Four Years of China's National Healthcare Security Administration: 124 Policies Implemented, RMB 800 Billion Saved – What’s Next?
On January 26, the National Healthcare Security Administration released the latest data on the direct settlement of cross-provincial medical expenses for patients seeking care outside their home provinces. Notably, significant progress has been made in the direct settlement of outpatient costs across provincial boundaries, a system that has been accelerated since 2021. As of the end of December 2021, there were 45,600 designated medical institutions and 82,700 designated pharmacies nationwide participating in the direct settlement program for cross-provincial outpatient expenses, with a cumulative total of 12.5144 million transactions processed. The improvement of this direct settlement mechanism for cross-provincial medical care will address the practical needs of 125 million people.
This far-reaching initiative is just one of many measures implemented by the National Healthcare Security Administration (NHSA) in the nearly four years since its establishment. At the recent National Healthcare Security Work Conference, the NHSA released its 2021 “report card,” presenting data-driven achievements in areas such as reducing patients’ financial burden for drugs and medical consumables, improving the experience of cross-provincial medical care, lowering epidemic prevention and control costs, and enhancing the quality of benefit coverage. A review of data announced at previous National Healthcare Security Work Conferences shows that the NHSA has saved patients at least RMB 800 billion in direct expenses, not including indirect costs spared through convenience measures such as cross-regional settlement.
Saving 800 billion yuan represents a phased achievement of the National Healthcare Security Administration’s strategic planning, and inevitably, more “small targets” will follow.
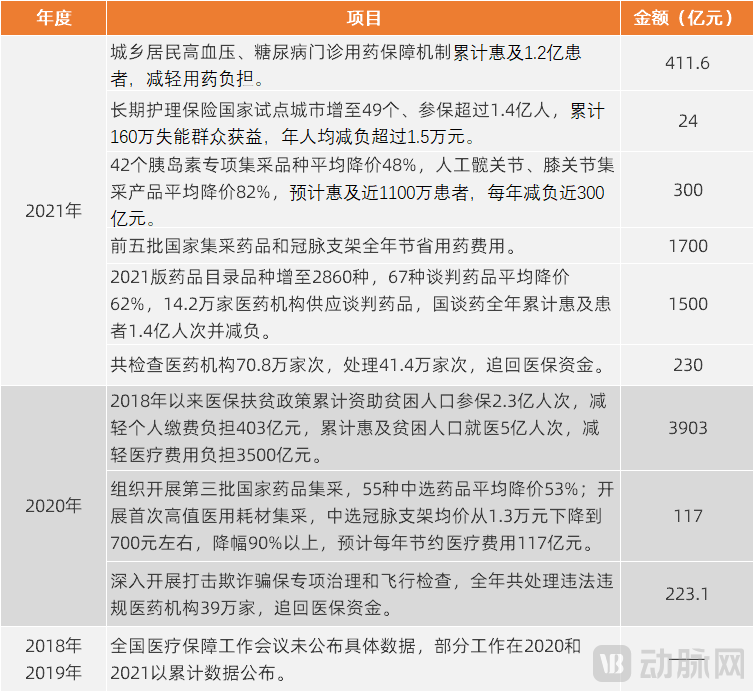
Key Data Released at National Healthcare Security Administration Work Conferences Over the Years, Source: Official Website of the National Healthcare Security Administration
First, let us examine the significant measures that the National Healthcare Security Administration has implemented over the past four years to alleviate the financial burden on patients and the general public.
Regularized Centralized Procurement and Price Negotiations Alleviate the Burden of Drug and Consumable Costs
On January 26, the volume declaration phase for the seventh round of National Centralized Drug Procurement commenced, marking the launch of the new year’s centralized procurement initiatives. Prior to this, from the initiation of the “4+7” pilot program in 2018 through the end of 2021, the National Healthcare Security Administration had organized six rounds of national centralized drug procurement. In 2020, the scope of national centralized procurement expanded from pharmaceuticals to medical consumables, with procurement programs already implemented for items such as coronary stents and artificial joints.
As of the end of 2021, the centralized procurement of drugs and medical consumables had cumulatively saved more than RMB 260 billion in expenditures for the basic medical insurance fund and patients.
