Bariatric Surgery: The Ultimate Weapon Against Obesity and Diabetes – Who Will Lead the Blue Ocean Market for Surgical Devices?
Weight loss is not merely a means for young people to pursue beauty, but an essential path toward health for individuals with obesity.
With China’s economic development and accelerating urbanization, overweight and obesity are affecting younger populations, with prevalence rates continuing to rise. This trend contributes to conditions such as diabetes, hyperlipidemia, and obstructive sleep apnea, adversely impacting patients’ quality of life and survival rates, thereby necessitating weight-loss interventions. The RMB 100-billion weight-loss market continues to witness sustained high demand.
In July, semaglutide, a glucose-lowering drug used by some individuals for weight loss, experienced stockouts in pharmacies in certain regions. In August, Beijing Biosis Healing Biological Technology Co., Ltd.’s product for sleeve gastrectomyBiorich™ Anastomotic Reinforcement and Repair for GastrectomyThe patch received regulatory approval. Around the same time, Standard Bariatrics, a company providing solutions for sleeve gastrectomy, was acquired by global medical device giant Teleflex for $300 million.
Sectors within the weight-loss ecosystem—including exercise, meal replacements, weight-loss medications, and bariatric surgery—are beginning to capture the attention of both the market and investors.
 China’s Exclusive, Innovative Product — Boruiqiang™Approval Document for the Market Launch of Anastomotic Reinforcement and Repair Patch
China’s Exclusive, Innovative Product — Boruiqiang™Approval Document for the Market Launch of Anastomotic Reinforcement and Repair Patch
In recent years, obesity has become a global challenge.
According to statistics from the World Health Organization (WHO), nearly 2 billion people worldwide are overweight or obese. The obesity rate nearly tripled between 1975 and 2016, with up to 2.8 million deaths annually attributed to overweight or obesity.China has the highest number of obese individuals in the world. Currently, the prevalence of overweight and obesity among adults in China stands at 34.3% and 16.4%, respectively, meaning that more than half of the adult population is affected by overweight or obesity.Moreover, substantial evidence indicates that Chinese individuals have higher body fat percentages; at the same body mass index (BMI) level, they face greater cardiovascular risk and all-cause mortality than Whites.
Obesity not only affects body shape but is also a major risk factor for non-communicable diseases, being closely associated with type 2 diabetes, hyperlipidemia, hyperuricemia, cardiovascular and cerebrovascular diseases, and respiratory disorders. In addition to its physical impacts, individuals with obesity are at a higher risk of developing mental health conditions.
From the patient’s perspective, managing obesity is expected to improve quality of life and reduce mortality risk; from a health economics standpoint, it can lower healthcare expenditures. Studies show that individuals with obesity receive 2.4 times as many prescriptions as those with normal weight, experience longer hospital stays, and undergo more complex and costly treatments.
As China’s economic development and people’s quality of life improve, obesity has been recognized as a disease requiring clinical intervention, making weight loss a prominent focus. The large target population creates substantial market opportunities.
China’s weight-loss market is vast, with the anti-obesity drug segment alone valued at tens of billions of yuan, attracting major players such as Eli Lilly and Hengrui Medicine. Spurred by the pandemic, online and offline exercise-based weight-loss programs have gained momentum, exemplified by Keep’s filing of its prospectus. Meanwhile, bariatric surgery, regarded as the “ultimate” weight-loss intervention, has seen a rapid increase in procedure volume in recent years, driving growth in the related medical device market.
Current weight-loss interventions can be broadly categorized into three types: lifestyle modifications, pharmacological therapy, and bariatric surgery. The first two represent more common traditional treatment approaches. Weight loss through dietary restriction and exercise among individuals with obesity often lacks sustainability and yields slow results. Particularly for patients with severe obesity, adherence to a scientifically designed exercise regimen combined with reasonable dietary control is required; however, the prolonged treatment duration makes long-term compliance difficult, and weight regain is common.
The weight-loss drug market is uneven in quality, with public perception even encompassing unregulated products lacking manufacturer details, quality certifications, or production licenses. Currently, only one weight-loss medication has been approved for marketing in China. It poses health risks for some individuals with obesity to use diabetes medications as substitutes. Moreover, pharmacological treatment often comes with significant side effects, such as appetite suppression and drowsiness.
