2022 Immune Cell Therapy Industry Report: Prospects from a Technology Pathway Perspective
Preface
In August 2017, the U.S. FDA approved Kymriah, the world’s first chimeric antigen receptor T-cell (CAR-T) therapy, for the treatment of relapsed or refractory B-cell acute lymphoblastic leukemia in patients up to 25 years of age. The indication was later expanded in 2018 to include adult patients with relapsed or refractory diffuse large B-cell lymphoma, rapidly igniting enthusiasm in the field. In 2021, China’s National Medical Products Administration (NMPA) consecutively approved two CAR-T products from Fosun Kite and JW Therapeutics for market launch. Furthermore, in 2022, Legend Biotech’s Carvykti, indicated for the treatment of adult patients with relapsed or refractory multiple myeloma, received sequential approvals in the United States and the European Union. These milestones have further accelerated research and development in the field of immune cell therapy. Throughout the evolution of immune cell therapy, various technological approaches—including CAR-T, TCR-T, CAR-NK, and tumor-infiltrating lymphocytes (TIL)—have emerged as competitive frontiers, each demonstrating unique therapeutic potential.
Based on this, VCBeat has authored the “2022 Report on the Immune Cell Therapy Industry,” and in Part I of its series, it focuses on addressing the following questions:
1. What is the current status of research and development for immune cell therapy, and how mature is its development?
2. What are the tumor-killing mechanisms of various types of immune cell therapies, and what are their primary indications?
3. What are the core bottlenecks currently facing immune cell therapy, and what are the strategies for breakthrough?
4. How do the development prospects of various technical pathways compare when comprehensively evaluated from the dimensions of safety, efficacy, durability, and commercial viability?
To clarify the aforementioned issues, VCBeat Research Institute conducted extensive industry surveys and, in conjunction with its own research findings, sought toIndustry Overview, Technological Pathways, Development Opportunities and Challenges, and Future Trend AnalysisThis report provides a comprehensive analysis of the immune cell therapy industry across multiple dimensions, aiming to deliver valuable insights for industry stakeholders and participants. This installment primarily focuses on technological pathways, while subsequent reports in the series will delve into manufacturing processes.
(Note: To access the full report, please scan the QR code at the end of the document.)
Immunocyte Therapy “Live Drugs” Show Promising Efficacy,Global R&D Momentum Remains Strong
1.1 Immune Cell Therapy—“Living Drugs” in Tumor Immunotherapy, with Prominent Efficacy Advantages
■ Immunocyte Therapy
Adoptive Cell Transfer Therapy (ACT) generally refers to the process of harvesting and isolating immune cells from tumor patients or allogeneic donors, followed by in vitro expansion, culture, screening, and identification, before reinfusing them into the patient. This approach enhances the recognition and cytotoxicity against tumor cells, thereby treating malignant tumors.
Source: National Cancer Institute, VCBeat
Classified by whether they are genetically engineered. Genetically modified:Composed of two structural components that provide targeting and cytotoxicity, respectively. Common examples include CAR-T, TCR-T, CAR-NK, and CAR-M therapies. Ex vivo genetic engineering endows immune cells with the ability to specifically recognize tumor cells (targeting), which are then infused back into the patient to achieve specific killing of tumor cells (cytotoxicity).Unmodified:Common types include TILs, LAK cells, CIK cells, DCs, NK cells, Tregs, CTLs, and γδT cells.
Classification by Cell Source. Autologous Type:Immune cells isolated from the patient themselves, “1v1” personalized service, high cost, long waiting period.General-purpose:Donor-derived, “1-to-many” off-the-shelf ready-to-use products with low cost.
■ Indications
Last-line treatment for malignant tumors (potentially moving to earlier lines in the future), including hematologic malignancies and solid tumors.
■ Advantages
Druggability:Compared with traditional drug development based on the protein level, it avoids undruggable targets (e.g., CAR-T uses viral vectors to carry CAR genes into T cells for transduction, enabling the expression of CAR proteins).
