Electroceuticals Revolutionize Disease Treatment: From Bioelectricity to Clinical Innovation
Electricity, hailed as one of the greatest discoveries in human history, has become the cornerstone of modern life, from electric lighting to the information superhighway. Yet its other role—bioelectricity—though vital to human survival, remains little known to the public.
There are no so-called "power plants" in the human body, yet electricity is generated everywhere. The carriers of bioelectricity are ions; their transmembrane migration generates electric currents and fields. The most intuitive manifestation of this phenomenon is in neural signal transmission, which explains our ability to respond rapidly to external stimuli. Furthermore, as research has deepened, the role of electricity has been revealed to extend into a complex network, influencing processes ranging from embryonic development, cell growth, and signal transduction to even playing a part in carcinogenesis.
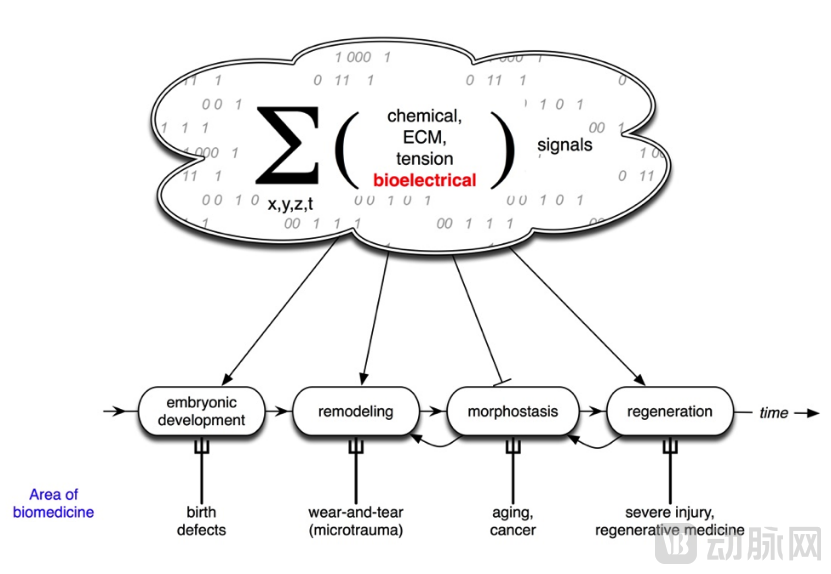
Partial Roles of Bioelectricity in the Human Body
Reference: Wikipedia, bioelectricity, https://fr.other.wiki/wiki/Bioelectricity
Furthermore, with the development of biomedical engineering, an increasing number of cross-disciplinary collaborations between electrical engineering and medicine are emerging. The most mature and widely applied example is the cardiac pacemaker, which utilizes low-frequency electric fields to assist cardiac contraction, making it one of the cornerstone therapeutic devices in cardiology. An example utilizing medium-frequency electric fields is Tumor Treating Fields (TTFields), a dark horse in oncology therapy. The most common device employing high-frequency electric fields is radiofrequency ablation, which destroys pathological tissue through substantial heat generation and is frequently used in patients with tumors and arrhythmias. Hailai Xinchuang is the first company in China and the second globally to enter the multicenter clinical trial stage for TTField research and development. In addition to destructive ablation, another important application of high-frequency electric fields is Deep Brain Stimulation (DBS), also known as a “brain pacemaker.”

Examples of Medical Engineering Devices Utilizing Electrotherapy
Deep brain stimulation (DBS) originally originated from the treatment of psychiatric disorders. In 1948, Lawrence Pool, a neurosurgeon at Columbia University, attempted to implant electrodes into the caudate nucleus of a woman suffering from depression and anorexia nervosa, reporting “good” therapeutic effects in the following weeks, although the electrodes were subsequently damaged. Subsequently, neurophysiologists and psychiatrists continuously applied chronic electrical neuromodulation techniques to the treatment of psychiatric disorders, pain, neurodegenerative diseases, and movement disorders, successfully laying the foundation for the further development of DBS.