In summary,Bariatric surgery achieves therapeutic goals through procedures such as sleeve gastrectomy and gastrointestinal bypass, and it is the only intervention capable of achieving sustained short- and long-term weight loss while improving comorbidities such as diabetes and hyperlipidemia.However, compared with the first two weight-loss approaches, bariatric surgery requires more stringent patient selection, and patients must also invest considerable money and time in the short term. Therefore, it bears repeated emphasis that bariatric surgery is not a shortcut to slimming down, but rather a more effective treatment for obesity.
Bariatric surgery originated in the 1960s. In clinical practice, Mason and Ito, regarded as the pioneers of bariatric surgery, observed that patients with peptic ulcer disease were able to maintain a low body weight after undergoing subtotal gastrectomy. Consequently, they performed the earliest form of gastric bypass surgery, which involved creating a small gastric pouch with preserved partial gastric volume and anastomosing the stomach to the small intestine following distal subtotal gastrectomy, achieving ideal weight loss outcomes.
With the continuous advancement of medical technology, bariatric procedures such as gastric bypass and gastrectomy have emerged. The application of laparoscopy has further propelled bariatric surgery into a more minimally invasive and precise era. Long-term clinical practice has revealed that bariatric surgery not only effectively reduces body weight in obese patients but also improves glucose metabolism disorders and alleviates metabolic diseases such as type 2 diabetes. Consequently, bariatric surgery is also referred to as metabolic and bariatric surgery.
Bariatric surgery is well-established in Europe and the United States, whereas China’s bariatric surgery industry, though a late starter, has developed rapidly and holds substantial growth potential.
According to statistics from the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO), the global number of bariatric surgery cases reached 630,000 in 2016, with the United States accounting for 220,000 cases, approximately one-third of the global total. Statistical data from 61 countries and regions worldwide in 2019 showed that the total annual number of bariatric and metabolic surgeries exceeded 830,000, among which the United States reported 335,124 cases.
Bariatric and metabolic surgery has only a 20-year development history in China. In 2000, the first and second bariatric surgeries were performed in Shanghai and Guangzhou, respectively. As of 2021, statistical data from 180 hospitals or bariatric centers in the Chinese Obesity and Metabolic Surgery Database (COMES Database) showed that the number of bariatric and metabolic surgeries in China reached 23,040 cases, with the estimated actual national total being approximately 25,208 cases. However, the total number of obese individuals in China has exceeded 90 million, including over 12 million with severe obesity, resulting in a penetration rate of bariatric and metabolic surgery of only 2‰.
Based on data from the COMES Database statistical report, the estimated number of bariatric surgeries performed nationwide in China was 1,950 in 2012 and 25,208 in 2021. The compound annual growth rate (CAGR) of bariatric surgery volume in China over the past decade was calculated to be 29.17%. Projections indicate that the annual number of bariatric surgeries nationwide will exceed 50,000 within the next three years and grow to nearly 200,000 within the next ten years. The market for bariatric and metabolic surgery in China is currently in a phase of rapid development and expansion.
From 2019 to 2021, the number of full-time bariatric surgeons rapidly increased from 342 dedicated physicians across 109 hospitals to 513 dedicated physicians across 164 hospitals. The three-year compound annual growth rate (CAGR) for the recorded number of full-time practitioners was 14.47%. Over the next five years, more than 1,000 physicians in China will be dedicated to practicing bariatric surgery.

Updated Statistical Data and CAGR Calculation for the 2019–2021 Chinese Database of Obesity and Metabolic Surgery
*Due to data source limitations, there is a significant deviation from the estimated surgical volume; CAGR is for reference only
Nevertheless, the number of physicians falls far short of market demand. Key factors currently constraining industry development include specialized training in bariatric surgery, patient education, and a substantial shortage of qualified specialists.
Currently, four types of bariatric surgeries are primarily performed in clinical practice. Among them, adjustable gastric banding is gradually being phased out of surgical practice due to its propensity to cause complications such as nausea, vomiting, and infection. In contrast, sleeve gastrectomy, characterized by its high safety and efficacy profile as well as abundant clinical evidence, has become the most prevalent bariatric procedure worldwide.In 2021, a total of 18,533 sleeve gastrectomies were performed in China, accounting for 80.4% of the annual volume of bariatric surgeries. Moreover, compared with 2020, the number of sleeve gastrectomies increased substantially by 86%.