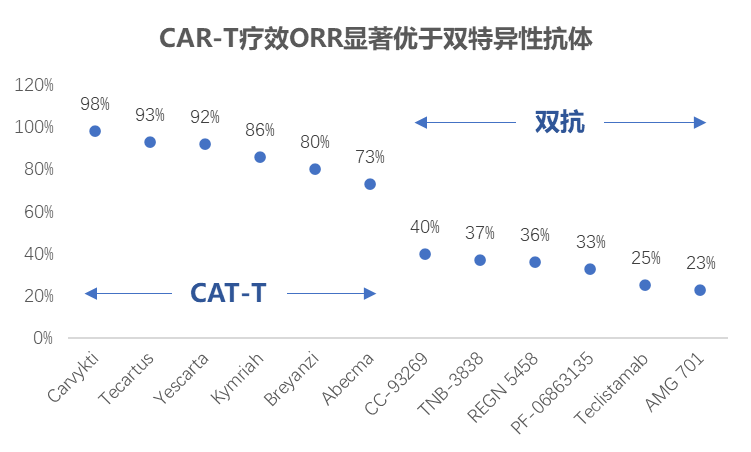
Excellent Efficacy:The objective response rate (ORR) of PD-1/PD-L1 antibody drugs is generally unsatisfactory, typically ranging from 10% to 30%. In contrast, the ORR for several FDA-approved CAR-T therapies generally falls between 70% and 90%. Furthermore, for patients resistant to PD-1 inhibitors, Iovance, a leader in tumor-infiltrating lymphocyte (TIL) therapy, reported at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting that the ORR of LN-144 in heavily pretreated melanoma reached 36%.
Source: Public information, compiled by VCBeat.
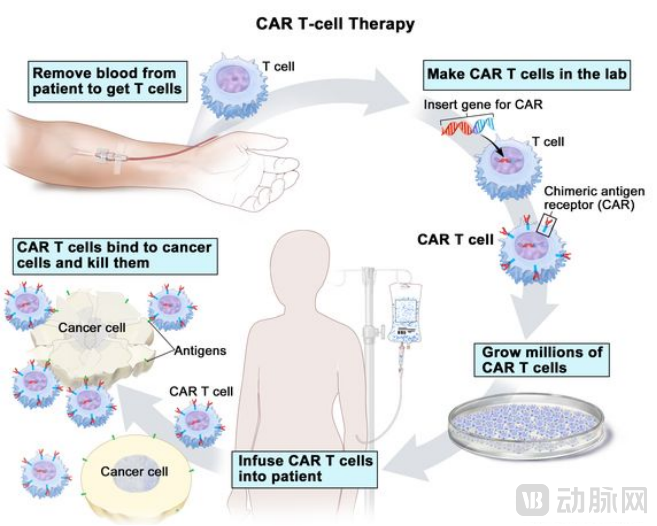
■ Treatment Process (Autologous as an Example)
Collect peripheral blood from the patient and isolate T cells — introduce pre-designed CAR genes into the T cells via genetic engineering — screen for CAR-T cells that successfully express CAR proteins on their cell surface — expand and culture in vitro — infuse back into the patient to target tumors with close monitoring.
■ This report focuses on
Common immune cell therapies include CAR-T, TCR-T, CAR-NK, and TIL. Among these, CAR-T therapy is the most mature, with eight products approved for market launch globally (six approved by the FDA and two licensed in China), demonstrating significant efficacy in hematologic malignancies.
1.2 First-generation CARs overcome the MHC restriction of TCRs, and each generation of CARs aims to enhance cell proliferation and cytotoxicity
First-generation CARs were derived from improvements to the TCR, thereby overcoming MHC restriction.
