Investment Value and Development Trends of Assisted Reproductive Technology (ART) Pharmaceuticals: Market Potential, Policy Support, and Innovation Outlook
In recent years, China’s birth rate has continued to decline. Whether this downward trend in the number of births can be reversed in the future hinges on whether fertility rates can be increased. There is substantial room for improvement in both the penetration rate and success rate of assisted reproductive technology (ART) in China, creating a vast ART market. Driven by multiple factors, including clinical demand, policy support, and capital investment, the ART sector demonstrates significant investment value. The entire ART process requires effective pharmacological support; therefore, related drugs occupy an important position in the industry chain. Currently, ART-related pharmaceuticals are predominantly imported, leaving considerable potential for domestic substitution. Furthermore, innovative drugs in the field of assisted reproduction represent a key area worthy of focused investment attention. For instance, premature ovarian insufficiency (POI) is a major cause of infertility, characterized by a high incidence rate and a current lack of preventive or therapeutic measures. An increasing number of universities and enterprises, both domestically and internationally, are developing innovative therapies to preserve or extend ovarian function, which will have a profound impact on reproductive medicine.

▲Source: Postdoctoral Innovation Practice Base of Oriental Fortune Capital Investment Management Co., Ltd.
Data released by the National Bureau of Statistics in January 2022 showed that China’s birth rate in 2021 hit its lowest level since 1952. If this declining trend continues, new population growth may turn negative in 2022, and China will soon enter an aging society. Whether the downward trend in births can be moderated in the future hinges on whether fertility rates can be raised. In China, the age range for first-time mothers is primarily concentrated between 20 and 29 years, while for second-time mothers it is mainly between 25 and 34 years. With the implementation of the three-child policy, fertility demand among older women will increase, generating substantial demand for assisted reproductive technologies (ART). Chinese data indicate that, due to factors such as delayed marriage and childbearing and the two-child policy, the number of newborns contributed by women aged 35–45 has been rising steadily. Based on statistics on female childbearing age and infertility rates in China, more than 50 million women face infertility issues. According to Frost & Sullivan, the prevalence of infertility in China has been increasing year by year, and by 2023 the proportion of the population affected by infertility is projected to reach 18.2%. The main reasons for the rising prevalence of infertility include:
1) Delayed marriage and childbearing: Infertility rates are positively correlated with age; as the number of individuals delaying marriage and childbearing increases, infertility rates rise;
2) Suboptimal lifestyle habits: Staying up late, reduced physical activity, and unhealthy diets contribute to a state of suboptimal health, thereby increasing the risk of infertility;
3) Increased life stress is also a significant factor contributing to the rising infertility rate.
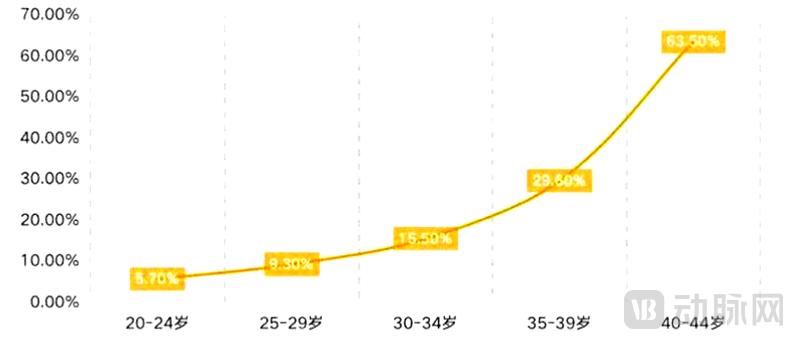
Fertility Age and Infertility Rates Among Chinese Women
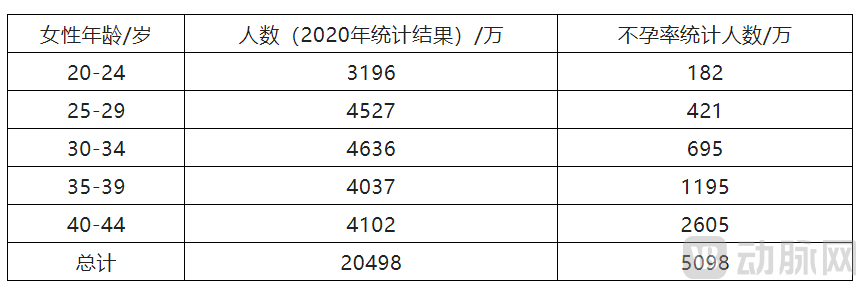
Number of Chinese Women by Childbearing Age
▲ Source: Data released by the National Bureau of Statistics in 2020
Currently, the penetration rate of assisted reproductive technology (ART) in China is only 7%, representing a significant gap compared to the nearly 30% penetration rate in the United States. According to a report by Qianzhan Industry Research Institute, the average success rate of in vitro fertilization (IVF) at domestically approved reproductive centers and infertility hospitals stands at approximately 50%, which is lower than that of the United States, Thailand, Germany, and Malaysia. Therefore, there is substantial room for improvement in both the penetration rate and success rate of ART in China. Assisted reproductive drugs account for approximately 34% of the market share in terms of treatment costs. Based on projections by Ping An Securities Research Institute, China’s assisted reproductive drug market is expected to reach RMB 23.4 billion by 2025, indicating broad market prospects.