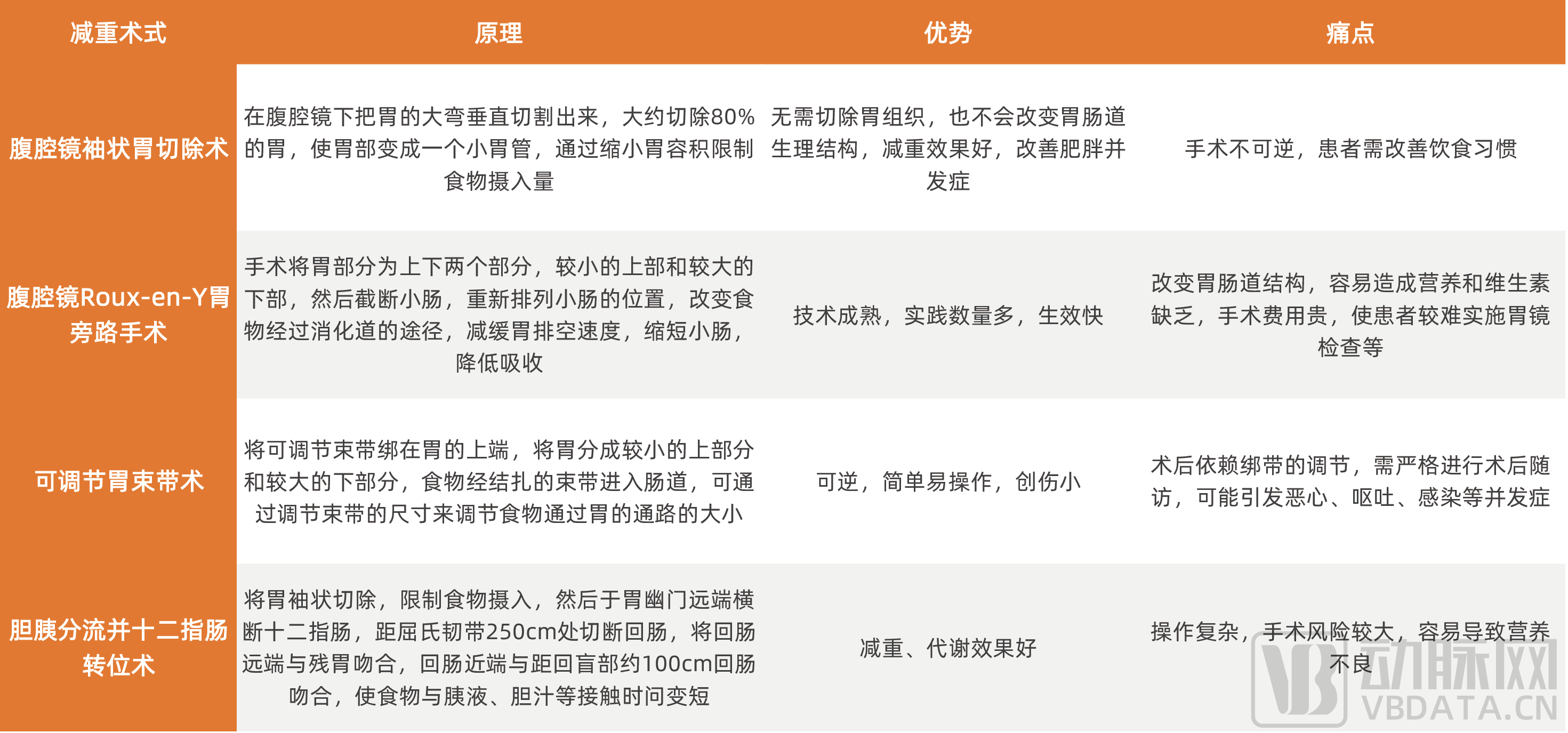
Four Common Types of Bariatric Surgery
According to the 2019 Chinese Guidelines for Surgical Treatment of Obesity and Type 2 Diabetes, the current indications for bariatric surgery in patients with simple obesity mainly include: (1) Bariatric surgery is actively recommended for patients with simple obesity and a BMI ≥37.5 kg/m²; surgery is recommended for patients with a BMI of 32.5–37.4 kg/m²; for patients with a BMI of 27.5–32.4 kg/m² whose condition is difficult to control through lifestyle modifications and pharmacological therapy, and who meet at least two components of metabolic syndrome or have comorbidities, surgery may be considered after comprehensive evaluation; (2) For men with a waist circumference ≥90 cm and women with a waist circumference ≥85 cm, where imaging studies indicate central obesity, the recommendation level for surgery may be appropriately increased following consultation with a multidisciplinary team; (3) The recommended age range for surgery is 16–65 years.