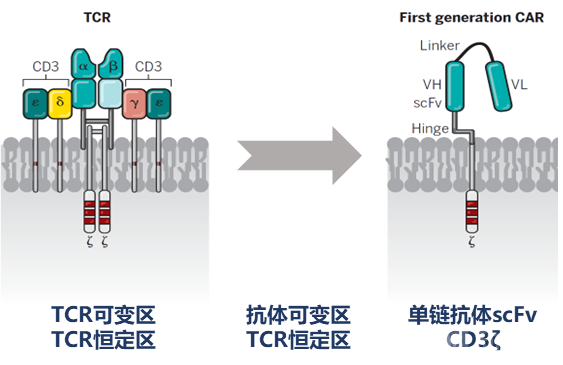
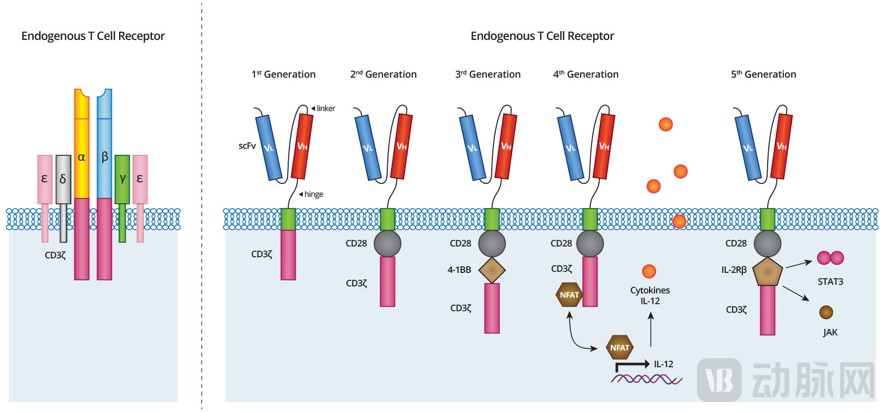
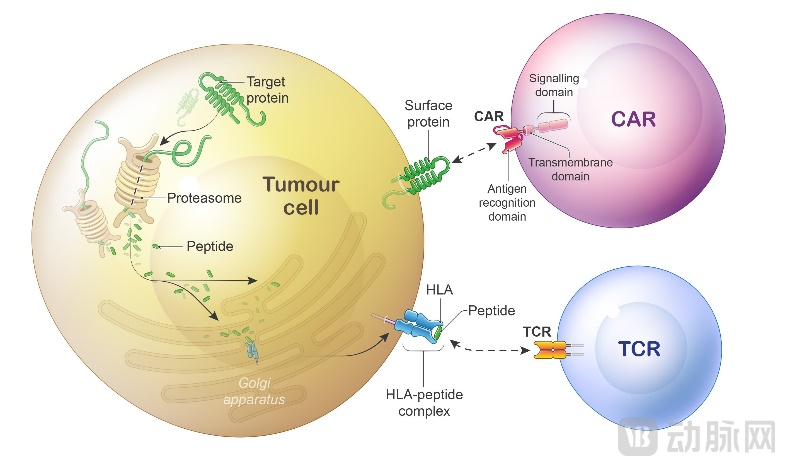
TCR (T cell receptor): MHC restriction.TCR belongs to the immunoglobulin family and forms a heterodimer consisting of an α chain and a β chain linked by disulfide bonds. The extracellular structure of TCR is highly similar to the Fab fragment of antibodies; however, unlike antibody variable regions that can directly bind antigens, TCR variable regions can only recognize antigens presented as complexes with major histocompatibility complex (MHC) molecules. Nevertheless, tumor cells can downregulate the expression of MHC class I molecules to evade immune surveillance.
First-generation CAR (chimeric antigen receptor): non-MHC restricted.To overcome the MHC restriction of TCRs, in 1989, a team led by Israeli scientist Zelig Eshhar replaced the variable regions of the TCR with antibody variable regions, constructing a chimeric receptor composed of antibody variable regions and TCR constant regions, and demonstrated that this chimeric receptor could directly bind to antigens.1993: The First Generation of CARs Emerged:Scientists have simplified the construction of both the antibody variable region and the TCR constant region, replacing the extracellular domain of the TCR with a single-chain variable fragment (scFv). This is because the scFv, formed by artificially linking the variable regions of the antibody heavy and light chains, retains the antigen-recognition capability similar to that of the antibody Fab fragment, andFusing the single-chain antibody scFv directly with the activating receptor CD3ζ into a single protein(Because TCR forms a non-covalent complex with CD3 upon activation and transduces extracellular signals into the cell via the CD3ζ subunit), and demonstrated its ability to specifically kill tumor cells in vitro.
