Lilly Reportedly in Advanced Talks to Acquire Kelonia Therapeutics for Over $2 Billion, Bolstering In Vivo CAR-T Pipeline

Orna
Novel Full-Process Circular RNA (Orna) Therapy Developer

Johnson & Johnson
Medical Device R&D and Manufacturer
On April 19th, U.S. time, The Wall Street Journal reported that, according to relevant sources, Eli Lilly is in advanced negotiations to acquire Kelonia Therapeutics (hereinafter referred to as Kelonia). The deal is expected to exceed 2 billion U.S. dollars and may be officially announced on April 20th, local time. If the transaction is completed, this will be Eli Lilly's second major move in the in vivo CAR-T field, as it had just acquired Orna Therapeutics for 2.4 billion U.S. dollars in February 2026.
iGPS™ Technology Platform: Achieving Precise Modification of Lentiviral Vectors
Kelonia was founded in 2020 and is headquartered in Cambridge, Massachusetts. It was established by Dr. Kevin Friedman, who has over 20 years of experience in the cell and gene therapy field. The company's core competitiveness lies in its self-developed iGPS™ (in vivo Gene Placement System) technology platform.
Unlike the complex process of traditional CAR-T, which requires the collection of patients' T cells, followed by ex vivo modification, expansion, and reinfusion, iGPS™ utilizes engineered lentiviral vector particles to directly generate CAR-T cells in the patient’s body through a single intravenous infusion. The core breakthrough of this technological pathway lies in addressing two key issues: precise targeting and elimination of the need for lymphodepletion.
Lentiviral vectors naturally tend to enter cells through the low-density lipoprotein receptor, which can cause the vector to be "intercepted" by organs such as the liver, reducing delivery efficiency. To address this, Kelonia made two key modifications to the vector—
First, the use of VSV-G mutants reduces the vector's natural targeting of cells expressing low-density lipoprotein receptors, decreasing liver uptake; second, the expression of anti-CD3 single-chain antibodies on the viral surface enables the vector to precisely recognize and enter CD3-positive T cells. This dual modification of "detargeting + retargeting" allows the iGPS™ vector to bypass non-target organs and efficiently deliver therapeutic genes to T cells.
Before traditional CAR-T therapy, patients need to undergo lymphodepletion chemotherapy to eliminate existing lymphocytes in the body and make room for the reinfused CAR-T cells. This process itself can cause side effects such as bone marrow suppression and an increased risk of infection. Clinical data from Kelonia demonstrates that the iGPS™ vector can still robustly expand CAR-T cells in patients without prior lymphodepletion, which is undoubtedly a significant advantage of in vivo CAR-T compared to traditional therapies.
With this technology platform, Kelonia has attracted collaborations with Astellas and Johnson & Johnson. In February 2024, Xyphos, a subsidiary of Astellas, reached a partnership with Kelonia, with a potential total transaction value exceeding $875 million. In November 2025, Johnson & Johnson also quietly established a strategic collaboration with Kelonia to develop in vivo CAR-T therapies.
The First Anti-BCMA In Vivo CAR-T to Enter Multi-Center Clinical Trials
Kelonia's core pipeline, KLN-1010, is an in vivo CAR-T therapy targeting BCMA, designed for the treatment of relapsed/refractory multiple myeloma (RRMM).
In January 2026, KLN-1010 received FDA IND approval, becoming the first anti-BCMA in vivo CAR-T project to conduct a multicenter clinical trial in the United States. Prior to this, the therapy had already initiated the Phase I inMMyCAR study in Australia.
At the American Society of Hematology Annual Meeting in December 2025, Kelonia announced the data of the first four patients; at the American Association for Cancer Research Annual Meeting in April 2026, the company updated with more complete follow-up results.
Patient Baseline:All four patients were elderly and had undergone multiple lines of heavy treatment. The median age was 66 years (range: 61-72 years), with a median of 3.5 prior treatment lines (range: 3-5 lines). All patients had previously received autologous stem cell transplantation and anti-CD38 monoclonal antibody therapy, and all carried high-risk cytogenetic abnormalities. This is a truly "refractory" population.
