardiac function is required, necessitating the use of extracorporeal ventricular assist devices (VADs) for cardiac support. ⑤ Acute cardiac dysfunction resulting from various emergencies, such as trauma.
When a patient retains partial cardiac pumping function but it is insufficient to meet the perfusion requirements of systemic organs, short-term (less than one week) half-flow support is adequate to fulfill the patient’s circulatory assistance needs. This scenario is commonly seen in cases caused by various etiologies.Emergency Treatment of Acute Heart Failure, Prevention of Shock in Acute Myocardial Infarction, or Emergency Treatment of Shock. Due toFirst-line ResuscitationCommonly seen in internal medicine and emergency departments, the percutaneous approach for femoral artery puncture is, in terms of operational simplicity, suitable for almost all clinicalThe Procedure with the Lowest Entry Barrier in the Department, the most suitable application isInterventional VAD (e.g., Impella). It should be noted that although the intra-aortic balloon pump (IABP) commonly used in China can increase coronary and cerebral blood supply through counterpulsation, its flow rate is only tens of milliliters, which is insufficient to maintain organ perfusion when shock occurs. In cases of acute cardiac output insufficiency, if vital organs are notTimely maintenance of blood perfusion is critical, as cardiorenal syndrome can lead to acute renal hypoperfusion, thereby causing acute kidney injury (AKI) and directly affecting patients' short- and long-term outcomes.
From a clinical perspective, rapid circulatory intervention should be initiated as soon as possible, with earlier intervention associated with better patient outcomes. Recent trends in clinical guidelines indicate that the timing of short-term ventricular assist device (VAD) intervention is increasingly shifting toward first-line use, evolving from deployment at the onset of shock to prophylactic use in high-risk percutaneous coronary intervention (PCI), and further toward first-line prophylaxis in ST-elevation myocardial infarction (STEMI).The 2013 JACC Heart Failure Treatment Guidelines state that percutaneous or extracorporeal ventricular assist devices may be used as short-term mechanical circulatory support for patients with HFrEF experiencing acute, severe hemodynamic compromise (Class IIa); the 2011 ACCF/AHA/SCAI Guidelines for Percutaneous Coronary Intervention and the 2015 SCAI/ACC/HFSA/STS Clinical Expert Consensus on the Use of Percutaneous Mechanical Circulatory Support in Cardiovascular Disease Management recommend their use for intra-procedural protection in high-risk PCI patients; and the 2018 ESC/EACTS Guidelines on Myocardial Revascularization recommend their use in patients with acute coronary syndrome and impaired cardiac function.
Due to Interventional VADThe percutaneous minimally invasive advantages bring interventional VADs closest to first-line therapyadvantages. Meanwhile, due to inherent physical limitations at the technical level, percutaneous ventricular assist devices (VADs) are unable to provide full-flow circulatory support for extended periods (longer than 7 days). This is because the human femoral artery has an anatomical upper limit on its diameter. When the blood pump is made small enough to be inserted into the femoral artery, the impeller at the pump head must be reduced in size (to a few millimeters). To maintain a flow rate exceeding 2 L/min with such a small impeller, the rotational speed typically exceeds 20,000 revolutions per minute, inevitably leading to hemolysis-related complications. Therefore, the advantages of percutaneous VADs lie in “emergency rescue” and “prevention.” In cases of acute heart failure or sudden shock occurring in clinical emergency settings, internal medicine wards, or interventional catheterization laboratories, percutaneous VADs can facilitate rapid resuscitation, allowing for subsequent treatment once the patient’s circulation has stabilized.
Percutaneous VADs utilize axial-flow rotary blood pump technology and can be implanted via catheter for short-term circulatory support. Currently, the only percutaneous VADs available on the market are Abiomed’s Impella series, which include the FDA- and CE-approved models 2.5, CP, 5.0, 5.5, and LD for clinical left ventricular assist, the RP model for right ventricular assist, and the next-generation ECP model currently in clinical trials. Two percutaneous VADs (Impella 2.5 and Impella CP) primarily target minimally invasive high-risk PCI protection and short-term treatment of cardiogenic shock. The Impella device directly reduces ventricular volume (preload) and increases systemic blood flow to a certain extent. Clinical trials have demonstrated that, after adjusting for disease severity, Impella provides more effective hemodynamic stabilization and is associated with higher survival rates compared with IABP.