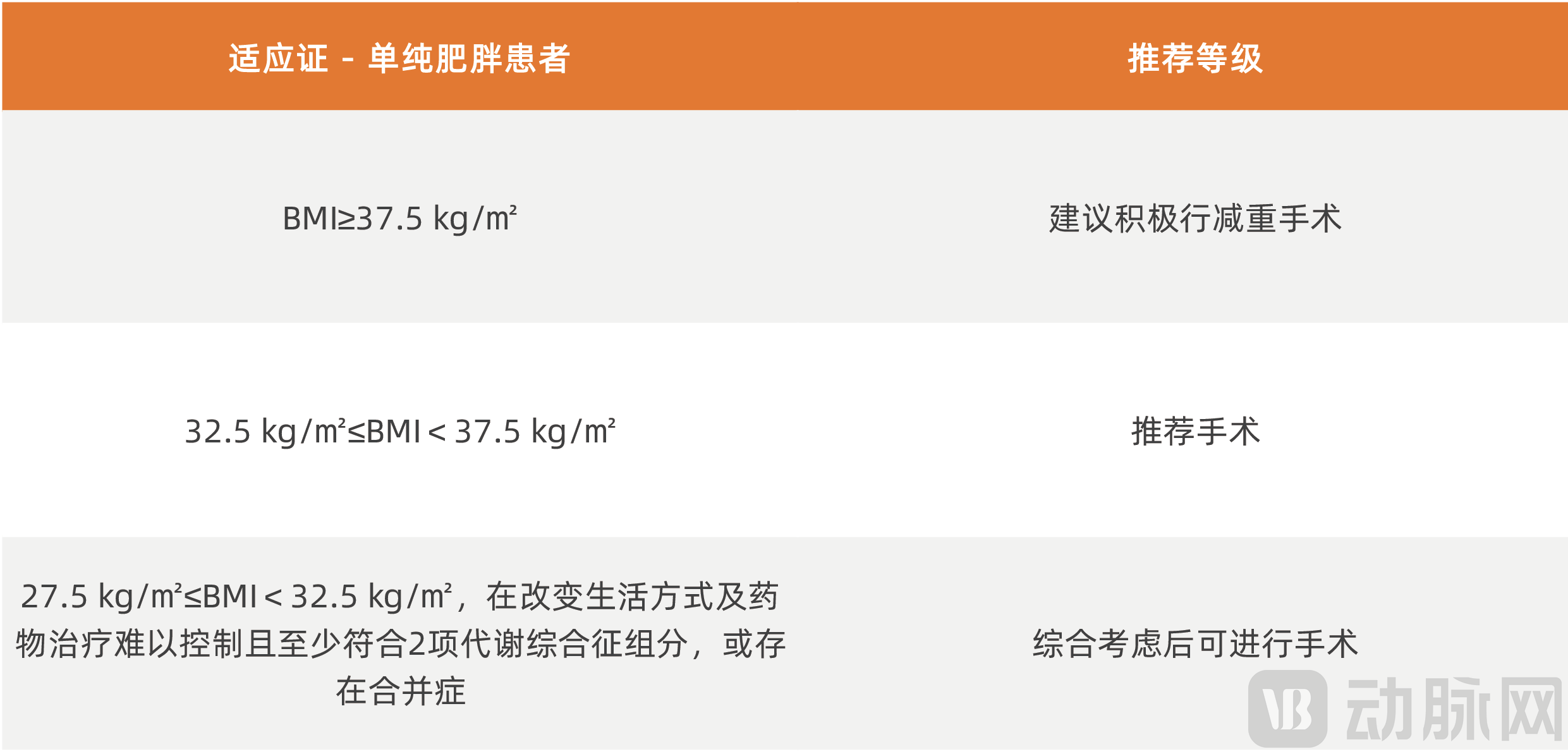
Indications for Bariatric Surgery in Patients with Simple Obesity
Note: (1) Components of metabolic syndrome (as defined by the International Diabetes Federation) include: elevated triglycerides (TG, fasting ≥1.70 mmol/L); reduced high-density lipoprotein cholesterol (HDL-C, fasting <1.03 mmol/L in men and <1.29 mmol/L in women); and hypertension (systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥85 mmHg; 1 mmHg = 0.133 kPa).