Effectiveness:All four patients achieved minimal residual disease (MRD) negativity in the first month of treatment, with the longest followed-up patient remaining MRD-negative at five months. According to the International Myeloma Working Group criteria, all patients reached partial response in the first month, and the depth of response deepened over time. The first enrolled patient achieved complete response (pending confirmation) at six months.
CAR-T CellsLevel of amplification in vivoImpressive. On the 15th day, the percentages of CAR-positive T cells in blood samples reached 35%, 22%, 72%, and 85%, respectively. Comparing these figures with the marketed ex vivo CAR-T product CARVYKTI, the peak expansion of KLN-1010's CAR-T cells is on par with the latter—indicating that the number of CAR-T cells generated in vivo is fully comparable to traditional ex vivo preparation.
Safety:This is the most impressive part of KLN-1010. A total of 3 cases of cytokine release syndrome (CRS) were recorded, all of which were grade 1-2, with no occurrence of severe CRS of grade 3 or higher. The incidence of neurotoxicity was 0, with no reports of delayed neurotoxicity. Cytopenia events were rare and short-lived – a stark contrast to the severe and persistent bone marrow suppression commonly seen with traditional CAR-T therapies.
A notable point is that KLN-1010 has maintained good safety even at higher doses. The analysis suggests that this may be due to the underlying logic of its vector design, which provides a milder and more physiological activation signal by targeting T cells through CD3 scFv, effectively avoiding severe cytokine storms.
Lilly Bets Again This Year, Giants Rush to Develop In Vivo CAR-T
According to PitchBook data, Kelonia has raised less than $60 million in cumulative financing to date, with its last public valuation in April 2022 being just over $100 million. However, sources reveal that Eli Lilly is expected to bid over $2 billion this time, representing a premium of 20 times.
In the past, large pharmaceutical companies tended to invest heavily in acquiring projects only after Phase II clinical data had been read out, in order to reduce technical risks. However, recent trends in business development (BD) transactions over the past year indicate a shift, particularly in the in vivo CAR-T field. If Lixianlai is predicted to acquire KLN-1010 at a high premium while it has only completed Phase I trials with data from four patients and remains at a very early stage, this further demonstrates that the competition among industry giants in the in vivo CAR-T space is focused on securing platforms.
Meanwhile, this is not Lilly's first bet in this direction. In fact, global pharmaceutical giants have already launched a race in the in vivo CAR-T field for 2025-2026.
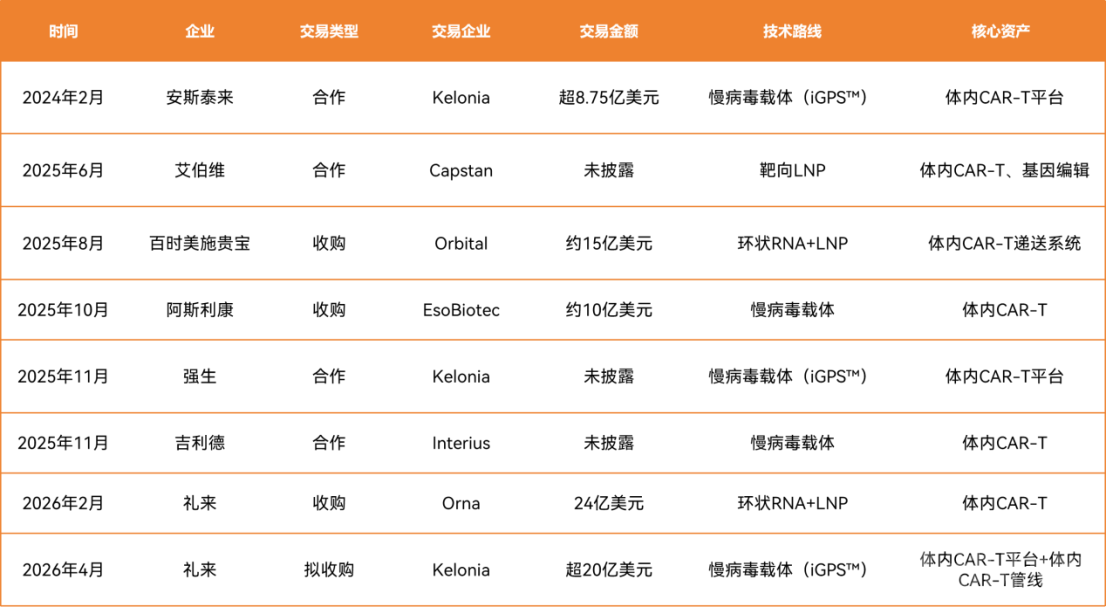
MNC's Significant Transactions in the In Vivo CAR-T Field
And several trends of MNC in the in vivo CAR-T layout are becoming increasingly clear.