Trends in Interventional VADs: Less Invasive, Faster Delivery, and Earlier Intervention
Since the FDA approved Impella for high-risk PCI indications in 2015–2016, its penetration rate and patient usage in the field of interventional cardiology have grown rapidly year by year. To date, the overall penetration rate of Impella in all PCI procedures has reached 19%, with a 34% penetration rate in high-risk PCI cases. Surveys of U.S. physicians indicate that both cardiologists and cardiac surgeons expect Impella to continue its rapid growth over the next two to three years, with its penetration rate projected to reach 27% of total PCI procedures. Among U.S. cardiologists, the proportion using Impella in high-risk PCI cases is as high as 64%, with standalone Impella use accounting for 57%, while the use of the traditional method, intra-aortic balloon pump (IABP), has shrunk to 28%.
In terms of industry development trends, interventional VADs are undergoing continuous technological iteration—Continued Miniaturization of Devices and Improved Blood Compatibility.The Impella ECP used in clinical trials is currently the smallest ventricular assist device in the world, with an insertion profile of only 9 Fr (3 mm). Its reduced size and simplified delivery system minimize vascular complications. The ECP pump head can expand to a diameter of 18 Fr within the aorta; as the impeller operates at a larger diameter, blood flow can exceed 3.5 L/min, significantly improving hemocompatibility.
Meanwhile, clinical research has progressively advanced with robust evidence-based medical support.Indication Expansionand VADEarlier Intervention TimingTwo recent pivotal studies are: ① PROTECT IV: Evidence from this clinical trial indicates that the target market for high-risk PCI has expanded by more than threefold. ② STEMI-DTU RCT: The ongoing STEMI DTU study is a prospective, multicenter, two-arm randomized controlled trial planning to enroll 668 patients undergoing treatment for ST-segment elevation myocardial infarction (STEMI). Preliminary data have shown that pre-reperfusion use of Impella reduces infarct size. Upon future approval for circulatory support in STEMI, the market is expected to expand further, capturing approximately 25% of the STEMI patient population.
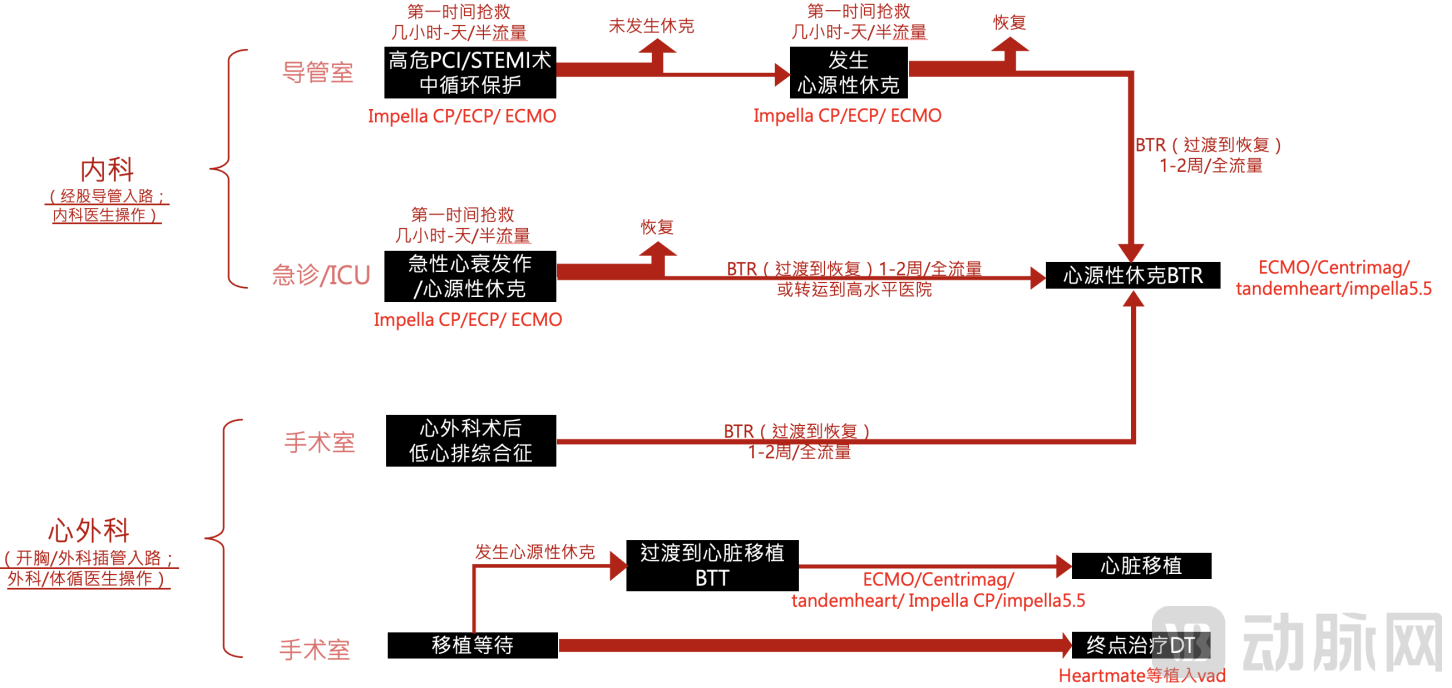
Figure 5. Segmentation of Clinical Needs and Patient Flow for VADs
When patients experience persistent low cardiac output and require an extended period (1 week to 1 month) for cardiac function recovery, bridging to full-flow support is often necessary. Common bridging therapies include Bridge-to-Recovery (BTR), Bridge-to-Decision (BTD), and Bridge-to-Transplant (BTT). BTR is commonly seen in cases such as fulminant myocarditis and low cardiac output syndrome following cardiac surgery. BTD is typically used in acute cases with unclear etiologies where patients have unstable circulation that cannot be restored quickly; it aims to stabilize hemodynamics, allowing clinicians sufficient time for further diagnosis and treatment. BTT is commonly employed to provide circulatory support for patients with poor cardiac function while awaiting a donor heart for transplantation.