(2) Comorbidities include abnormal glucose metabolism and insulin resistance, obstructive sleep apnea-hypopnea syndrome (OSAHS), non-alcoholic steatohepatitis (NASH), endocrine dysfunction, hyperuricemia, male sexual dysfunction, polycystic ovary syndrome, osteoarthritis, and renal dysfunction, particularly in the presence of cardiovascular risk factors or chronic complications such as type 2 diabetes mellitus (T2DM).
(3) It has certain efficacy for patients with a BMI of 27.5–32.5, but there is insufficient evidence from both domestic and international sources to support its long-term efficacy; therefore, cautious implementation is recommended.
(4) If dual-energy X-ray absorptiometry (DEXA) measurements of android fat content correlate with abdominal and visceral fat distribution, a significant increase in android fat content suggests central obesity; alternatively, MRI may be used to assess abdominal visceral fat content.
For patients with type 2 diabetes mellitus (T2DM), the indications for surgery mainly include: (1) Patients with T2DM retain a certain degree of insulin secretory function. (2) For those with a BMI ≥32.5 kg/m², bariatric surgery is actively recommended; for those with 27.5 kg/m² ≤ BMI <32.5 kg/m², surgery is recommended; for those with 25 kg/m² ≤ BMI <27.5 kg/m², if glycemic control is difficult to achieve through lifestyle modifications and pharmacological therapy, and at least two components of metabolic syndrome are present or comorbidities exist, surgery should be undertaken with caution. (3) For patients with 25 kg/m² ≤ BMI <27.5 kg/m², if waist circumference is ≥90 cm in males or ≥85 cm in females, and imaging studies suggest central obesity, the recommendation level for surgery may be appropriately elevated after consultation with a multidisciplinary team. (4) The recommended age range for surgery is 16–65 years.
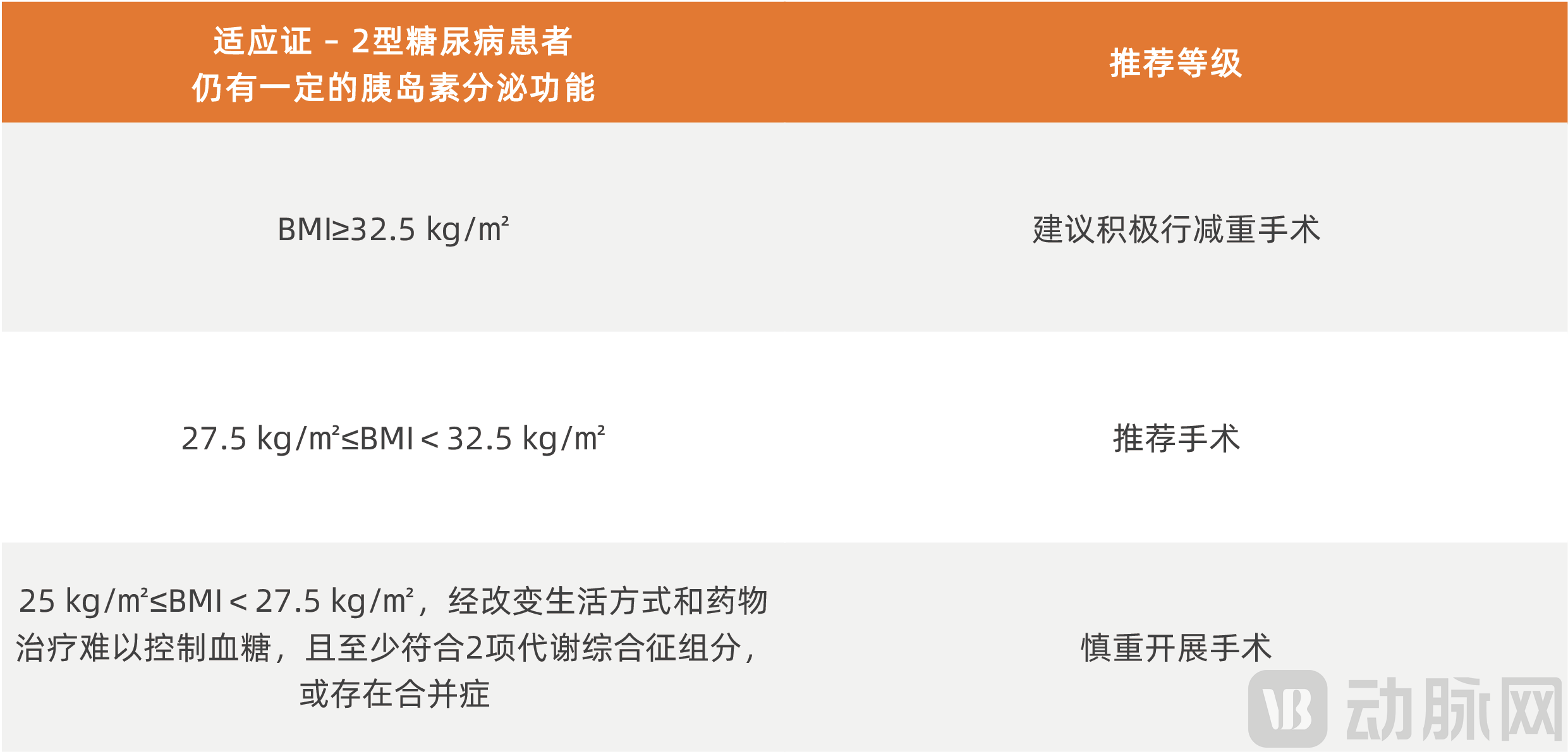
Indications for Bariatric Surgery in Patients with Type 2 Diabetes
As the global obesity crisis intensifies, with a rising number of obese patients suffering from comorbidities such as diabetes, traditional interventions like exercise and pharmacotherapy are no longer sufficient to address complication management, leaving a substantial gap in weight-loss treatment. The broader adoption of sleeve gastrectomy is poised to become the “ultimate weapon” for patients with obesity and type 2 diabetes.