Since the establishment of the National Healthcare Security Administration, a normalized mechanism for negotiating the inclusion of drugs in the national medical insurance catalog has been established. From 2018 to present, China has carried out adjustments to the National Medical Insurance Drug Catalog for four consecutive years, cumulatively adding 507 new and high-quality drugs to the catalog. The average annual price reduction for negotiated drugs is approximately 50%-60%. According to statistics, the negotiated drugs over the first three years have reduced the financial burden on patients by RMB 170 billion.
In 2021, nusinersen sodium injection, the world’s first precision-targeted therapy for spinal muscular atrophy (SMA), was included in the National Reimbursement Drug List (NRDL) through price negotiations, with the cost per dose dropping from RMB 700,000 to over RMB 30,000, significantly alleviating the financial burden on patients. A total of seven drugs for rare diseases were added to the updated NRDL during these negotiations. To date, the list includes 45 drugs for rare diseases, enabling an increasing number of patients with rare conditions to benefit directly.
Expanded Outpatient Coverage, Reduced Outpatient Expenditures
In the past, health insurance coverage was primarily focused on inpatient care, with limited outpatient coverage that relied mainly on out-of-pocket payments or personal health insurance accounts. In recent years, outpatient coverage has been gradually expanded.
Regarding urban and rural resident basic medical insurance, in 2019, the National Healthcare Security Administration and other departments issued the "Guiding Opinions on Improving the Outpatient Medication Reimbursement Mechanism for Hypertension and Diabetes among Urban and Rural Residents," which clarified that expenses for antihypertensive and hypoglycemic medications incurred by insured patients with these two conditions during outpatient visits shall be covered by the pooled fund, relying on designated primary healthcare institutions at Level II and below. The reimbursement rate within the policy scope shall exceed 50%.
Regarding employee basic medical insurance, in 2021, the General Office of the State Council issued the "Guiding Opinions on Establishing and Improving the Outpatient Mutual Aid Security Mechanism for Employee Basic Medical Insurance," which outlined two aspects of outpatient coverage planning: first, gradually including ordinary outpatient expenses for frequently occurring and common diseases within the scope of payment by the pooled fund, with the reimbursement rate starting at 50% for expenses within the policy scope, and appropriately favoring retirees in benefit payments; second, gradually expanding the range of chronic and special diseases covered by the pooled fund for outpatient care, with some conditions managed similarly to inpatient benefits.
Meanwhile, in addition to personal use, the individual account may also be used to cover out-of-pocket expenses incurred by the account holder’s spouse, parents, and children for medical care, as well as out-of-pocket costs for purchasing medicines, medical devices, and medical consumables at designated retail pharmacies.
Subsequently, multiple provinces across China, including Sichuan and Fujian, followed suit by issuing local policies for outpatient mutual aid under the employee basic medical insurance scheme, specifying reimbursement rates, coverage limits, and implementation timelines. These policies have been implemented to varying degrees across different regions, with certain differences in covered conditions and reimbursement ratios. Overall, the combination of two key measures—outpatient pooling payments and family sharing of personal account funds—aims to address gaps in outpatient coverage. This will facilitate a transition from self-insurance through personal accounts to mutual aid supported by pooled funds, thereby alleviating the financial burden on patients seeking outpatient care.
Direct Settlement for Cross-Provincial Medical Care: Higher Efficiency in Seeking Treatment
According to statistics, 125 million migrant workers across China have a need for cross-provincial settlement of medical expenses.
As early as 2016, the National Cross-Regional Medical Expense Settlement System was launched, enabling patients to gradually benefit from direct reimbursement for inpatient care across regions, thereby gaining significant convenience. However, cross-regional settlement remained unavailable for outpatient visits, which are utilized more frequently. Influenced by demographic mobility patterns, it has become increasingly common for retired elderly individuals to relocate to other cities to live with their children, creating a more urgent demand for cross-regional settlement of outpatient expenses.
In 2020, the National Healthcare Security Administration and the Ministry of Finance issued the Notice on Promoting the Pilot Program for Direct Interprovincial Settlement of Outpatient Expenses, proposing a pilot plan involving the Beijing-Tianjin-Hebei region, the Yangtze River Delta region, and five southwestern provinces. Concurrently, they formulated the Operational Procedures for Direct Interprovincial Settlement of Outpatient Expenses (Trial), which specified detailed settlement rules.
