Billion-Patient Hopes Dimmed, Capital Pressure Intensifies: What Lies Ahead for the Atrial Shunt Market?
Atrial Shunt Device: An Emerging International Therapy for Heart Failure. Since Corvia Medical (acquired by Edwards Lifesciences) launched the world’s first atrial shunt device, innovative enterprises and capital investors both in China and abroad have increasingly bet on this new sector, with technological innovation and large-scale financing becoming its defining themes.
However, in February 2022, the global atrial shunt device market experienced a significant “earthquake.”
Corvia Medical’s Corvia Atrial Shunt Device Fails Phase III Clinical Trial.Data show that subjects in the atrial shunt trial who received the Corvia implant did not experience a reduced incidence of heart failure or improved health status, with results no different from those in the sham surgery group.
The Corvia device is the world’s first approved atrial shunt and currently boasts the most robust clinical evidence. Previously, the Corvia Atrial Shunt completed a series of evidence-based clinical trials, fully demonstrating its efficacy and safety in the treatment of heart failure.
The REDUCE LAP-HF II trial is the first Phase III clinical trial in the global atrial shunt device industry. Will its failure cast a shadow over this emerging sector? What lies ahead for the development pathway of these devices?
First, we need to clarify the reasons for the negative results of Corvia Medical’s current clinical trial. Heart failure, particularly HFpEF (heart failure with preserved ejection fraction), is a heterogeneous disease; as demonstrated by previous drug trials, a one-size-fits-all approach is inappropriate.
According to data published in The Lancet, Corvia Medical’s multicenter clinical trial enrolled a total of 1,072 participants, of whom 626 were randomized, including 314 assigned to the atrial shunt group and 312 to the sham procedure group.
This trial primarily enrolled patients aged ≥40 years with symptomatic heart failure, an ejection fraction ≥40%, a pulmonary capillary wedge pressure ≥25 mmHg during exercise, and a pressure gradient between the pulmonary capillary wedge pressure and the right atrium ≥5 mmHg.
Overall study results indicate that implantation of an interatrial shunt device did not reduce the overall incidence of heart failure events, nor did it improve the health status of patients with heart failure. Moreover, prespecified subgroup analyses revealed that in males, patients with a pulmonary artery systolic pressure >70 mmHg under a 20-watt exercise load (meeting the criteria for severe pulmonary hypertension), and those with a right atrial volume index >29.7 mL/m², the shunt device actually increased the incidence of adverse heart failure events.
However, according to publicly available information,In a subgroup of the REDUCE LAP-HF II trial comprising subjects with normal pulmonary vascular resistance (PVR) during exercise, no implanted pacemakers, and no pulmonary vascular disease, patients treated with an atrial shunt device experienced 0.12 heart failure events per year, compared with 0.22 events per year in the sham procedure group (a statistically significant difference). The results demonstrated that implantation of an atrial shunt device reduces the incidence of heart failure events and improves patients’ health status.
Dr. Sanjiv Shah, Co-Principal Investigator of the REDUCE LAP-HF II trial, stated, “Before this study began, we were aware that patients with severe pulmonary vascular disease were unlikely to benefit from atrial shunt procedures.”With further patient selection, atrial shunting demonstrates favorable therapeutic efficacy in patients with heart failure with preserved ejection fraction (HFpEF) without pulmonary vascular disease.”
The Chinese Expert Consensus on Interatrial Shunt Devices for the Treatment of Heart Failure with Preserved Ejection Fraction (2021) states that contraindications for interatrial shunt devices include: 1. Coexisting definitive right heart failure, such as congestive hepatopathy, recurrent lower extremity edema, or polyserositis; or imaging findings indicating a right ventricular diameter greater than the left ventricular diameter, tricuspid annular plane systolic excursion (TAPSE) < 12 mm, pulmonary valve fractional area change (PVFAC) < 25%, or resting right atrial pressure > 14 mmHg; 2. Heart failure patients with coexisting pre-capillary pulmonary hypertension.