As healthcare standards continue to improve, medical insurance in some regions has begun to cover sleeve gastrectomy, the number of specialized bariatric surgeons is increasing, and surgical volume is expected to continue growing.The surgical procedures and techniques for sleeve gastrectomy are being continuously standardized, with the successive release of the “Guidelines for Laparoscopic Sleeve Gastrectomy” and the “Guidelines for Robot-Assisted Sleeve Gastrectomy.”
Dividing the stomach into two parts is the most critical step in sleeve gastrectomy, with anastomosis being the key. The remaining gastric wall must be securely closed to prevent leakage of gastric contents from the incision edges into the abdominal cavity, while blood vessels at the incision margins must also be properly sealed to avoid bleeding and infection. Under laparoscopy, manual suturing is somewhat limited; staplers can perform tasks that are difficult to achieve with manual suturing, offering effective and safe anastomosis, and thus have gradually become widely adopted in clinical practice.
However, intraoperative anastomotic bleeding and postoperative anastomotic leakage remain significant complications associated with gastrectomy. These issues primarily arise from impaired tissue healing due to excessive anastomotic tension, local tissue edema, or hypoproteinemia, with incidence rates ranging from 1.7% to over 10%. Leakage of gastrointestinal fluids at the anastomosis site may lead to intra-abdominal infection or even peritonitis, necessitating reoperation. This not only increases the physical and financial burden on patients but may also be life-threatening.
Therefore,To further promote the adoption of sleeve gastrectomy, it is essential to first address the issues of anastomotic leakage and bleeding.
In 2020, the European Association for Endoscopic Surgery (EAES) released clinical practice guidelines for bariatric surgery, summarizing the latest evidence related to bariatric procedures. The guidelines strongly recommend the use of staple line reinforcement products in sleeve gastrectomy to reduce perioperative complications, including overall mortality and bleeding incidence. However, prior to this, China lacked effective staple line reinforcement products, and there was no clinical consensus. The absence of such products and guidelines has, to some extent, hindered the adoption of sleeve gastrectomy.