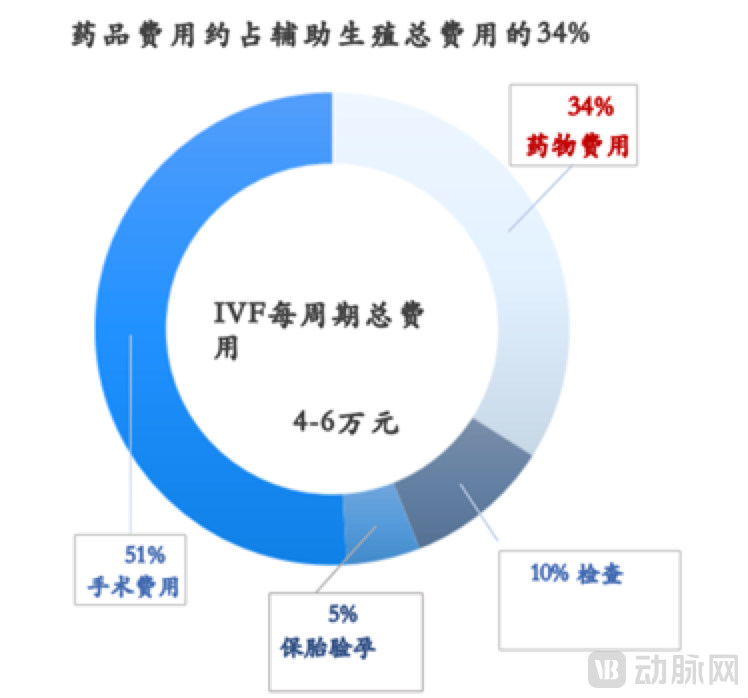
▲Source: PDB, Ping An Securities Research Institute
China’s fertility policies have undergone five major phases: from encouraging childbirth, to birth control, to family planning, to the one-child policy, and finally to the two-child policy and the recent relaxation to allow three children in the new era. With the implementation of the three-child policy, fertility demand among older-age populations will increase, thereby driving greater demand for assisted reproductive technologies (ART). Public hospitals are currently unable to meet this surging demand; consequently, the industry is expected to see a rise in chain-based institutions that extend their services downstream, forming integrated specialty care centered on pregnancy, childbirth, and maternal-infant health. In addition, the state has refined and tightened relevant regulations, and more policies are anticipated to be introduced in the future to standardize market practices while supporting industry development.
The inclusion of assisted reproductive technology (ART) medications in the medical insurance reimbursement scope also reflects a positive policy signal. On August 23, 2021, the National Healthcare Security Administration issued the “Reply of the National Healthcare Security Administration to Suggestion No. 5581 at the Fourth Session of the 13th National People’s Congress,” explicitly stating that eligible fertility-supporting medications, including bromocriptine, triptorelin, and clomiphene citrate for ovulation induction, would be included in the reimbursement list. Consequently, medical insurance now covers all categories of medications throughout the entire ART cycle, including down-regulation agents, ovulation-inducing drugs, ovulation-triggering agents, and luteal phase support medications.
In February 2022, the Beijing Municipal Healthcare Security Administration, in conjunction with the Municipal Health Commission and other departments, issued the "Notice on Standardizing and Adjusting Prices for Certain Medical Services," which standardized and adjusted the prices of 63 medical service items. Concurrently, the Municipal Healthcare Security Administration and the Municipal Human Resources and Social Security Bureau introduced supporting policies for medical insurance and work-related injury reimbursement. As part of proactive measures to support fertility, and based on the principles of cost controllability and ensuring the sustainability of the medical insurance fund, 16 assisted reproductive technology (ART) procedures—such as intrauterine insemination, embryo transfer, and sperm optimization processing, which are widely applicable, clinically necessary, technically mature, safe, and reliable—were included in the Category A reimbursement scope of basic medical insurance for outpatient treatment. Currently, there are 15 designated basic medical insurance institutions in Beijing qualified to provide assisted reproductive services. In addition to national medical insurance, commercial insurance is also providing support for assisted reproduction, with some insurers launching specific IVF insurance products.