Patients undergoing bridging transition are characterized by the inability of half-flow circulatory support to maintain systemic perfusion for extended periods. Due to the severity of their condition, these patients have high systemic flow requirements and heightened sensitivity to complications such as hemolysis. Therefore, they require prolonged, full-flow circulatory support with high blood compatibility to ensure normal organ function. It is important to note that bridging transition is also time-sensitive, particularly forThe timing of initiating circulatory support also has a critically important impact on patient prognosis.. For patients experiencing shock after cardiac surgery, if the time from initial weaning off cardiopulmonary bypass to the initiation of transitional circulatory support therapy exceeds 6 hours, the survival rate decreases from 44% to 14%.[5][17]。Early use of circulatory support devices is believed to improve patients' ultimate rates of weaning off support and hospital discharge.[4]. If circulatory support is established too late, it will lead to worsening disease severity and organ dysfunction, thereby reducing survival rates.[1][5][18][19]. If cardiac arrest has occurred in the patient prior to the initiation of short-term circulatory support, the patient’s survival rate decreases from 47% to 7%.[5][17]。
To ensure full-flow support, ventricular assist devices (VADs) require an enlarged impeller volume to enhance pumping efficiency. Meanwhile, to achieve prolonged support and high hemocompatibility, VADs must reduce impeller rotational speed and optimize flow pathways. Consequently, due to these mechanical principles, it is difficult to make mid-term VADs, which are responsible for bridging therapy, as compact as percutaneous VADs; their cannulation method is similar to that of extracorporeal membrane oxygenation (ECMO). However, because VADs can unload the left ventricle, they significantly facilitate the recovery of cardiac function in patients with heart failure. Compared with long-term VADs (implantable VADs), most patients requiring short-term bridging will either recover or proceed to other subsequent treatments. Therefore, in this intermediate transitional phase, the traumatic cost of open-chest implantation and the exceptionally high out-of-pocket expenses are key factors comprehensively considered in clinical decision-making.