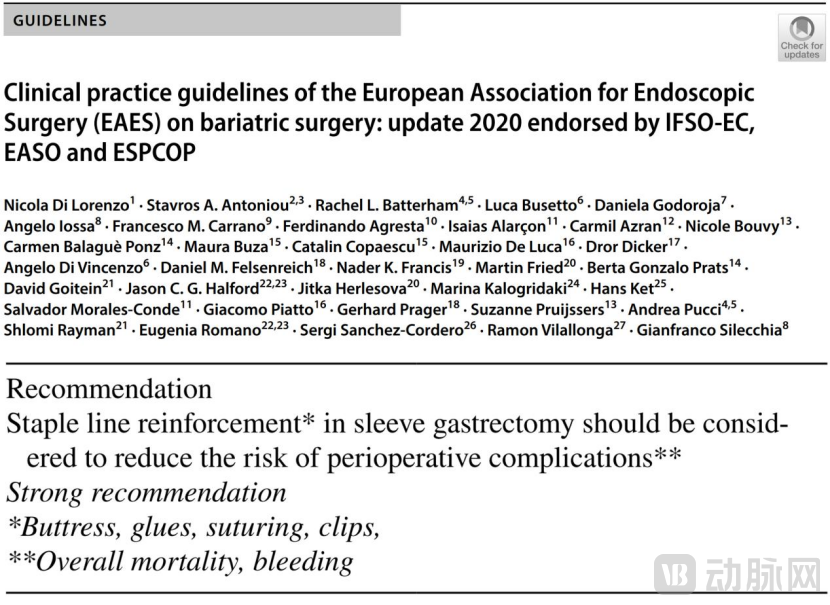
Clinical Practice Guidelines for Bariatric Surgery 2020 Edition – European Association for Endoscopic Surgery (EAES): Strong Recommendation for the Use of Staple Line Reinforcement Products in Sleeve Gastrectomy
Boruiqiang™ Anastomotic Reinforcement and Repair Patch is a significant solution derived from clinical practice.
This August, the first breakthrough emerged in China’s previously untapped market for anastomotic reinforcement and repair products. Biosis Healing’s Boruiqiang™ Anastomotic Reinforcement and Repair Patch has received approval for use in distal gastrectomy, proximal gastrectomy, sleeve gastrectomy, and gastrointestinal anastomosis.
This is China’s first comprehensive line of anastomotic reinforcement and repair products, including tubular, flat patch, and circular types. It is also the world’s first anastomotic reinforcement and repair product made from SIS (small intestinal submucosa) material for use with linear staplers. The Boruiqiang™ Anastomotic Reinforcement Patch is compatible with products from most major stapler manufacturers on the market, meeting clinical needs for gastrointestinal anastomosis.
Boruiqiang™ Anastomotic Reinforcement Patch is used to reinforce anastomotic sites, with its mechanism of action primarily involving both physical reinforcement and biological repair.
Physical Reinforcement Effect:Ensures uniform compression across the tissue cross-section, distributes stress at suture holes, reinforces anastomotic tissue, and significantly reduces the incidence of anastomotic bleeding and postoperative anastomotic leakage;Bioremediation:Boreiqiang™ Anastomotic Reinforcement Patch utilizes non-crosslinked ECM-derived SIS biomaterial, preserving the natural structure and composition of the extracellular matrix (ECM). Rich in bioactive substances, it promotes rapid healing of the anastomosis and is completely degraded and absorbed within 3–4 months after implantation.