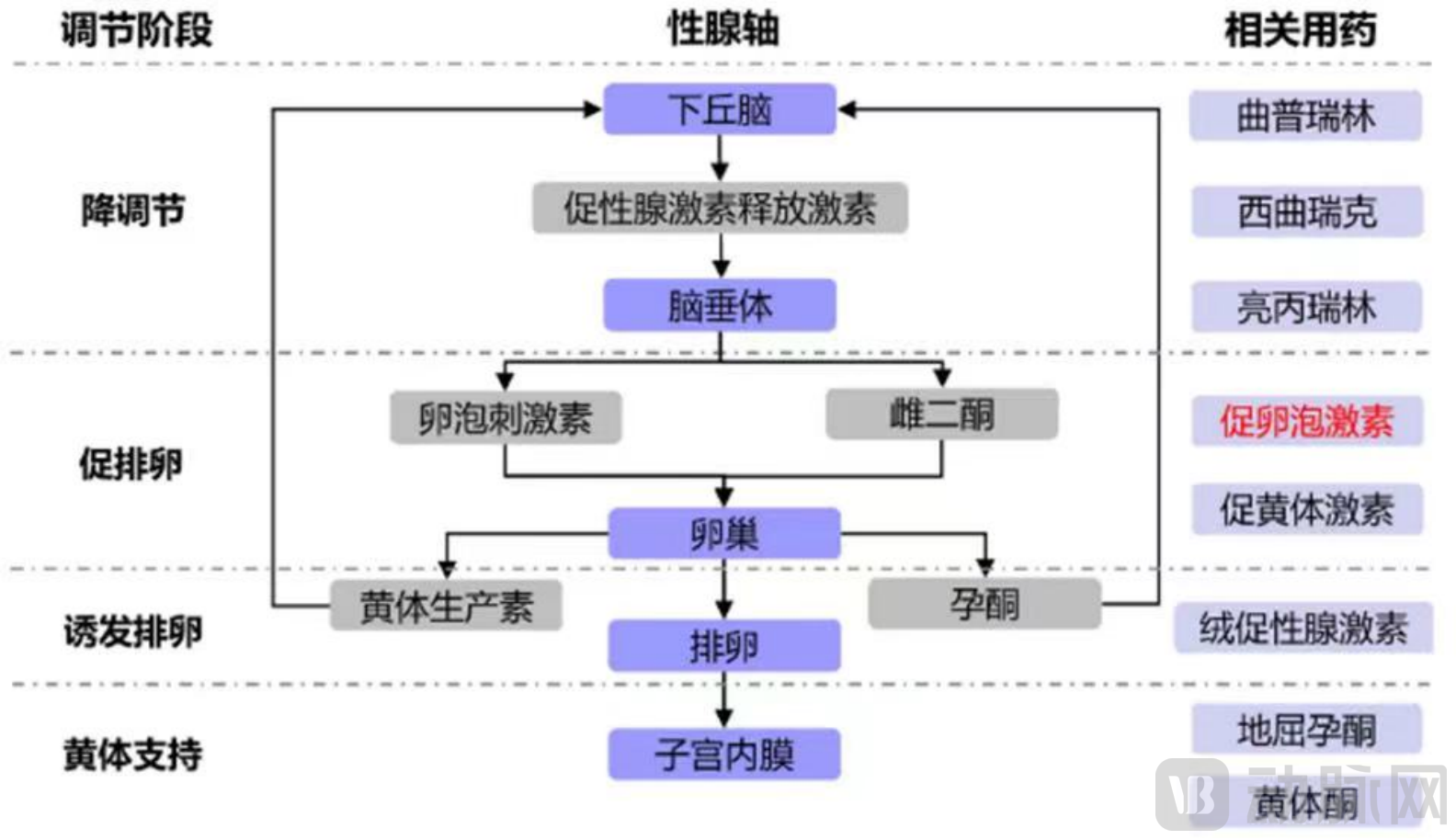
The human reproductive cycle is characterized by monofollicular development and ovulation. The majority of follicles undergo three stages—recruitment, selection, and dominance—to reach maturity. In a normal menstrual cycle, follicle-stimulating hormone (FSH) serves as a key regulator in follicular development, playing a crucial role in balancing follicular recruitment and atresia. Luteinizing hormone (LH) governs the development, selection, and ovulation of the dominant follicle. GnRH agonists bind to GnRH receptors in the pituitary gland, initially promoting the release of FSH and LH; however, with continuous administration, they suppress the synthesis and release of pituitary gonadotropins (Gn) and ovarian sex hormones. GnRH antagonists bind to pituitary GnRH receptors without exerting biological activity, thereby completely blocking the effects of endogenous GnRH and causing a rapid decline in serum FSH and LH levels.
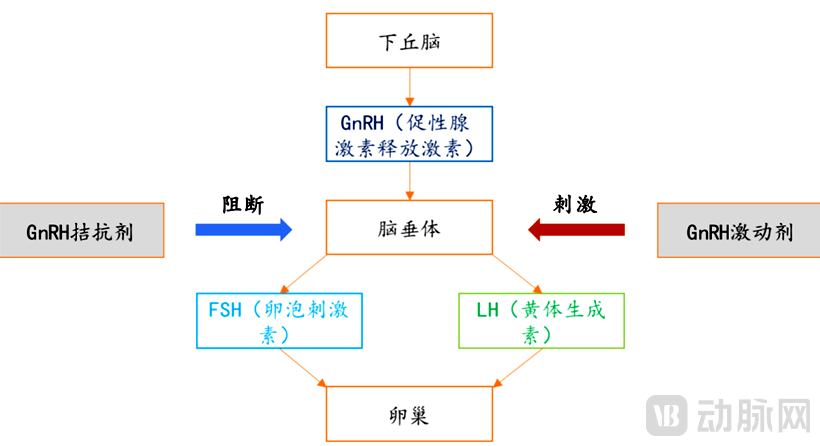
▲Source: Ping An Securities Research Institute
Premature Ovarian Insufficiency (POI) is a condition characterized by diminished ovarian function in women under the age of 40. It is defined by amenorrhea lasting at least four months, intermittently elevated follicle-stimulating hormone (FSH) levels exceeding 25 IU/L (with intervals of at least four weeks between measurements), and low estrogen levels, leading to infertility. Currently, there are no effective pharmacological treatments specifically approved for POI. In the context of assisted reproductive technology (ART), growth hormone (GH) can be administered to poor responders with compromised ovarian function to improve clinical pregnancy rates. GH enhances oocyte quality by regulating its own receptors and boosting mitochondrial activity. It also indirectly stimulates the ovaries via the insulin-like growth factor (IGF) axis, thereby increasing ovarian responsiveness to ovulation induction agents. Furthermore, GH promotes follicular development and oocyte maturation by modulating hormone production.