As previously mentioned, the outpatient care coverage system is being accelerated and improved, which also means that cross-regional settlement for outpatient services must keep pace. In 2021, the cross-provincial settlement of outpatient expenses was accelerated. Currently, direct cross-provincial settlement for general outpatient expenses has achieved full coverage across all pooling regions in China’s 31 provinces (autonomous regions and municipalities directly under the Central Government) and the Xinjiang Production and Construction Corps. Additionally, every province has at least one pooling region that has launched pilot programs for the direct cross-provincial settlement of expenses related to the treatment of chronic and special diseases.
As of the end of December 2021, there were 45,600 designated medical institutions and 82,700 designated pharmacies across China providing direct cross-provincial settlement for outpatient expenses, with a cumulative total of 12.5144 million direct settlements; among these, 9.496 million settlements were made in 2021 alone.
Nationwide direct cross-provincial settlement of inpatient expenses is also being steadily advanced. As of the end of December 2021, there were 52,700 designated medical institutions participating in such settlements, representing a year-on-year increase of 18.7%. In 2021, direct cross-provincial settlements for inpatient expenses nationwide totaled 4.4059 million cases, a year-on-year increase of 46.8%.
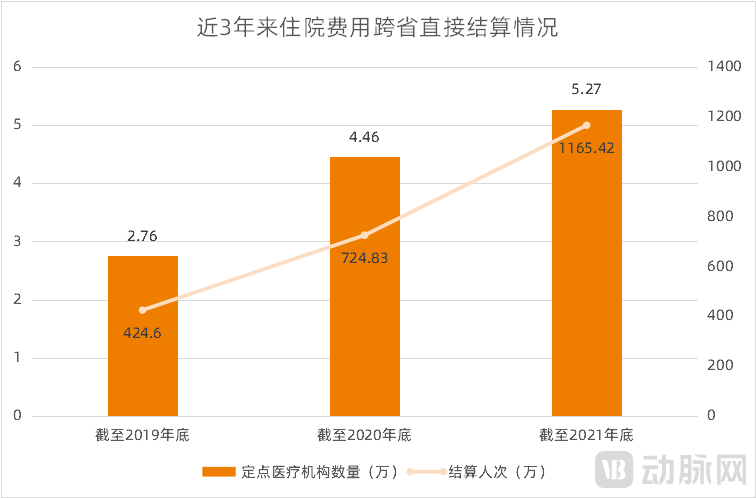
National Statistics on Direct Cross-Provincial Settlement of Inpatient Expenses (2019–2021, Cumulative Figures), Source: Official Website of the National Healthcare Security Administration
Measures such as centralized drug procurement, national reimbursement drug list negotiations, and outpatient pooling reimbursement directly reduce the financial burden on patients. In contrast, the direct settlement of cross-provincial medical expenses indirectly alleviates this burden by eliminating the need for patients to travel for reimbursement claims, achieved through institutional breakthroughs and technological improvements adapted to new patterns of population mobility.
Vaccines Are Free, While the Price of Nucleic Acid Testing Continues to Drop
Health insurance coverage for epidemic prevention and control is also closely related to the general public. During the pandemic, health insurance funds and fiscal authorities jointly covered the treatment costs for COVID-19 patients. In 2020, a total of RMB 2.84 billion in expenses for COVID-19 patients was settled, with health insurance paying RMB 1.63 billion.
Subsequently, sporadic COVID-19 outbreaks emerged in various regions across China. To ensure the parallel operation of socioeconomic activities and the “dynamic zero-COVID” strategy, nucleic acid testing and vaccination became the two most fundamental measures, with enormous demand.