Source: Science, VCBeat
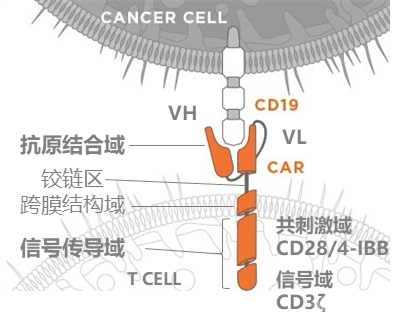
Core Structure of CAR: Extracellular Antigen-Binding Domain & Intracellular Signaling Domain
Extracellular Antigen-Binding Domain: Provides targeting capability and specifically recognizes tumor-associated antigens.Namely, the single-chain variable fragment (scFv), which consists of the variable heavy chain (VH) and variable light chain (VL) of an antigen-specific immunoglobulin. For example, tumor cells in patients with acute lymphoblastic leukemia express CD19 on their surface; the scFv of the constructed CAR protein can recognize CD19, thereby activating T cells to kill the tumor cells.
Intracellular Signaling Domain: Determines the Proliferation, Activation, and Cytotoxic Capacity of Immune Cells.The foundational component of first-generation CARs is CD3ζ. With iterative optimization, co-stimulatory molecules and cytokines have been incorporated to further enhance the potency of immune cells.
Source: Public information, VCBeat.
Optimization of CAR Structures Across Generations Based on Intracellular Co-stimulatory Domains to Enhance Proliferation, Activation, and Cytotoxicity
First Generation: Contains only the activating receptor CD3-ζ. The cells cannot be fully activated, resulting in slow expansion, poor persistence, and weak anti-tumor efficacy.
Second Generation: One co-stimulatory molecule, CD28 or 4-1BB. Enhances T cell proliferation and extends survival time.
Third generation: Two co-stimulatory molecules, CD28 and 4-1BB. Further enhances T cell proliferation and activation.
Fourth generation: Pro-inflammatory cytokine IL-12. Recruits natural killer (NK) cells and enhances the cytotoxic activity of T cells.
Fifth Generation: Cytoplasmic IL-2Rβ chain domain with STAT3/5 binding sites. Overcomes the tumor-suppressive microenvironment and enhances the anti-tumor efficacy of T cells.
Source: BJC, VCBeat
1.3 Development History: CAR-T Therapy Surges Ahead, Demonstrates Significant Efficacy in Hematologic Malignancies, and Receives Repeated FDA Approvals
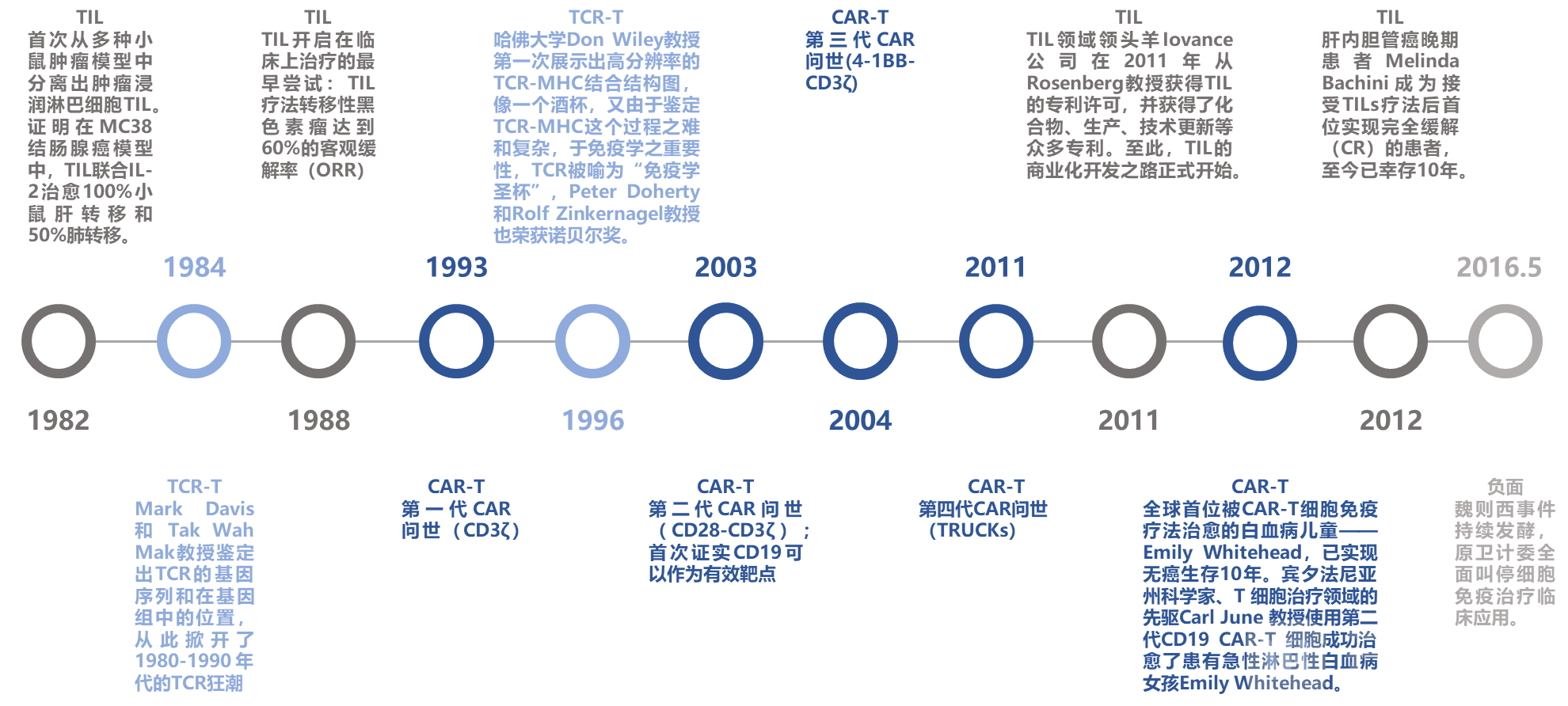
A review of the development history of immune cell therapy reveals that the first-generation CAR was derived from TCR engineering in 1993. Although it started later than TCR and TIL therapies, it has demonstrated significant efficacy in hematologic malignancies, with multiple products approved successively since 2017. In contrast, TCR and TIL therapies primarily target solid tumors, which present greater therapeutic challenges. The following section outlines key milestones and events in the field of immune cell therapy.