Pharmacological treatment for assisted reproduction aligns with hormonal regulation during the reproductive cycle and is primarily divided into four stages: down-regulation, ovarian stimulation, ovulation induction, and luteal phase support. Different types of medications are used in each stage. Ovarian stimulation drugs are the most extensively used, typically requiring 20–40 injections per treatment cycle. They account for the highest proportion of costs, exceeding 60%, followed by luteal phase support drugs at approximately 20%, down-regulation drugs at around 15%, and ovulation induction drugs at about 5%. Currently, this market is characterized by an oligopolistic structure. Merck is the leader in assisted reproductive drugs and has launched multiple products in China, including cetrorelix, recombinant follicle-stimulating hormone (rFSH), recombinant human chorionic gonadotropin (r-hCG), and progesterone gel. Foreign companies such as Merck and MSD hold significant advantages. However, with the trend toward domestic substitution, competition among Chinese-made assisted reproductive drugs is becoming increasingly intense. Commonly used assisted reproductive medications fall into the following four categories:
1) Down-regulation medications: including GnRH agonists and GnRH antagonists, which temporarily suppress the natural production of reproductive hormones;
2) Ovulation induction drugs: including follicle-stimulating hormone, human menopausal gonadotropin, luteinizing hormone, clomiphene, and letrozole, which promote follicular growth and development;
3) Induction of ovulation: Human chorionic gonadotropin (hCG) is used to induce final oocyte maturation, rendering the egg fertilizable;
4) Luteal phase support: including dydrogesterone and progesterone, to prepare the endometrium for embryo implantation.
▲Source: Compiled by Zhiyin Pharma
Down-regulation drugs
I. GnRH Agonists (GnRH-a)
Since 1984, gonadotropin-releasing hormone (GnRH) analogs have been used in controlled ovarian stimulation cycles for in vitro fertilization. Synthetic decapeptide analogs of GnRH exhibit greater potency than native GnRH and can regulate the levels of luteinizing hormone (LH), follicle-stimulating hormone (FSH), testosterone (T), and estradiol (E2) in human blood.
GnRH agonists (GnRH-a) are available in short-acting and long-acting formulations. Short-acting formulations are administered daily, whereas long-acting formulations are administered at intervals of 1, 3, 4, 6, or 12 months. Commonly used GnRH-a in China include leuprorelin and triptorelin, both of which command substantial market shares, with leuprorelin being the leading product. Imported leuprorelin is priced at approximately RMB 1,750 per box, while domestically produced leuprorelin is priced at no less than RMB 1,500 per box. Triptorelin is currently marketed primarily by three companies: Ipsen, Ferring, and GenSci Pharmaceutical. From January to September 2021, sales of triptorelin acetate in public hospitals across key provinces and municipalities in China exceeded RMB 400 million, representing a year-on-year increase of 36.25%. Among these sales, Ipsen (France) accounted for 67.13%, Ferring Pharmaceuticals for 32.21%, and Changchun GenSci Pharmaceutical for 0.66%.
Compared with GnRH antagonists, a disadvantage of GnRH agonists is their inability to promptly suppress the release of endogenous gonadotropins; therefore, pretreatment suppression is required for a period prior to the initiation of gonadotropin therapy.
II. GnRH Antagonists (GnRH-A)
The invention of GnRH antagonists has not only provided clinicians with an alternative to GnRH agonists but also spurred innovations aimed at enhancing the safety and simplicity of ovarian stimulation. These advancements include refined natural cycle protocols, the development of minimal stimulation protocols, the use of agonists to trigger final oocyte maturation, the administration of antagonists during the luteal phase to prevent ovarian hyperstimulation syndrome (OHSS), and the application of antagonist protocols in intrauterine insemination (IUI) cycles to control endogenous LH surges.
GnRH antagonists (GnRH-A) competitively bind to pituitary GnRH receptors, inhibiting the release of gonadotropins (Gn). They are characterized by rapid onset and short duration of action, with pituitary function recovering rapidly after discontinuation. The inhibitory effect is dose-dependent, exhibiting linear pharmacokinetics. Studies have shown that there is no statistically significant difference in pregnancy rates or live birth rates between the GnRH-A protocol and the GnRH agonist (GnRH-a) long protocol. However, the incidence of ovarian hyperstimulation syndrome (OHSS) is significantly lower in patients using GnRH-A compared to those using GnRH-a, with the difference being statistically significant.
Cetrorelix is a key GnRH antagonist in China, with the market currently dominated by imported products. The originator of cetrorelix is Baxter, and it is primarily marketed by Merck and Hybio Pharmaceutical. Merck holds a market share of over 90%, indicating substantial potential for domestic substitution.