Regarding nucleic acid testing, test kits were once in short supply during the early stages of the pandemic, with the price reaching RMB 260 per person. In June 2020, the Office of the National Healthcare Security Administration issued the Notice on Coordinating to Further Enhance COVID-19 Testing Capacity, improving pricing policies for testing services. In 2021, the National Healthcare Security Administration implemented three rounds of significant nationwide price reductions for nucleic acid testing. Currently, the prices for individual single-sample testing and pooled multi-sample testing have been reduced to no more than RMB 40 and RMB 10 per person, respectively. For individuals, nucleic acid testing has become a low-cost routine safeguard measure before and after travel, such as business trips, returning home, or visiting relatives.
Regarding vaccination, from late 2020 to late 2021, China administered over 2.9 billion doses of the COVID-19 vaccine. The COVID-19 vaccination was provided free of charge nationwide, with costs jointly covered by medical insurance and fiscal funds.
In fact, the basic medical insurance fund is primarily designated for treatment purposes and originally did not cover preventive services such as vaccination. However, according to the National Healthcare Security Administration, covering the costs of COVID-19 vaccines through medical insurance is a special measure taken in response to an exceptional situation. It mainly utilizes the accumulated surplus of the medical insurance fund, thereby neither affecting the current revenue and expenditure balance of the fund nor impacting beneficiaries’ access to medical care and reimbursement benefits.
The aforementioned measures demonstrate the effectiveness of medical insurance in alleviating individuals’ out-of-pocket healthcare expenses. Apart from pandemic prevention and control, all other measures have either become or are poised to become standardized practices with broad population coverage and substantial financial implications.
Building on these achievements, what is the next goal of the National Healthcare Security Administration? The “14th Five-Year Plan for National Medical Security” (hereinafter referred to as the “Plan”), issued by the General Office of the State Council in 2021, has charted the course. The Plan sets forth 15 development indicators across four areas: insurance coverage, benefit levels, refined management, and high-quality services.
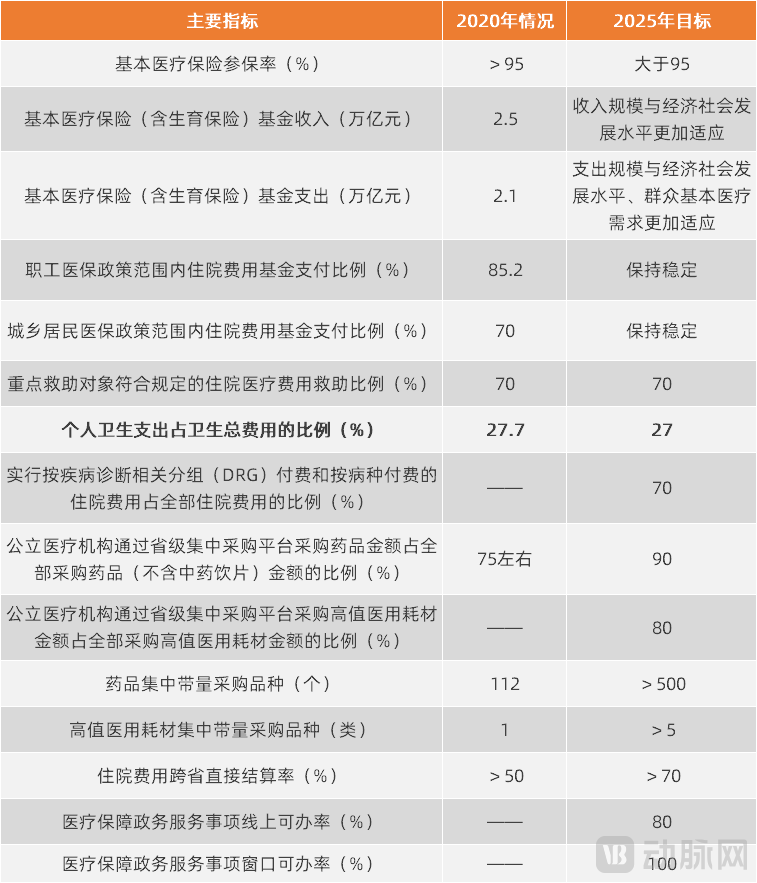
Key Indicators for the Development of National Healthcare Security During the 14th Five-Year Plan Period, Source: "14th Five-Year Plan for National Healthcare Security"
In the chart above, the variations among indicators highlight the key priorities for medical insurance initiatives. Specifically, the reduction in the share of out-of-pocket health expenditures in total health spending from 27.7% to 27% will result from the combined effects of other indicators, serving as an indirect reflection of the overall level of medical security. Guided by this overarching objective and considering other policies involving the National Healthcare Security Administration over the past four years, future medical insurance efforts will follow this pathway: expanding the funding pool, curbing expenditures, and optimizing payment methods, thereby enhancing coverage capacity.