Dr. Dai Jing, Medical Affairs Director at Deno Group’s Nuosheng Company, stated: “The negative results of Corvia Medical’s recent multicenter clinical trial were primarily related to whether appropriate patient selection was implemented. Factors such as pulmonary vascular resistance, left ventricular ejection fraction, and gender may all influence the efficacy of atrial shunt devices.”
Heart failure patients with pulmonary vascular disease may not benefit from atrial shunt procedures, whereas those with a left ventricular ejection fraction ≥50% tend to achieve better outcomes. Domestic and international companies will need to conduct clinical validation to further explore and gradually standardize patient selection criteria for atrial shunt procedures.
From the perspective of clinical demand, the market prospects for atrial shunt devices are broad, supported by over 60 million heart failure patients and more than 40 million patients with pulmonary arterial hypertension worldwide.
Heart failure has long been a challenging clinical problem. As the terminal stage of various cardiovascular diseases, it is characterized by poor prognosis, limited treatment options, and high patient mortality, earning it the reputation as the "final battlefield" of cardiovascular disease.
Approximately 2% of adults worldwide have heart failure, with prevalence increasing with age. Patients with heart failure often require hospitalization, and their quality of life is significantly reduced due to symptoms such as dyspnea, fatigue, and depression. Moreover, the prognosis is poor, with more than half of patients dying within five years.
According to a recent study published in the European Journal of Preventive Cardiology, the global number of patients with heart failure rose from 33.5 million in 1990 to 64.3 million in 2017. Among the newly diagnosed cases worldwide, 29.9% were from China.As the aging of China's population intensifies, the number of heart failure patients continues to rise, imposing a significant burden on patients' families and the national medical insurance system, thereby creating a clear demand for clinical treatment.
Based on left ventricular ejection fraction (LVEF), patients with heart failure can be classified into three subtypes: heart failure with preserved ejection fraction (HFpEF); heart failure with mildly reduced ejection fraction (HFmrEF); and heart failure with reduced ejection fraction (HFrEF). Among these, patients with HFpEF and HFmrEF account for approximately half of all heart failure cases.
Over the past decade, therapies for heart failure with reduced ejection fraction (HFrEF) have advanced rapidly. Clinical guidelines recommend pharmacological interventions, including diuretics, renin-angiotensin system inhibitors, and beta-blockers, as well as device-based therapies such as cardiac resynchronization therapy (CRT) and implantable cardioverter-defibrillators (ICDs).
However, existing treatments fail to significantly reduce mortality or morbidity in patients with HFpEF. The 2018 Chinese Guidelines for the Diagnosis and Treatment of Heart Failure state that the management of HFpEF should focus on symptom relief, underlying cardiovascular diseases and comorbidities, and cardiovascular risk factors, employing a comprehensive therapeutic approach.
HFpEF is a heterogeneous syndrome involving multiple pathophysiological mechanisms, including systemic inflammation, myocardial ischemia, tissue fibrosis, and cardiomyocyte hypertrophy. It presents significant challenges for clinical diagnosis and lacks effective pharmacological treatments.Clinical studies have failed to confirm that ACEIs/ARBs and beta-blockers improve prognosis or reduce mortality in patients with HFpEF. To date, the management of HFpEF has been largely limited to lifestyle modifications and pharmacologic therapies aimed at symptom relief.
In February 2021, the U.S. FDA approved Novartis’ Entresto as the first medication for the treatment of heart failure with preserved ejection fraction (HFpEF). This approval marked an expansion of the drug’s indications, as Entresto had previously been indicated only for patients with heart failure with reduced ejection fraction (HFrEF). With this approval, Entresto became the first and only therapy approved for the treatment of patients with guideline-defined heart failure, including both HFrEF and HFpEF.
However, in China, Entresto is currently indicated only for patients with heart failure with reduced ejection fraction (HFrEF). Patients with heart failure with preserved ejection fraction (HFpEF) primarily rely on medications such as diuretics and beta-blockers; however, these therapeutic approaches can only partially reverse ventricular hypertrophy, relax the myocardium, and improve diastolic function.