Ovulation Induction and Superovulation Drugs
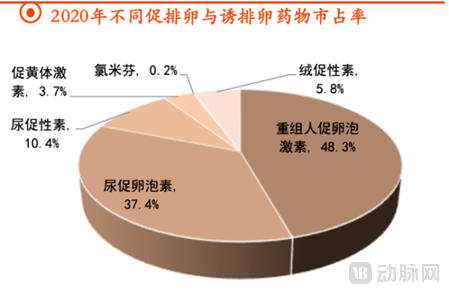
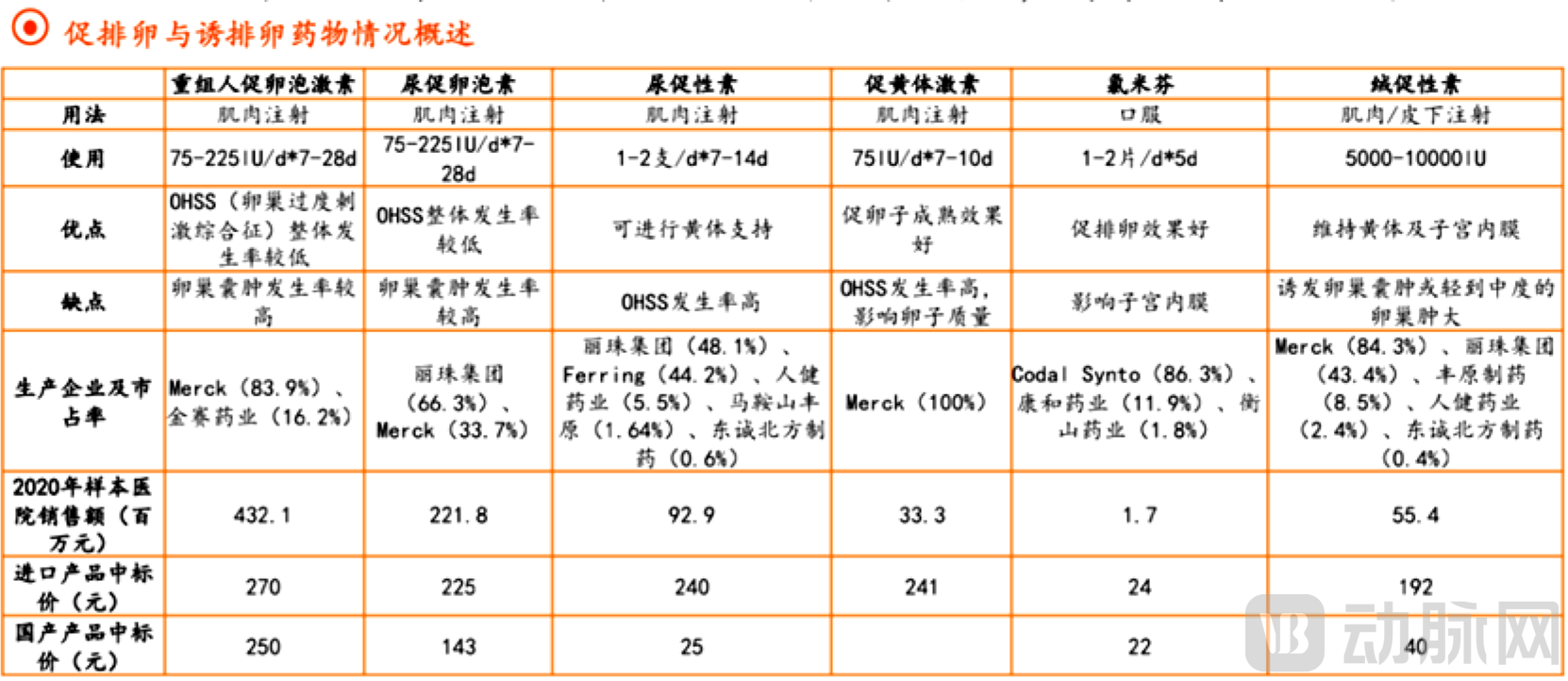
There are various ovulation-inducing drugs that act at different levels of the hypothalamic-pituitary-ovarian axis and exert effects through diverse mechanisms. Among them, recombinant follicle-stimulating hormone (rFSH) holds the largest market share, followed by urinary follicle-stimulating hormone (uFSH). Human menopausal gonadotropin (hMG) and human chorionic gonadotropin (hCG) rank third and fourth, respectively. Sales in sample hospitals in key cities remain dominated by imported products, with domestically produced products accounting for a relatively low proportion. The overall prices of domestically produced drugs are significantly lower than those of imported products, allowing domestic manufacturers to leverage their price advantage to prioritize capturing the primary healthcare market. With the rapid development of the assisted reproductive technology industry and market penetration into lower-tier regions, domestically produced products have substantial room for growth.
▲Source: YAOZHI, PDB, Ping An Securities Research Institute
I. Follicle-Stimulating Hormone
Follicle-stimulating hormone (FSH) is a highly glycosylated protein synthesized and secreted by the gonadotropic cells of the anterior pituitary gland. By binding to its receptors, FSH promotes follicular growth and development, stimulates the synthesis and secretion of estrogen by the ovaries, and thereby facilitates the formation of mature follicles. The market size for FSH in China is substantial. From 2012 to 2019, sales of FSH in sample hospitals grew annually from RMB 550 million to RMB 1.05 billion, representing a compound annual growth rate (CAGR) of approximately 9.8%. The terminal sales of FSH are estimated to exceed RMB 3 billion. Currently, growth in European and American markets has stagnated, whereas China has emerged as a sunrise market. All FSH products currently marketed in China are short-acting formulations, which can be categorized into urinary-derived FSH and recombinant FSH. Urinary-derived FSH continues to hold a certain market share due to its price advantage. However, as the production costs of recombinant FSH in China further decrease, the exit of urinary-derived products from the market has become an inevitable trend, and domestically produced products will gradually replace imported ones.