1. Increase: Expand the funding pool
Regarding employee basic medical insurance, following the implementation of outpatient mutual aid coverage for payment purposes, a portion of the funds from individual accounts will be transferred to the pooled fund. According to statistics, the annual pooled fund will increase by approximately RMB 200 billion compared with previous years. These additional funds can be used to cover the outpatient reimbursement expenses mentioned above.
Regarding the basic medical insurance for urban and rural residents, premiums are composed of individual contributions and government subsidies. In recent years, the Government Work Report has included requirements to raise the fundraising standards for this insurance annually. Since its establishment, the National Healthcare Security Administration has implemented these measures each year, increasing the per capita government subsidy and individual contribution from RMB 490 and RMB 220 in 2018 to RMB 580 and RMB 320 in 2021, respectively. Going forward, the National Healthcare Security Administration will explore a more reasonable fundraising mechanism for resident medical insurance and optimize the structure of individual contributions and government subsidies.
Furthermore, both the “Opinions on Deepening the Reform of the Healthcare Security System” issued by the Central Committee of the Communist Party of China and the State Council, and the “14th Five-Year Plan for National Healthcare Security” emphasize the need to adapt to the development of new business formats and improve the enrollment and contribution mechanisms for flexibly employed workers. This measure not only serves to expand healthcare insurance coverage but also represents one of the channels for enlarging the funding pool.
1. Reduction: Compressing Medication Expenditure
Centralized procurement and price negotiations for pharmaceuticals and medical consumables remain a key approach to cost containment.
In accordance with the requirements of the “14th Five-Year Plan for National Healthcare Security,” by 2025, each province (autonomous region, and municipality directly under the Central Government) shall have no fewer than 500 varieties of drugs included in national and provincial centralized volume-based procurement; by 2025, each province (autonomous region, and municipality directly under the Central Government) shall have no fewer than five categories of high-value medical consumables included in national and provincial centralized volume-based procurement.
Recently, a national conference on centralized drug procurement was held. The meeting proposed that in 2022, centralized procurement should be comprehensively carried out across three major categories: chemical drugs, biological products, and traditional Chinese medicine (TCM) proprietary medicines, thereby establishing a multi-tiered, coordinated framework involving national-level, cross-provincial alliance, and provincial-level procurement. Regarding pharmaceuticals, building upon the nationally organized centralized procurement, each province must include no fewer than 100 varieties in its provincial-level centralized procurement. For medical consumables, while continuing to advance the nationally organized centralized procurement of high-value medical consumables, each province must include no fewer than seven varieties in its provincial-level centralized procurement, with key coverage of major high-value consumables in the cardiovascular and orthopedic fields. Specifically, drug-coated balloons and orthopedic trauma consumables must be included in the centralized procurement programs of all provinces. Guidance and support will be provided for the cross-provincial alliance-led centralized procurement of dental implants spearheaded by Sichuan Province; provinces not participating in this alliance are also required to independently carry out their own centralized procurement.
Drug price negotiations will advance in tandem with the development and market launch of new drugs in China, aiming not only to alleviate the financial burden on patients but also to synergistically promote innovation and transformation within the pharmaceutical industry.
1. Optimization: Accelerate the Implementation of Payment Method Reform
Payment method reform is not only a means of refined management for medical insurance, but also a measure to improve medical quality and avoid excessive medical treatment, thereby benefiting patients.
The “14th Five-Year Plan” for National Healthcare Security stipulates the nationwide implementation of a diversified, composite healthcare payment system dominated by diagnosis-related group (DRG) and disease-based payments. It advances reforms in regional global budgeting using a point-value system for healthcare security funds, guiding medical institutions toward rational diagnosis and treatment and enhancing the efficiency of healthcare security fund utilization. Specifically, by 2025, DRG-based and disease-based payments shall account for 70% of total inpatient expenses.