Left ventricular diastolic dysfunction, which leads to a significant and rapid increase in left atrial pressure during exercise, is considered a major contributor to heart failure symptoms and increased mortality in patients with HFpEF. A conventional surgical approach involves creating an interatrial septal shunt in HFpEF patients to allow blood flow from the left atrium to the right atrium, thereby reducing left-sided cardiac load.
Extensive prior clinical practice has demonstrated that left-to-right shunt congenital heart disease (Qp/Qs < 1.5) does not lead to right heart failure or pulmonary hypertension, and the shunt itself causes only approximately a 10% reduction in cardiac output, indicating a favorable safety profile.
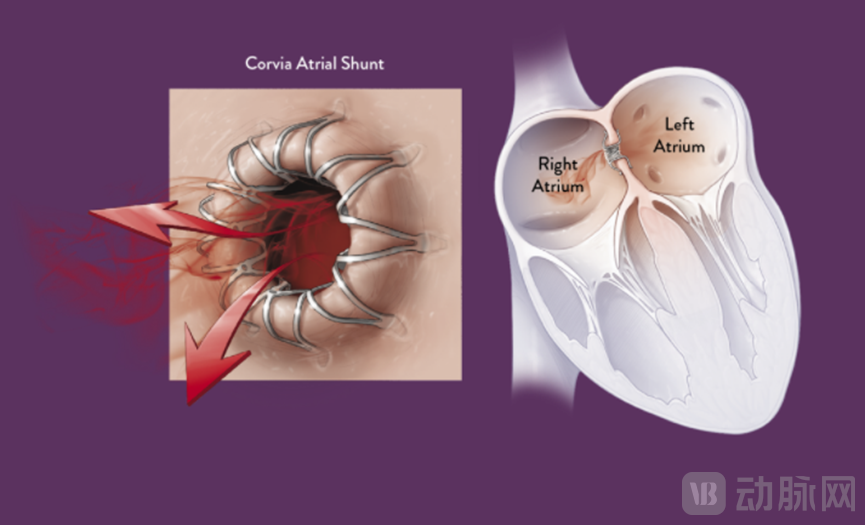
Mechanism of Action of the Atrial Shunt Device Source: Corvia Medical Official Website
Clinically,Such “south-to-north water diversion” procedures typically involve puncturing and creating an aperture in the patient’s atrial septum using a sheath, enlarging the opening with balloon dilation, and implanting an interatrial shunt device to maintain patency. This percutaneous, minimally invasive approach alleviates left atrial pressure overload without significantly reducing left ventricular output or substantially increasing right ventricular load, thereby relieving pulmonary congestion and dyspnea, and improving patients’ clinical symptoms, exercise tolerance, and prognosis.
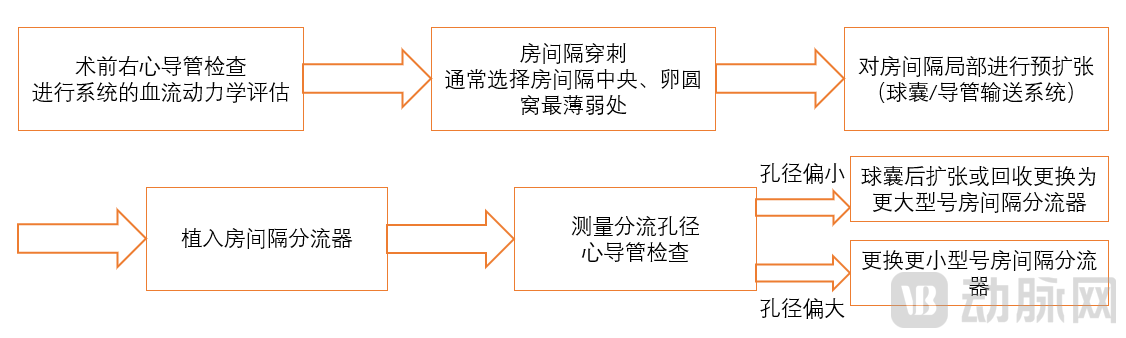
Atrial Shunt Implantation Source: "Chinese Expert Consensus on the Treatment of Heart Failure with Preserved Ejection Fraction Using Atrial Septal Shunts"
In addition to patients with HFpEF, some companies have also been expanding the indications for atrial shunt devices to include HFrEF and pulmonary hypertension in recent years.