▲Source: Ping An Securities Research Institute
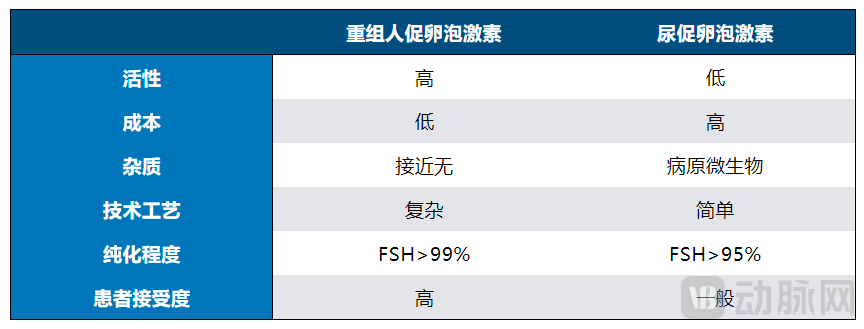
Recombinant human follicle-stimulating hormone (rhFSH) surpasses urinary follicle-stimulating hormone (uFSH) in terms of biological activity, purity, and safety, thereby commanding the majority of the market share. Currently, the primary manufacturers of FSH in China include Merck, Organon, Livzon Pharmaceutical Group, and GeneScience Pharmaceuticals. The products offered by Organon and Merck are recombinant FSH, Livzon’s product is urinary FSH, and GeneScience Pharmaceuticals’ recombinant human FSH (Jinsaiheng) is a domestically produced rhFSH. Due to stricter quality control during the manufacturing process, rhFSH is preferred by large hospitals. While Merck dominates the sales of rhFSH, the market share of domestic products is gradually increasing. Data on rhFSH usage in public hospitals indicates that the growth rate of domestic drugs is more than double that of imported drugs. At present, four brands—Gonal-f, Jinsaiheng, Anxinbao, and Fangleshu—are engaged in intense competition. Clinical results from Guizhou Medical University in 2021 demonstrated that among non-low responders, the use of either domestically produced or imported rhFSH in long-acting ovulation induction protocols during the follicular phase yielded equally safe ovulation induction efficacy and pregnancy outcomes. This indicates that, with equivalent efficacy, domestically produced rhFSH offers a price advantage. In the future, domestic recombinant FSH is expected to gradually replace urinary FSH, and domestic products will also capture market share from imported alternatives.
Short-acting follicle-stimulating hormone (FSH) still has certain limitations, including a short half-life of clinical products, frequent injections, and poor patient compliance. The development of long-acting FSH can address the drawback of the short half-life associated with existing drugs. Therefore, convenient-to-use long-acting recombinant FSH for clinical application represents the future direction of research and development. Elonva, launched by Organon in 2010, was the first long-acting FSH to enter the market. By employing site-directed mutagenesis and gene recombination technologies, Organon extended the in vivo activity duration of Elonva by approximately tenfold compared to traditional FSH. A single injection of Elonva showed no significant differences in fertilization rate, number of embryos, pregnancy rate, or hormone levels when compared with daily injections of traditional FSH over seven days. However, according to industry experts, the half-life of Elonva is actually only twice that of short-acting FSH, necessitating high-dose administration to maintain blood drug concentrations over seven days, which can cause strong ovarian stimulation. Currently, this drug is approved only in the European Union; it has not been approved by the U.S. Food and Drug Administration (FDA) or the Center for Drug Evaluation (CDE) in China. Regarding long-acting recombinant human FSH, domestic companies such as Baoji Pharmaceutical, GeneScience Pharmaceuticals, Shuanglu Pharmaceutical, and GenCare Biopharma have also made strategic layouts, with their products currently in clinical stages.
II. Human Menopausal Gonadotropin
Human Menopausal Gonadotropin (hMG) primarily exerts the effects of Follicle-Stimulating Hormone (FSH) while also containing Luteinizing Hormone (LH). In women, hMG promotes follicular development and maturation, stimulates estrogen secretion by the follicles, and induces endometrial proliferation. The subsequent administration of Human Chorionic Gonadotropin (hCG) can enhance ovulation induction. Livzon Group holds a dominant market position for this product, with a market share of 48% in 2020. However, the sales proportion of Livzon Group’s product in sample hospitals across key cities has shown a declining trend in recent years, while the market share of the imported brand from Ferring has gradually increased. This shift is mainly attributed to the fact that the imported product is high-purity hMG, which contains fewer protein impurities and causes fewer allergic reactions. Currently, Livzon Group’s high-purity hMG has entered clinical trials. The launch of this product is expected to further expand the market share of domestically produced alternatives and capture greater market presence.
III. Luteinizing Hormone
Luteinizing hormone (LH), secreted by the basophilic cells of the anterior pituitary gland, acts on mature ovarian follicles to induce ovulation and corpus luteum formation. It also promotes estrogen secretion by the corpus luteum, theca interna, and interstitial cells. Lutropin alfa, currently used in assisted reproductive technology, shares the same structure and physiological responses as endogenous LH. Sales of lutropin alfa in sample hospitals across key cities had been steadily increasing but began to decline in 2019. Merck currently holds the entire domestic market for lutropin alfa.
IV. Clomiphene
Clomiphene (clomiphene citrate) is a non-steroidal estrogen antagonist that exhibits strong anti-estrogenic effects and weak estrogenic activity. It competitively binds to estrogen receptors in hypothalamic cells, thereby relieving the negative feedback inhibition of estrogen on the hypothalamus. This stimulates the release of gonadotropin-releasing hormone (GnRH) from the hypothalamus, promoting the secretion of follicle-stimulating hormone (FSH) and luteinizing hormone (LH), which in turn facilitates follicular growth and development. The efficacy of clomiphene for ovulation induction is approximately 80%, but the pregnancy rate is only 35%–40%. The primary reason for this discrepancy is that the local anti-estrogenic effect of clomiphene causes cervical mucus to become thickened, hindering sperm penetration, and impairs endometrial development. Although dominant follicles develop, the endometrium becomes excessively thin, adversely affecting implantation of the fertilized egg. Concurrent administration of clomiphene with estrogen (initiated simultaneously with clomiphene at an oral dose of 1 mg/day until follicular maturation and ovulation) can mitigate its adverse effects on the endometrium.