Currently, most extracorporeal artificial hearts on the market are centrifugal rotary blood pumps. To continuously optimize and address hemolysis caused by mechanical support points of the impeller, the technology has undergone multiple iterations, with the latest generation of extracorporeal ventricular assist devices (VADs) utilizing magnetic levitation technology. Magnetically levitated blood pumps eliminate mechanical contact while ensuring a controllable and sufficiently large blood flow gap between the rotor and other components. This reduces damage to blood cells caused by the moving impeller rotor, thereby enhancing the safety of long-term circulatory support related to hemocompatibility. Extracorporeal VADs represented by Abbott’s CentriMag can provide various forms of intermediate-term circulatory support for up to 30 days. Other commonly used clinical VADs for intermediate-term support include ECMO, Impella 5.0/5.5, and TandemHeart.
When chronic heart failure progresses to the end stage and patients are awaiting heart transplantation, implantation of a long-term ventricular assist device (VAD) may be considered if they are ineligible for transplantation, or due to donor shortage or excessively long waiting times. Although heart transplantation is an effective treatment for end-stage heart failure, the scarcity of donors spurred the development of the earliest VADs. In recent years, clinical study data have shown that the clinical outcomes of long-term VADs approach the long-term survival rates associated with heart transplantation. Consequently, the use of long-term VADs as an alternative therapy or as destination therapy (DT) for end-stage heart failure has gradually become their primary indication.
Trends in Implantable VADs: Long-Term Assist Support and Destination Therapy
Heart transplantation is an effective treatment for end-stage heart failure. However, due to a shortage of donors, only approximately 5,000 heart transplant procedures are performed worldwide each year, with over 2,000 conducted annually in the United States. In China, donor availability is even more limited, with fewer than 500 transplants currently performed each year. The performance of a ventricular assist device (VAD) primarily depends on the bearing mechanism supporting the rotor within the blood pump. Evolution has progressed from early pulsatile pumps to second-generation devices featuring mechanical contact bearings (e.g., Abbott’s HeartMate II) or hydrodynamic bearings (e.g., Medtronic’s HVAD), and finally to third-generation fully magnetically levitated systems (e.g., Abbott’s HeartMate 3).
With technological iterations, there has been a significant improvement in long-term patient survival rates and quality of life. According to clinical statistics, the current three-year survival rate for patients with the HeartMate 3 exceeds that of heart transplantation, with higher survival rates observed during the first three years compared to transplant recipients. Due to its third-generation fully magnetically levitated technology pathway, the device demonstrates markedly improved blood compatibility compared to second-generation pumps. The incidence of long-term adverse events, particularly thrombus-related neurological complications caused by the blood pump (which led to the recall of Medtronic’s HVAD in 2021), has shown a downward trend. In 2018, the HeartMate 3 already accounted for the majority (80%) of VAD implants in the market. However, given the nature of long-term implantation, patient management remains critical; currently, the primary complication—percutaneous driveline infection—remains an unresolved challenge.
Iterative aspects among indications,Long-term implantation (DT) is gradually becoming the mainstream treatment for end-stage heart failureWith continuous advancements in medical management, patient selection, and technology, the indications for ventricular assist device (VAD) products have gradually evolved from serving as a bridge to transplant (BTT) to becoming a long-term implantable alternative therapy, establishing themselves as the definitive treatment for heart failure patients and gaining increasing acceptance among surgeons and patients alike.
References:
[1]. MosterdA,HoesAW. Clinical epidemiology of heart failure[J]. Heart, 2007,93(9):1137-1146. DOI: 10.1136/hrt.2003.025270.
[2]. Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics – 2014 update: a report from the American Heart Association. Circulation. 2014;129(3): e28-e292.
[3]. Senni M, Tribouilloy CM, Rodeheffer RJ, et al. Congestive heart failure in the comminity: trends in incidence and survival in a 10-year period. Arch Intern Med. 1999;159(1):29-34.
[4]. Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statstics-2013 update: a report from the American Heart Association. Circulation. 2013;127(1): e6-e245.
[5]. Gu Dongfeng, Huang Guangyong, He Jiang, et al. Epidemiological survey and prevalence of heart failure in China[J]. Chinese Journal of Cardiology, 2003, 31(1): 3-6. DOI: 10.3760/j:issn.0253-3758.2003.01.002.
[6]. Zhang Y, Zhang J, Butler J, et al. Contemporary epidemiology, management, and outcomes of patients hospitalized for heart failure in China: results from the China heart failure (China-HF) registry[J]. J Card Fail, 2017,23(12):868-875. DOI: 10.1016/j.cardfail.2017.09.014.