In 1982, pioneer Dr. Steven Rosenberg and his colleagues at the National Institutes of Health (NIH) first isolated tumor-infiltrating lymphocytes (TILs) from various murine tumor models. They demonstrated that, in the MC38 colon adenocarcinoma model, TILs combined with IL-2 cured 100% of mice with liver metastases and 50% of those with lung metastases.
In 1984, Mark Davis and Professor Tak Wah Mak identified the gene sequence of the TCR and its location in the genome, thereby ushering in the TCR research boom of the 1980s and 1990s.
In 1988, the earliest clinical attempts at TIL therapy were initiated: TIL therapy for metastatic melanoma achieved a 60% objective response rate (ORR).
1993, the first generation of CAR was introduced (CD3ζ).
In 1996, Professor Don Wiley of Harvard University first revealed the high-resolution structure of the TCR–MHC complex. Resembling a wine glass, and given the difficulty and complexity of characterizing the TCR–MHC interaction as well as its critical importance in immunology, the TCR has been hailed as the “Holy Grail of Immunology.” Professors Peter Doherty and Rolf Zinkernagel were also awarded the Nobel Prize.
In 2003, the second-generation CAR (CD28-CD3ζ) was introduced; it was the first to confirm that CD19 could serve as an effective target.
In 2004, the third-generation CAR (4-1BB-CD3ζ) was introduced.
In 2011, the fourth generation of CARs (TRUCKs) was introduced.
In 2011, Iovance, a leader in the TIL field, obtained a patent license for TILs from Professor Rosenberg and secured numerous patents covering compounds, manufacturing processes, and technological updates. This marked the official commencement of the commercial development of TIL therapy.
In 2012, Emily Whitehead, the first child in the world to be cured of leukemia by CAR-T cell immunotherapy, achieved ten years of cancer-free survival. Professor Carl June, a scientist from Pennsylvania and a pioneer in the field of T-cell therapy, successfully cured Emily Whitehead, a girl with acute lymphoblastic leukemia, using second-generation CD19 CAR-T cells.
In 2012, Melinda Bachini, a patient with advanced intrahepatic cholangiocarcinoma, became the first patient to achieve complete response (CR) after receiving TILs therapy and has survived for 10 years to date.