V. Letrozole
Third-generation aromatase inhibitors are synthetic benzotriazole derivatives. Letrozole reduces estrogen levels by inhibiting aromatase, which increases pituitary follicle-stimulating hormone (FSH) secretion via negative feedback, thereby inducing follicular growth and development. Meanwhile, it inhibits the conversion of androgens to estrogens, leading to increased local androgen concentrations in the ovaries. Elevated androgen levels enhance follicular sensitivity to FSH, improving the responsiveness of patients with polycystic ovary syndrome (PCOS) to ovulation-inducing agents. Side effects include hot flashes, nausea, and fatigue, most of which are caused by estrogen deficiency. In terms of efficacy, letrozole is less effective than clomiphene for ovulation induction; however, it offers a higher overall success rate for subsequent blastocyst implantation and causes less physical harm to women. Clinical studies on monotherapy ovulation induction in patients with infertility due to ovulatory dysfunction have shown that letrozole can improve endometrial receptivity indices, result in smaller fluctuations in serum sex hormone levels, and significantly increase clinical pregnancy rates.
VI. Human Chorionic Gonadotropin
Human chorionic gonadotropin (hCG) shares the same alpha subunit structure as luteinizing hormone (LH). It exhibits biological and immunological activities similar to those of LH. When used to promote follicular maturation, high-dose injections are required to mimic the preovulatory LH surge. A single high dose can induce follicular maturation and ovulation, while also supporting luteal function. It is administered when the dominant follicle reaches maturity criteria, typically at a dosage of 5,000–15,000 IU, given as a single intramuscular injection or divided into two injections. Human menopausal gonadotropin primarily promotes the development and maturation of multiple follicles, which may result in multiple pregnancies. Currently, Merck holds the largest market share for hCG in China, at 45.44%. Merck’s product is recombinant human chorionic gonadotropin, which offers superior product stability. Livzon Pharmaceutical Group follows closely with a market share of 43.36% for its hCG product.
Luteal Phase Support Medications
Luteal phase support medications can thicken the endometrium, facilitating embryo implantation, and constitute an indispensable component of assisted reproductive technology (ART). These medications include dydrogesterone and progesterone. In China, dydrogesterone is exclusively distributed by Solvay, while progesterone is primarily marketed by Merck and Besins Healthcare. Both products achieved steady growth from 2019 to 2021, with a decline observed in 2020 due to the impact of the pandemic. Progesterone ranks second among sex hormones and genital tract regulators. From January to September 2021, the progesterone market in key provincial and municipal public hospitals in China reached RMB 320 million, representing a year-on-year increase of 29.03%. The top three manufacturers in this segment during the same period were Merck Serono, Zhejiang Xianju Pharmaceutical, and Laboratoires Besins. Foreign brands dominate the public hospital market, while domestic brands have emerged as a rapidly growing force. With the development of the ART industry, demand for luteal phase support medications is expected to continue rising.
Physicians typically formulate individualized controlled ovarian stimulation protocols for assisted reproductive technology (ART) by comprehensively considering the patient’s baseline characteristics (age and ovarian reserve), serum anti-Müllerian hormone (AMH) levels, basal follicle-stimulating hormone (FSH) levels, antral follicle count (AFC), body mass index (BMI), and prior ART treatment history. Commonly used ovarian stimulation protocols include the following categories, which differ based on the type of down-regulation agents employed and the duration of their administration:
1. Long Protocol
The long protocol is primarily suitable for patients with normal ovarian reserve and regular menstruation, and is also applicable to those with uterine fibroids, adenomyosis, or endometriosis. It can effectively suppress premature LH surges, reduce the number of cycle cancellations, ensure good follicular synchronization, yield a higher number of oocytes, maintain stable clinical pregnancy rates, and allow for fresh embryo transfer. It is divided into the follicular-phase long protocol and the luteal-phase long protocol:
1) Long Protocol for the Follicular Phase: On days 2–3 of the menstrual cycle, administer a long-acting gonadotropin-releasing hormone agonist (GnRH-a) at a dose of 3.75 mg. Assess hormone levels and follicle size after 30 to 45 days. Once down-regulation criteria are met, initiate ovulation induction with gonadotropins (Gn). Monitor serum hormone levels and follicle size; when follicular development is appropriate, perform triggering and oocyte retrieval.
2) Long luteal phase protocol: Starting 5–6 days after ovulation, administer gonadotropins (Gn) at a dose of 1.5–1.875 mg. After 16 days, measure hormone levels and follicle size. Once down-regulation criteria are met, use Gn for ovarian stimulation, monitor serum hormone levels and follicle size, and perform oocyte retrieval when follicular development is appropriate.
2. Antagonist Protocol
The antagonist protocol is convenient to use, features a shorter duration of ovarian stimulation, requires less medication, and reduces the risk of ovarian hyperstimulation syndrome (OHSS). Gonadotropins (Gn) are administered for ovarian stimulation starting on day 2 or 3 of the menstrual cycle. An antagonist is added after 5–7 days of Gn administration, or when the leading follicle reaches a diameter of ≥14 mm or luteinizing hormone (LH) levels reach ≥10 IU/L. This protocol is widely used in patients with high ovarian response and can significantly reduce the risk of OHSS compared to the long protocol. Fresh embryo transfer can be performed in patients without significant symptoms of OHSS.