[7]. Fonarow GC, Heywood JT, Heidenreich PA, Lopatin M, Yancy CW; ADHERE Scientific Advisory Committee and Investigators. Temporal trends in clinical characteristics, treatments, and outcomes for heart failure hospitalizations, 2002 to 2004: findings from Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J. 2007; 153(6): 1021 – 1028. [PMID: 17540205]
[8]. Cleland JG, Swedberg K, Follath F, et al.; Study Group on Diagnosis of the Working Group on Heart Failure of the European Society of Cardiology. The EuroHeart Failure survey programme – a survey on the quality of care among patients with heart failure in Europe. Part 1: Patient characteristics and diagnosis. Eur Heart J. 2003; 24(5): 442 – 463. [pmid: 12633546]
[9]. Castro P, Vukasovic JL, Garces E, Sepulveda L. Ferrada M, Alvarado S; Insuficiencia Cardiaca: Registro y Organization. Cardiac failure in Children hospitals: Results of the National Registry of Heart Failure, ICARO. Rev Med Chil. 2004; 132(6): 655 – 662. [PMID: 15332366]
[10]. National Health Commission of the People’s Republic of China. National Report on the services, Quality and Safety in Medical Care System [M] . Beijing: Scientific and Technical Documentation Press, 2019
[11]. O'Connor C, Abraham W, Albert N, et al. Predictors of mortality after discharge in patients hospitalized with heart failure: An analysis from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). Am Heart J. 2008; 156: 662 - 673.
[12]. Krumholz H, Wong Y, Paretn E, et al. Quality of care for elderly patients hospitalized with heart failure. Arch Intern Med. 1997; 157: 2242 – 2247.
[13]. Gorelik O, Almoznino-Sarafian D, Shteinshnaider M, et al. Clinical variables affecting survival in patients with decompensated diastolic versus systolic heart failure. Clin Res Cardiol. 2009; 98: 224 – 232.
[14]. Ahmed A, Allman R, Ponarow G, et al. Incident heart failure hospitalization and sub-sequent mortality in chronic heart failure: a propensity-matched study. J Card Fail. 2008; 14: 211 – 218.
[15]. Setoguchi S, Warner-Stevenson L. Hospitalizations in patients with heart failure: who and why. J Am Coll Cardiol. 2009; 54: 1703 – 1705.
[16]. Setoguchi S, Stevenson L. Schneeweiss S. Repeated hospitalizations predict mortality in the community population with heart failure. Am Heart J. 2007; 154: 260 – 266.
[17]. Chinese Society of Cardiology, Chinese Medical Association. Retrospective survey of hospitalized cases with chronic heart failure in selected regions of China in 1980, 1990, and 2000[J]. Chinese Journal of Cardiology, 2002, 30(8):450-454. DOI: 10.3760/j:issn:0253-3758.2002.08.002.
[18]. National Centre for Cardiovascular Diseases, China. Report on Cardiovascular Diseases in China [M] . Beijing: Encyclopedia of China Publishing House, 2018
[19]. Li L, Liu R, Jiang C, et al. Assessing the evidence‐practice gap for heart failure in China: the Heart Failure Registry of Patient Outcomes (HERO) study design and baseline characteristics [J]. Eur J Heart Fail, 2020, 22 (4): 646-660. DOI: 10.1002/ejhf.1630.
Author Introduction
Dr. Chen Yang, a participant in the CCI Phase II program and a CCI Gold Mentor. He previously oversaw investments in innovative medical devices at Northern Light Venture Capital, bringing over a decade of experience in clinical practice and early-stage healthcare investment. Prior to entering the investment field, Dr. Chen worked for many years on the clinical front lines at Fuwai Hospital, National Center for Cardiovascular Diseases, and Beijing Anzhen Hospital, accumulating extensive clinical expertise and industry resources. He has participated in several international multicenter academic studies and large-scale clinical trials of cardiovascular devices, as well as the early research and development of multiple innovative medical devices. Dr. Chen also serves as an entrepreneurial mentor at several domestic clinical translation centers, providing guidance on track selection from scratch, strategic direction, and device R&D consultation, with a commitment to fostering China’s local medical device innovation driven by clinical needs. Dr. Chen holds a Doctor of Medicine degree from Peking Union Medical College.