Pulmonary hypertension is also a disease with complex etiology and lacks effective treatment options. Patients with pulmonary hypertension experience sustained right atrial hypertension, necessitating reduction of right atrial pressure to delay right ventricular enlargement and right heart failure. Additionally, patients with pulmonary hypertension can undergo atrial septostomy to establish a stable and controllable right-to-left shunt, which reduces right ventricular volume and pressure overload while increasing left ventricular preload and cardiac output.
Although right-to-left shunting appropriately reduces arterial oxygen saturation, the increased left ventricular output overall enhances myocardial and renal perfusion, thereby improving symptoms and prognosis in patients with right heart failure.
Summarize into one sentence,In patients with heart failure, left atrial pressure needs to be shunted to the right atrium; in patients with pulmonary hypertension, right atrial pressure is directed into the left atrium.However, atrial shunt devices primarily address unilateral cardiac dysfunction; therefore, they are mainly indicated for patients with heart failure with preserved ejection fraction (HFpEF) who have relatively normal right ventricular function, or for patients with pulmonary hypertension who have relatively normal left ventricular function.
According to Dr. Dai Jing of Deno Medical, “Heart failure patients with severe pulmonary vascular disease exhibit dysfunction in both the left and right atria, making them unsuitable candidates for interatrial shunt therapy. Patients with impaired left ventricular function but relatively preserved right ventricular function are more likely to benefit. By leveraging the compensatory capacity of the right heart, an effective left-to-right interatrial shunt can be established via a created septostomy, thereby reducing left atrial pressure.”
As Corvia Medical’s clinical results in the United States delivered an unexpected setback, other innovative companies worldwide continue to explore new technological directions for atrial shunt devices, with capital closely watching this emerging market.
As an implantable interventional device designed to create a shunt at the atrial septum, the atrial shunter presents certain technical challenges. First, it must provide adequate radial support to ensure stable and sustained shunting. Second, the device must exhibit excellent biocompatibility and promote endothelialization to reduce the risks of infection and thrombosis. Long-term patency is another critical consideration in product development, as changes in atrial aperture size or patient condition can alter the demand for atrial flow.
Currently,Globally, only three companies have received approval for their atrial shunt devices: Corvia Medical (United States), V-WAVE (Israel), and Occlutech (Germany).
Among them,Corvia Medical’s Corvia Atrial Shunt is the world’s first interatrial shunt device for the treatment of patients with HFpEF, and the first atrial shunt to receive CE marking.The Corvia atrial shunt consists of a nitinol shape-memory alloy laser-cut stent, with left and right atrial discs forming an interlocking structure.
In 2019, the Corvia Atrial Shunt was granted Breakthrough Device Designation by the FDA. In the same year, Corvia Medical was acquired by Edwards Lifesciences for $35 million.
To date, the Corvia Atrial Shunt has been implanted in nearly 500 patients worldwide, with the first cohort of recipients having reached seven years post-implantation. According to the official Corvia Medical website, three years after implantation, 75% of heart failure patients experienced significant improvements in quality of life, and 69% did not require hospitalization for heart failure during this period.