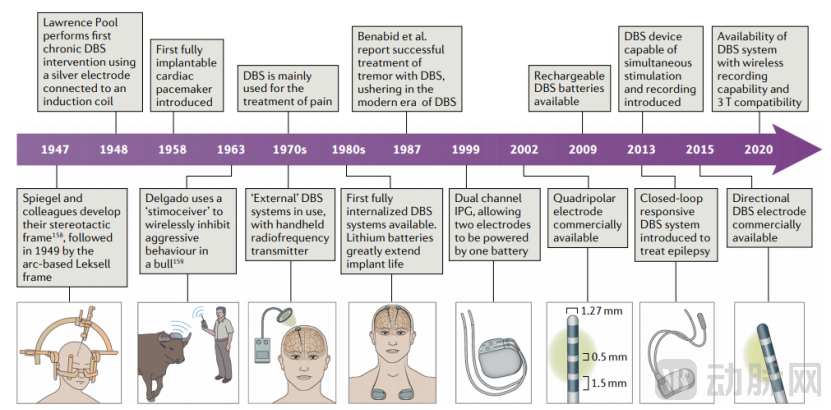
Timeline of Major Events in the Evolution of DBS Technology
In principle, DBS utilizes implanted electrodes to deliver electrical pulses to specific brain regions, thereby modulating specific cellular activity and substance transport, and inhibiting abnormal firing of nuclei. There are five main hypotheses regarding its specific mechanisms: 1) Depolarization block hypothesis (inactivation of action potential generation in efferent outputs); 2) Neural interference hypothesis; 3) Synaptic inhibition hypothesis (depletion of neurotransmitters at the terminals of efferent outputs); 4) Synaptic modulation hypothesis (activation of inhibitory or excitatory neuronal terminals in efferent outputs); 5) DBS-astrocyte hypothesis (prolongation of neurotransmitter release pathways involving astrocytes).
The DBS system comprises intracranial stimulation electrodes, subcutaneous extension leads, an implantable pulse generator (IPG), and a magnetic switch. The stimulation electrodes are made of platinum-iridium, offering excellent biocompatibility and electrical conductivity. Each electrode features four contacts, with a diameter of 1.27 mm and inter-contact spacing of either 0.5 mm or 1.5 mm; various configurations have been developed. The pulse generator is the device that delivers electrical pulses. Since the advent of early external pulse generators, the technology has evolved to include implantable pulse generators (IPGs), which can be surgically implanted in the subcutaneous tissue of the chest. The introduction of IPGs has posed significant challenges for battery life. Early batteries typically lasted approximately 3–4 years and required surgical replacement. However, rechargeable IPGs have now been developed, further enhancing the clinical convenience of DBS therapy.
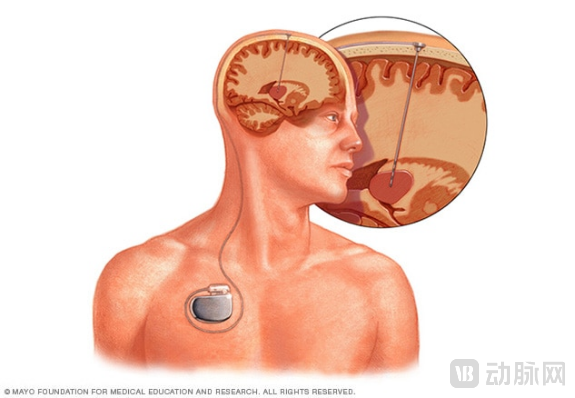
Schematic Diagram of a Brain Pacemaker
Source: Mayo Clinic,https://www.mayoclinic.org/tests-procedures/deep-brain-stimulation/about/pac-20384562
1. Clinical Practice of DBS
Deep Brain Stimulation (DBS) is currently primarily used to treat patients with mid-to-late stage Parkinson’s disease and dystonia, and has also been explored in the management of psychiatric disorders such as depression, obsessive-compulsive disorder, and anorexia nervosa. DBS implantation relies on stereotactic techniques, requiring intraoperative electrophysiological monitoring and intraoperative testing after lead placement. For patients with Parkinson’s disease and dystonia, the therapeutic effects of DBS are often immediate. Following postoperative cranial imaging to confirm the accuracy of lead positioning, the attending physician can remotely adjust stimulation parameters using specialized software.
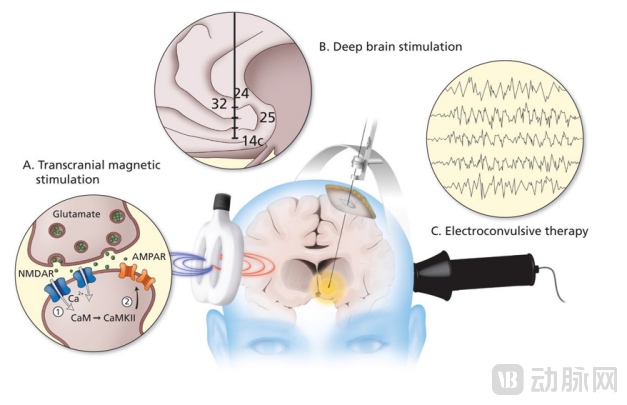
Neuroelectrical Modulation Therapies for Treatment-Resistant Depression
Currently, FDA-approved indications for deep brain stimulation (DBS) include Parkinson’s disease, essential tremor, dystonia, obsessive-compulsive disorder (OCD), and epilepsy. For patients with Parkinson’s disease, ideal candidates are those exhibiting fluctuating motor symptoms and intolerance or resistance to medication; target sites include the globus pallidus pars interna (GPi), subthalamic nucleus (STN), and the ventral intermediate nucleus (VIM) of the thalamus. The target area for dystonia is the GPi; compared with patients with Parkinson’s disease or essential tremor, those with dystonia may exhibit a delayed response, and DBS is less effective in patients with secondary dystonia. For OCD patients, Level I evidence supports the STN as the target region, while Level II evidence supports stimulation of the ventral striatum. Regarding epilepsy treatment, the FDA approved DBS in 2018 as an adjunctive therapy for drug-resistant epilepsy, with particularly favorable outcomes in patients with focal seizures.