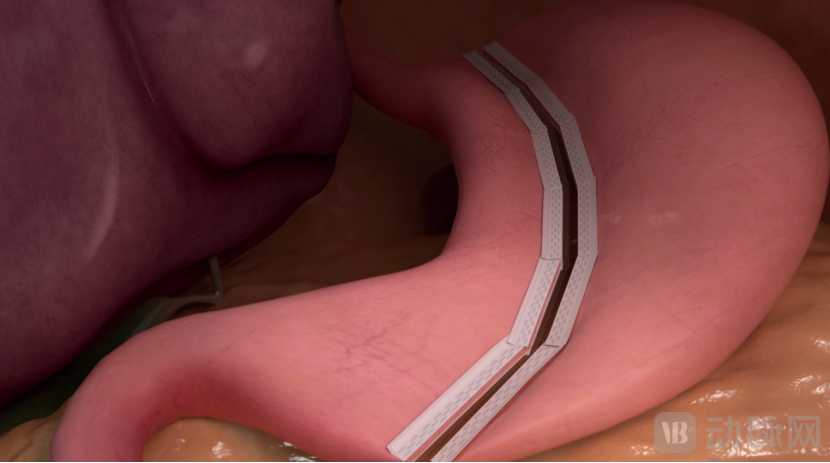
Schematic Diagram of the Application of Boruiqiang™ Anastomotic Reinforcement Patch in Sleeve Gastrectomy
A large-sample meta-analysis, which included 16,967 articles (covering 56,309 cases in studies on anastomotic leakage and 41,864 cases in studies on anastomotic bleeding), demonstrated that the application of anastomotic reinforcement products in sleeve gastrectomy and gastric bypass surgery can significantly reduce the incidence of bleeding and anastomotic leakage. Furthermore, biological materials for anastomotic reinforcement were found to be superior to synthetic materials.

Large-Sample Meta-Analysis
In addition to its innovative products, Beijing Biosis Healing Biological Technology Co., Ltd. is actively promoting the establishment of expert consensus on the use of anastomotic reinforcement patches in gastrointestinal surgery in China, which is expected to further standardize gastrointestinal anastomosis procedures.
Beijing Biosis Healing Biological Technology Co., Ltd. has been deeply engaged in the field of SIS biomaterials for many years, with multiple research findings published in top-tier international journals such as *Advanced Healthcare Materials*. The company’s SIS biomaterials are derived from porcine small intestinal submucosa (SIS) matrix and manufactured using a non-crosslinked process. This approach preserves natural bioactive components, ensuring excellent biocompatibility, prevention of tissue adhesion, and resistance to infection. Upon implantation, the material actively induces tissue regeneration and degrades as the regeneration process is completed.
Beijing Biosis Healing possesses a fully independent intellectual property rights SIS material platform and has developed a portfolio of over ten Class III implantable products addressing clinical needs across neurosurgery, otology, oral and maxillofacial surgery, thoracic surgery, abdominal wall surgery, and colorectal surgery. Furthermore, Beijing Biosis Healing offers nearly 20 types of surgical instruments, including linear cutters, endoscopic cutters, circular staplers, trocars, and ligation clips.
Clinically, Biosis Healing provides physicians with a comprehensive suite of surgical instruments for sleeve gastrectomy, including staplers, trocars, ligation clips, and staple line reinforcement patches, offering an end-to-end solution under a single brand throughout the entire surgical procedure.
As previously mentioned, with advancements in healthcare and heightened public health awareness, issues such as obesity and metabolic disorders that impact quality of life and even survival are receiving greater attention. Consequently, the weight loss market will continue to expand and become increasingly standardized. On the basis of effectively managing complications such as anastomotic leakage and hemorrhage, the volume of bariatric surgeries will continue to grow.
Currently, few medical device companies have focused on the bariatric surgery sector, leaving the market in a blue-ocean stage characterized by small and fragmented participation. However, Beijing Biosis Healing Biological Technology Co., Ltd has recognized the growth potential of the bariatric surgery market through years of clinical observation and market accumulation, and has continued to deepen its engagement in this field. With the approval of its exclusive anastomotic reinforcement patch product in China, the company has begun to demonstrate clear leadership qualities.
Overall, Beijing Biosis Healing Biological Technology Co., Ltd. boasts a blockbuster product in anastomotic reinforcement patches and provides a comprehensive solution with a full set of instruments for gastric volume reduction surgery, demonstrating technological and product leadership. Currently, the company has attracted interest from multiple investors and is well-positioned to capture market share ahead of competitors.
References:
1、《Clinical Benefit of Gastric Staple Line Reinforcement (SLR) in Gastrointestinal Surgery: a Meta-analysis》
2. “Chinese Database for Obesity and Metabolic Surgery: 2021 Annual Report”
3、Shikora SA, Mahoney CB. Obes Surg. 2015 Jul;25(7):1133-41.
4、Di Lorenzo N, Antoniou SA, Batterham RL, Busetto L, et al. Surg Endosc. 2020 Jun;34(6):2332-2358.