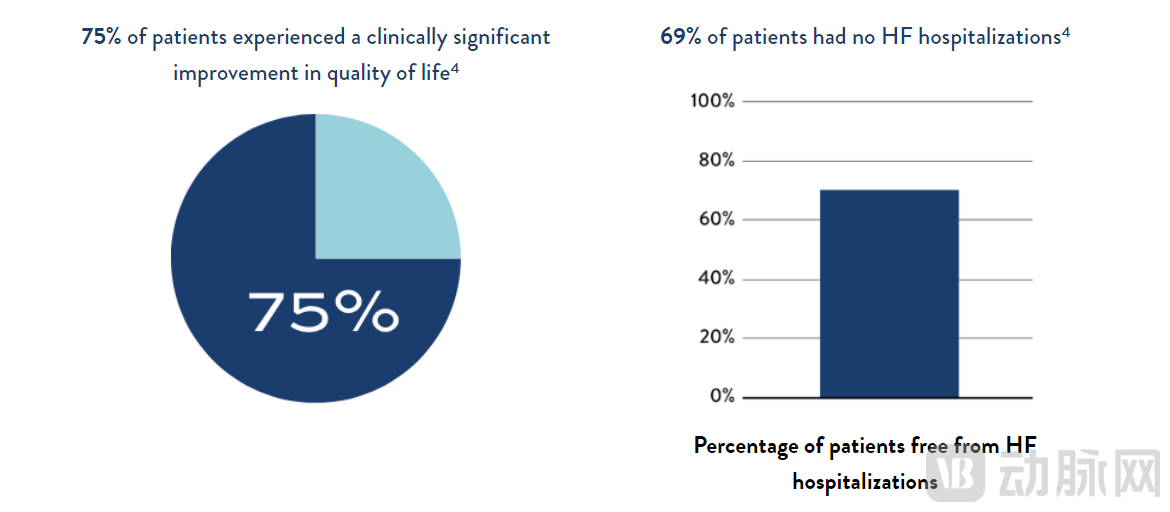
Outcomes in Heart Failure Patients Three Years After Corvia Atrial Shunt Procedure Source: Corvia Medical Official Website
V-WAVE’s atrial shunt devices comprise two generations. The first-generation V-Wave atrial shunt, limited by flaws in its unidirectional valve design, demonstrated suboptimal patency rates and has since been discontinued. The second-generation Ventura atrial shunt features an hourglass-shaped nitinol frame, with a polytetrafluoroethylene (PTFE) polymer coating on the left side and three bovine pericardial leaflets on the right side, designed to prevent embolization and early shunt occlusion.
Occlutech’s AFR Atrial Shunt is a nitinol mesh device composed of two flat discs and a connecting neck with a central fenestration. It allows blood to flow from the left atrium to the right atrium through the central shunt aperture, thereby reducing the burden on the left atrium. Once implanted, the AFR maintains an atrial shunt of fixed diameter. To meet the varying shunt requirements of different patients, the AFR is available in four different fenestration diameters.
Previously,The FDA has granted Breakthrough Device Designation to both the Ventura and AFR devices for the treatment of patients with heart failure (HFpEF or HFrEF) and pulmonary hypertension.However, to date, the FDA has not approved any atrial shunt device.
Edwards Lifesciences’ independently developed Root Device is an H-shaped stent implanted via the internal jugular vein into the central region of the left atrium–coronary sinus, creating a 7-mm-diameter shunt. Postoperatively, patients do not require immobilization. The product has currently completed a small-scale First-in-Human (FIM) study, with results yet to be disclosed.
Overall, Corvia Medical, V-WAVE, and Occlutech are leading the global market for atrial shunt devices. All three companies are conducting clinical trials to demonstrate the safety and efficacy of their existing atrial shunt devices in order to bring them to market. However, their atrial shunt systems still require further improvement in aspects such as device size, delivery sheath diameter, and retrievability.
Currently, there are no approved atrial shunt devices in China. Domestic companies are continuously breaking through with innovative product designs to bridge the time gap with superior-performing products.
First, improvements in the intrinsic performance of atrial shunt devices, such as device size, endothelialization, and radial support force. Second, heart failure patients present with varying disease severities and thus require different levels of atrial shunting. Most existing products have a fixed shunt diameter, making it difficult to meet personalized treatment needs. Furthermore, long-term implantation of atrial shunts in the human body can lead to endothelialization and a reduction in aperture size, thereby decreasing shunt volume.Adjustable Atrial Septal Shunt Diameter Emerges as a New Direction in the Development of Atrial Shunt Devices。
Furthermore, atrial shunt devices must demonstrate a favorable safety profile. Currently approved atrial shunt devices are designed for permanent implantation, which not only increases the risks of thrombosis and device migration but also makes it difficult to accommodate the need for reintervention should the patient’s condition change. Heart failure patients undergoing atrial shunt procedures are often middle-aged or elderly, and this population may have comorbidities such as atrial fibrillation and mitral stenosis that require surgical intervention. Therefore,Retrievable, biodegradable, or even non-implantable atrial shunts are also emerging as a new direction.。

Overview of Global Atrial Shunt Devices Sources: Public Information, Corporate Websites
The NoYA Atrial Shunt System, developed by Nuosheng Medical under Deno Medical, is the world’s first independently developed, implant-free, adjustable atrial shunt device. During the procedure, the operator anchors a diameter-adjustable stent to the interatrial septum and uses radiofrequency energy to heat, coagulate, and contract the septal tissue surrounding the stent, thereby creating a permanent interatrial communication.