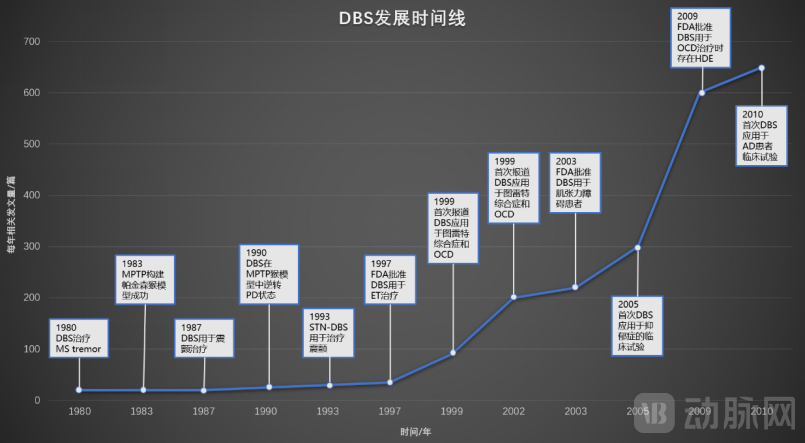
DBS Development Timeline
AD, Alzheimer's disease; ET, essential tremor; HDE, Humanitarian Device Exemption; MPTP, 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine; PD, Parkinson's disease; STN-DBS, subthalamic nucleus deep brain stimulation
Given that deep brain stimulation (DBS) is a long-term implantable device, multiple factors can significantly impact patients’ quality of life. The primary design concept of DBS was modeled after cardiac pacemakers; consequently, there were no breakthrough advancements for a considerable period after entering the “modern DBS” era in the 1980s. Nevertheless, DBS still faces limitations such as bulky battery size, limited battery lifespan necessitating frequent replacements, and lack of feedback information from stimulation electrodes. Furthermore, programming capabilities require further development. Concerns also remain regarding potential effects on patients’ cognitive functions, as well as risks of information leakage from implanted devices or even hijacking by malicious actors (“brainjacking”).
Building on current devices, we can further look ahead to the future development of medical equipment:
1) Electrode and IPG Design: Further miniaturization and cranial implantation are required, preferably with wireless power transfer capabilities. Modern mass production should be implemented to reduce costs. Additionally, battery life must be extended and charging efficiency optimized to avoid frequent surgical replacements.
2) Safety: Enhanced compatibility with MRI systems of 3T and above, built-in sustained-release antibiotics for infection prevention, and protection against data leakage and brainjacking;
3) Optimization of stimulation methods: Multiple implantable pulse generators (IPGs) are implanted to achieve multi-channel independent current control, enhance modulation of waveform shapes, and coordinate the frequency and inter-pulse intervals of different electrical pulses to improve control intensity;
4) Improve closed-loop design: Design probes to collect patient electrophysiological information, and achieve feedback regulation by integrating information and using artificial intelligence technology;
5) Enhancing targeting precision using neuroimaging techniques: Discovering specialized sequences or employing 7T MRI to improve local anatomical resolution, refining image processing software, and exploring optimal target characteristics for DBS implantation through prospective functional imaging.