In fact, over the past few years, the National Healthcare Security Administration has spearheaded explorations into payment method reforms. However, due to the complexity of the reform measures and the large number of stakeholders involved, further progress is still needed to advance the reform agenda.
In 2021, the National Healthcare Security Administration issued the "Notice on Printing and Distributing the Three-Year Action Plan for DRG/DIP Payment Method Reform," promoting the in-depth development of DRG/DIP payment reform from partial to comprehensive coverage, from select groups to the entire population, and from extensive to refined management. More detailed arrangements were made for the reform progress from 2022 to 2024, demonstrating a stronger commitment to reform.
Therefore, the next three years will witness the rapid implementation of payment method reforms, with healthcare institutions being the most directly affected.
Enhance Coverage Capacity, Reduce the Share of Out-of-Pocket Expenses
The above measures create fiscal space through a strategy of “one increase, one decrease, and one optimization,” enabling the basic medical insurance fund to provide more comprehensive and in-depth coverage for insured individuals, thereby achieving the goal of reducing the proportion of out-of-pocket health expenditures.
Currently, outpatient coverage and direct settlement for cross-provincial medical care have achieved certain results in alleviating patients’ financial burden. However, due to significant variations in implementation across provinces and municipalities, both initiatives will continue to expand in terms of geographic coverage, participating medical institutions, and covered conditions, thereby benefiting more insured individuals. In accordance with the requirements of the 14th Five-Year Plan for National Healthcare Security, outpatient benefits will be steadily improved, ensuring coordinated integration between outpatient and inpatient benefits; furthermore, integrated online and offline direct settlement services for cross-regional medical care will be gradually realized for both inpatient and outpatient expenses.
It is worth noting that, as the aging process accelerates, long-term care insurance will become a key priority for the basic medical insurance system. In recent years, pilot programs for long-term care insurance have been implemented in selected regions. The National Healthcare Security Administration and the Ministry of Civil Affairs have jointly formulated the “Standards for Assessing Levels of Disability for Long-Term Care (Trial),” and a long-term care insurance system will be steadily established during the 14th Five-Year Plan period.
In previous pilot programs, the funding channels for long-term care insurance were similar to those for employee basic medical insurance, with costs shared by employers and employees. To avoid increasing the financial burden on employers during the pilot period, the employer’s contribution was directly transferred from the medical insurance funds already paid by the employer, without requiring an additional contribution rate. The individual’s share could be withheld and remitted from the personal accounts of the employee basic medical insurance. In other words, during the pilot period, funding was essentially reallocated from existing medical insurance funds. Given that these funds were already not “abundant,” this approach would not be sustainable in the long run. Therefore, during the pilot and implementation phases, long-term care insurance will establish diversified funding channels to achieve broader coverage.
In accordance with the requirements of the 14th Five-Year Plan for National Medical Security, efforts will be made to explore the establishment of a multi-channel financing mechanism characterized by mutual assistance and shared responsibility. For employees participating in long-term care insurance, funding will primarily come from contributions by employers and employees, thereby forming a dynamic adjustment mechanism for financing that aligns with economic and social development as well as the level of coverage. Social forces will be introduced to participate in the administration of long-term care insurance services. Commercial insurance institutions are encouraged to develop commercial long-term care insurance products.
Since the establishment of the National Healthcare Security Administration (NHSA) nearly four years ago, 124 policy documents have been formulated and gradually implemented. While these policies target different stakeholders—including insured individuals, hospitals, physicians, pharmaceutical and medical device companies, and IT firms providing technical support—the underlying logic among them is clear. As previously mentioned, this logic centers on achieving better coverage through a strategy of “one increase, one decrease, and one optimization.” Furthermore, the “14th Five-Year Plan” and the Outline of Long-Range Objectives Through the Year 2035 propose that basic public services should achieve equalization. As basic medical security is an integral part of basic public services, the term “equalization” implies more equitable coverage, ensuring that even patients with relatively rare conditions are included within the scope of coverage. It is foreseeable that “equalization” will become a key principle guiding reforms as the healthcare security system works toward reducing the proportion of out-of-pocket health expenditures.