Post-procedure, the system is completely withdrawn from the body, leaving no implants behind. This fundamentally avoids complications such as device migration and thrombosis, while preserving the option for future transseptal procedures.Moreover, the NoYA atrial shunt system features an adjustable shunt orifice design, with a stent diameter adjustable from 4 to 10 mm, to meet diverse shunting requirements.
The NoYA Atrial Shunt completed its first-in-human (FIM) study with 10 cases in Q2 2019. Clinical studies showed no device-related adverse events during the 6-month follow-up period, a decrease in NT-proBNP levels from baseline, and significant improvement in NYHA functional class, demonstrating the favorable efficacy and safety profile of the atrial shunt device. Currently, the NoYA Atrial Shunt System is undergoing large-scale, multicenter clinical trials across China.
Weike Medical’s D-Shant Atrial Shunt is China’s first independently developed implantable atrial shunt device.This product features an inward-locking metal stent design, is only the size of a coin, and provides excellent radial support. Additionally, D-Shant allows for secondary intervention, ensuring surgical safety.
As of December 2020, Wuhan Union Hospital and Beijing Fuwai Hospital had jointly completed a first-in-man (FIM) clinical study involving 20 cases. Patients demonstrated significant postoperative hemodynamic improvement, and no aperture stenosis or occlusion, embolic events, or other serious adverse events were observed during the 6-month follow-up.
Furthermore, atrial shunts developed by Lepu Heartcare, Qichen Medical Group, and Aoliu Medical have also entered the First-in-Human (FIM) study phase; all are implantable stents. In addition to innovations in adjustable diameter and retrievability, domestic companies have made improvements in terms of device size, endothelialization, and morphology. Chinese enterprises are narrowing the time gap through technological advancements.

Incomplete Statistics on Chinese Atrial Septal Defect Device Manufacturers Source: Public Information
Capital has responded with equal enthusiasm.In November 2021, Weike Medical completed a Series B financing round amounting to hundreds of millions of yuan, led by Sequoia China; in January 2022, Aoliu Medical closed its Series A financing round of nearly RMB 60 million. In February 2022, Lepu Xintai announced that it had passed the listing hearing.
It is evident that, at a time when there are still no effective treatments for heart failure globally, the atrial shunt market has become highly coveted, driven by both early-stage technological and product accumulation as well as capital infusion during its development.
Although the recent clinical trial of the Corvia atrial shunt device yielded negative results, it has brought to light underlying issues within the industry. This will drive enterprises and clinical researchers to explore and clarify the impact of factors such as ejection fraction, pulmonary artery pressure, and hemodynamics on the efficacy of atrial shunt therapy, further standardize the indications and treatment protocols for atrial shunt procedures, and improve both the product technology of atrial shunt devices and clinical trial design.
References:
“A Brief Discussion on the Essence of Heart Failure Treatment: Starting from the REDUCE LAP-HF II Study” — “CCI Cardiovascular Physician Innovation Club”
"Is HFpEF Diagnosis and Treatment Challenging? A Comprehensive Review of New Advances in Heart Failure Therapy Research! | 2021 Great Wall Conference" — Medical World Cardiovascular Channel
“Landmark REDUCE LAP-HF II Trial Demonstrates Clinical Benefit of Corvia® Atrial Shunt in Large Segment of Heart Failure Patients” — Corvia Medical Official Website
"Lepu HeartTech Prospectus"
“Chinese Expert Consensus on Atrial Septal Shunt Devices for the Treatment of Heart Failure with Preserved Ejection Fraction (2021)”