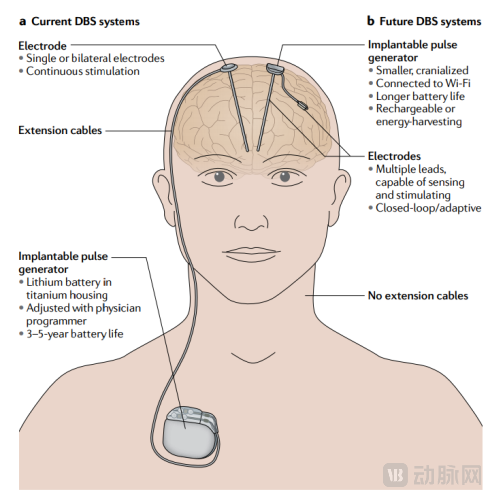
Future Design Outlook for DBS
Since the first global deep brain stimulation (DBS) surgery was performed in 1987, this therapy has been approved for the treatment of Parkinson’s disease, dystonia, essential tremor, and drug-resistant epilepsy. It also shows broad prospects in the exploration of psychiatric disorders such as refractory obsessive-compulsive disorder and depression. Taking Parkinson’s disease as an example, it is a common neurodegenerative disorder that predominantly affects the elderly, with symptoms typically manifesting as tremors, muscle rigidity, masked facies, and shuffling gait. DBS therapy can significantly alleviate patients’ symptoms, and its efficacy has been widely validated worldwide.
Medtronic was the first medical device company to conduct research on deep brain stimulation (DBS) devices. For a long time, the DBS market was monopolized by foreign companies. However, in recent years, with continuous innovation and breakthroughs by domestic enterprises such as Jingyu Medical and PINS Medical, the original monopoly pattern is gradually being broken. Founded in 2012, Jingyu Medical has achieved significant breakthroughs in treating diseases such as Parkinson’s disease and drug addiction, leveraging its years of experience in DBS technology research. In 2014, Jingyu Medical’s DBS device for treating Parkinson’s disease was included in the special approval channel for innovative medical devices by the National Medical Products Administration. PINS Medical, established in 2008, has built a collaborative innovation model integrating “industry, academia, research, and clinical practice” through partnerships with numerous clinical institutions, including Tsinghua University, Beijing Tiantan Hospital, and Peking Union Medical College Hospital. Both companies have received support from Hillhouse Investment, which has also accelerated the R&D efficiency of domestically produced DBS devices.
Tens of thousands of patients in China have already benefited from domestically developed deep brain stimulation (DBS) devices. Both in terms of device R&D and clinical practice, China has accumulated experience at the international forefront. Moreover, research teams continue to develop and optimize China’s self-developed DBS systems to better serve the general public.
The journey of deep brain stimulation (DBS) from early exploration to invention and the achievement of breakthrough clinical efficacy serves as a highly instructive case. First, “cross-disciplinary” research is currently a prominent trend. As components of the material world, human beings strictly adhere to physical laws; therefore, to some extent, the human body can be abstracted as a mechanical system and “repaired” through specific interventions. For instance, ultrasound can be used to modulate the opening and closing of the blood-brain barrier, thereby influencing the efficiency of substance transport, or stents can be employed to support narrowed blood vessels. The improvement in disease states achieved by such external devices is both significant and visibly evident.
However, another key insight from the development of deep brain stimulation (DBS) devices is the long development cycle and the significant challenges in research and development. On one hand, the discovery of therapeutic efficacy is often serendipitous rather than predictable. For instance, when DBS was first boldly attempted in patients with psychiatric disorders, no one could have foreseen its current achievements. Similarly, Tumor Treating Fields (TTFields) evolved from an accidental observation of electric fields inhibiting bacterial growth to becoming recognized as the "fourth modality" of cancer treatment—a transition that was equally unforeseeable. Furthermore, given that medical devices directly impact patient safety, they are subject to rigorous, multi-layered regulatory scrutiny. Beyond therapeutic efficacy, considerations such as clinical feasibility and patients' quality of life necessitate continuous optimization. This process demands substantial effort and large-scale R&D teams, which precisely underscores the value of deep brain stimulation devices.
References
[1] Levin, M (2014). "Molecular bioelectricity: How endogenous voltage potentials control cell behavior and instruct pattern regulation in vivo". Molecular Biology of the Cell. 25 (24): 3835–50. doi:10.1091/mbc.E13-12-0708. PMC 4244194. PMID 25425556.
[2] Bates, Emily (2015). "Ion Channels in Development and Cancer". Annual Review of Cell and Developmental Biology. 31: 231–47. doi:10.1146/annurev-cellbio-100814-125338. PMID 26566112.
[3] Pool, J. L. (1954) Psychosurgery in older people. J. Am. Geriatr. Soc. 2, 456–466.
[4] Krauss J K , Lipsman N , Aziz T , et al (2020). Technology of deep brain stimulation: current status and future directions[J]. Nature Reviews Neurology.
[5] Fastest Neupsy Insight Engine (2018). Mechanisms of Action of Deep Brain Stimulation: A Review, Neupsy Key
[6] Nir Lipsman, et al (2014), Neuromodulation for treatment-refractory major depressive disorder, CMAJ January 07, 186 (1) 33-39;
[7] Pycroft, L. et al (2016).. Brainjacking: implant security issues in invasive neuromodulation. World Neurosurg. 92, 454–462