Firstly, in terms of technology, the two routes of LNP delivery (Orna, Capstan) and lentiviral vector delivery (Kelonia, EsoBiotec, Interius) are running neck and neck, each with its own supporters. Currently, if the acquisition of Kelonia is successful, Eli Lilly is expected to become the only giant to simultaneously layout both routes, possessing two technical platforms: circular RNA + LNP and lentiviral vector.
In terms of transaction value, the publicly disclosed figures generally fall within the range of 1 to 2.5 billion US dollars. This price range reflects the industry's valuation consensus on in vivo CAR-T technology: technical feasibility has been preliminarily validated, but the risks associated with large-scale clinical trials and commercialization have yet to be fully mitigated. Industry giants are willing to pay a premium for an important entry point, but they are still some distance away from going all-in.
Moreover, the simultaneous acquisition of "technology platforms + core pipelines" is gradually becoming an established model. Many of the aforementioned transactions focus not only on specific products but also emphasize technology platforms. This aligns with the core competitive logic of in vivo CAR-T — focusing on the delivery system itself, where the platform determines everything.
Therefore, if Eli Lilly really steps in, it would be like providing double insurance for the in vivo CAR-T technology route, ensuring that no matter which delivery route is taken, they won't fall behind.
From the perspective of indications, it fills a key gap in the blood cancer pipeline. Eli Lilly has strengths in solid tumors (especially breast cancer and lung cancer) in the oncology field, while its presence in blood cancers is relatively weak. BCMA-targeted multiple myeloma is one of the most successful indications for CAR-T therapy, with Legend Biotech's CARVYKTI already demonstrating the enormous potential of this market. By acquiring Kelonia, Eli Lilly can quickly gain access to a BCMA CAR-T pipeline that has been validated in humans and offers differentiated safety advantages.
More importantly, Kelonia's platform technology is scalable—iGPS™ can not only deliver the CAR gene but also other therapeutic transgenes, making it a technical platform that can continuously produce pipelines for both hematologic and solid tumors.
Further down the line are the perennial issues of cost and accessibility. Compared to the traditional autologous CAR-T costs and quality expenses, the core commercial value of in vivo CAR-T lies in transforming cell therapy into a "standardized drug." Single infusion, no ex vivo manipulation, no lymphodepletion—if this model is validated in larger-scale clinical trials, the cost and accessibility of CAR-T therapy will undergo a fundamental transformation.
By 2025, Eli Lilly has become the world's most valuable pharmaceutical company. The substantial cash flow generated by its GLP-1 products has provided ample resources for its aggressive investment in next-generation technology platforms. To avoid over-reliance on a single blockbuster drug, building a pipeline reserve across next-generation technology platforms such as in vivo CAR-T, gene therapy, and RNA therapeutics has become an inevitable choice for large pharmaceutical companies to navigate cycles and hedge risks.
The deal between Eli Lilly and Kelonia has not been officially announced, but regardless of whether this deal is ultimately reached, the voice of "2026 is becoming a turning point for the industrialization of in vivo CAR-T" is still amplifying.