3. Clomiphene Protocol
On days 2–3 of the menstrual cycle, clomiphene citrate (CC) at 5 mg/day and letrozole (LE) at 2.5 mg/day are initiated, concurrently with gonadotropins (Gn) for ovarian stimulation. Serum hormone levels and follicular development are monitored to adjust the Gn dosage. Upon maturation of the follicles, ovulation triggering, oocyte retrieval, embryo culture, and freeze-all strategy are performed. In subsequent cycles, endometrial preparation is carried out followed by embryo transfer. This protocol is widely used in patients with poor ovarian response; it requires fewer days of Gn administration and a lower total Gn dose. However, due to its adverse effects on endometrial receptivity, fresh embryo transfer is contraindicated, and frozen-thawed embryo transfer must be performed in a subsequent cycle.
4. Ovulation Induction Protocols Under High Progestin Conditions
On days 2–3 of the menstrual cycle, medroxyprogesterone acetate (MPA) at a dose of 4–10 mg is initiated concurrently with gonadotropins (Gn) for ovarian stimulation. Serum hormone levels and follicular development are monitored to adjust the Gn dosage. Upon maturation of the follicles, trigger administration, oocyte retrieval, embryo culture, and freeze-all strategy are performed. Endometrial preparation and embryo transfer are carried out in subsequent cycles. This protocol is widely used in patients with poor ovarian response due to its convenience and lower medical costs; however, fresh embryo transfer is contraindicated because of its adverse effects on endometrial receptivity, necessitating frozen-thawed embryo transfer in later cycles. Its application is also increasingly common in patients with polycystic ovary syndrome (PCOS), associated with a lower incidence of ovarian hyperstimulation syndrome (OHSS).
With demographic shifts and the evolution of the social environment, the prevalence of infertility has increased. Despite the advancements in assisted reproductive technology (ART), several issues remain worthy of attention, such as ovarian hyperstimulation syndrome (OHSS) resulting from controlled ovulation induction and the rise in multiple pregnancies due to the implantation of multiple embryos; these challenges urgently require solutions. Future ART medications will be capable of retrieving morphologically superior and consistent oocytes through mild ovarian stimulation. By replacing urinary-derived gonadotropins with bioengineered synthetic gonadotropins (FSH, LH, and hCG), it is possible to fully mimic the normal physiological reproductive environment in vivo. This approach not only shortens the duration of ovarian stimulation for patients but also yields oocytes of better quality. In the future, the market share of drugs such as recombinant human follicle-stimulating hormone (rhFSH), recombinant follitropin beta, and recombinant human chorionic gonadotropin (rhCG) is expected to expand further. Additionally, the development of convenient long-acting products for clinical use represents a key direction for future R&D. Currently, the ART medication market is dominated by imported products. However, as domestic enterprises strengthen their R&D and commercial expansion capabilities, they are poised to capture market share and achieve import substitution with Chinese-made alternatives. In terms of innovation and optimization of administration routes, the development of oral or transdermal medications that can effectively induce ovulation will constitute another significant direction for future development.
The ovaries in women age on average five times faster than other organs. The development of drugs that preserve or extend ovarian function will have a profound impact on women’s reproductive health. Recently, an increasing number of innovative R&D achievements in this field have emerged both in China and abroad. In February this year, a study published by Professor Lu Bai’s team from the School of Pharmaceutical Sciences at Tsinghua University in Nature Communications demonstrated that TrkB-activating antibody drugs can promote follicular development, representing a potential innovative therapy for premature ovarian insufficiency. Recently, Oviva Therapeutics, founded by Harvard molecular biologist Daisy Robinton, secured $11.5 million in seed funding to support the development of bioengineered anti-Müllerian hormone (AMH). Preclinical data indicate that the engineered AMH can protect immature follicles during chemotherapy. Moreover, this therapy has the potential to increase the number of mature oocytes, offering a possible improvement for in vitro fertilization (IVF) outcomes. Another Harvard-incubated ovarian therapeutic platform, Gameto, is investigating the application value of reprogrammed ovarian cells (granulosa cells and oocyte precursors) in assisted reproductive technologies.
Author: Chen Pin, Oriental Fortune Capital
*References
1.Qin, X., Zhao, Y., Zhang, T. et al. TrkB agonist antibody ameliorates fertility deficits in aged and cyclophosphamide-induced premature ovarian failure model mice. Nat Commun 13, 914 (2022).
2.Han, Fang, Xiaoming Guan, Wei Guo, and Bai Lu. et al. Therapeutic Potential of a TrkB Agonistic Antibody for Ischemic Brain Injury. Neurobiology of Disease (2019).
3.Guo, Wei, Keliang Pang, Yanbo Chen, Shudan Wang, Heng Li, Yihua Xu, Fang Han, et al. TrkB Agonistic Antibodies Superior to BDNF: Utility in Treating Motoneuron Degeneration. Neurobiology of Disease (2019).
4.Abdalla H & Thum MY. et al. An elevated basal FSH reflects a quantitative rather than qualitative decline of the ovarian reserve. Human Reproduction 19 893–898 ( 2004).
5. “Meta-analysis of the efficacy of the GnRH-a combined with GnRH-ant ultra-short protocol in patients with poor ovarian response,” Journal of Third Military Medical University, 2018, 40(4): 350-355.
6. “Expert Consensus on Ovulation Induction Medications in Assisted Reproductive Technology,” Reproduction & Contraception, Vol. 35, No. 4, 2015.
7. “Reproductive and Urogenital Sex Hormone Medications: A Surging $20 Billion Forecast,” Pharmaceutical Economic News.
8. “Panoramic View of the Assisted Reproductive Technology Industry: A Golden Track for Consumption Upgrading Benefiting from New Population Policies,” Ping An Securities.