In May 2016, as the Wei Zexi incident continued to escalate, the former National Health and Family Planning Commission completely halted the clinical application of cellular immunotherapy.
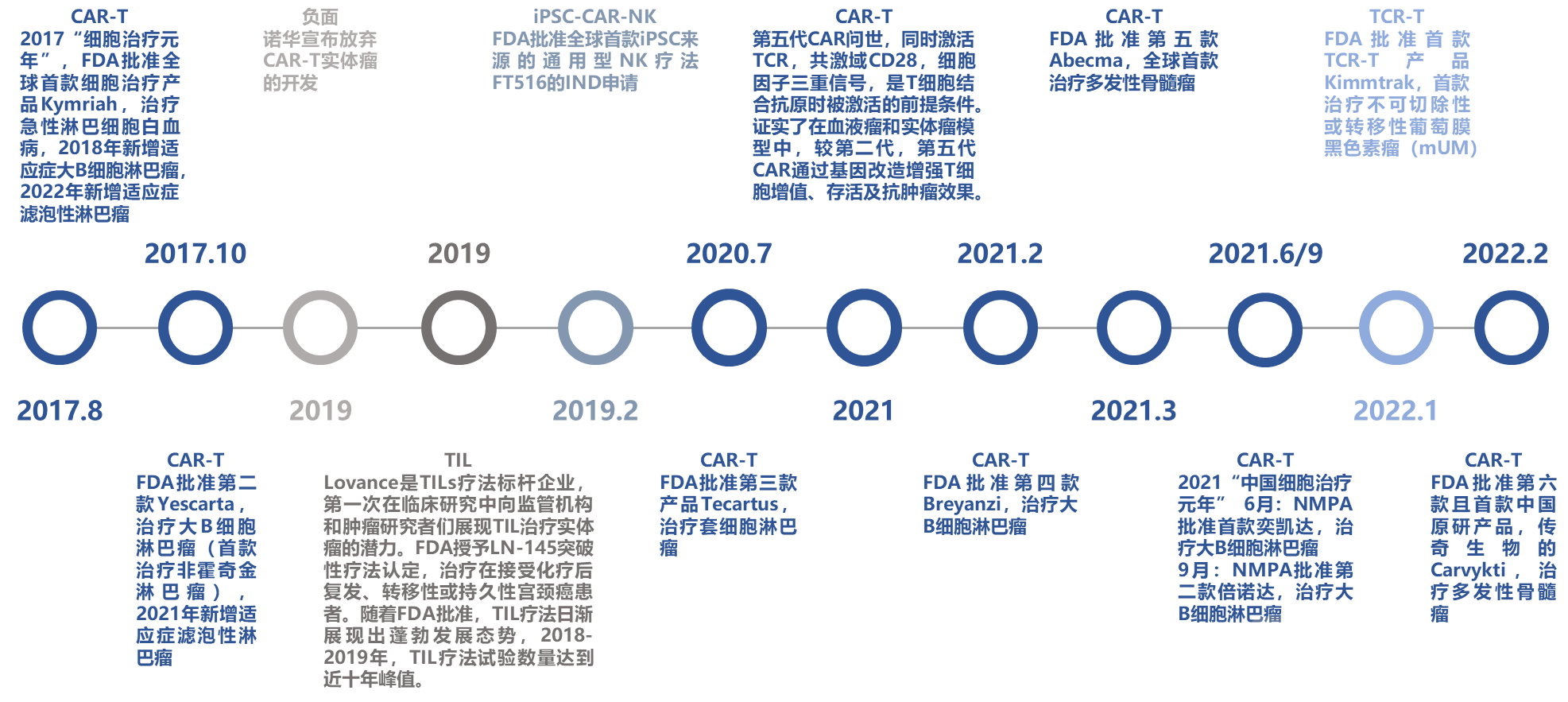
2017: The “Year One” of Cell Therapy.
In August 2017, the FDA approved Kymriah, the world’s first cell therapy product, for the treatment of acute lymphoblastic leukemia; in 2018, its indications were expanded to include large B-cell lymphoma, and in 2022, follicular lymphoma was added as an additional indication.
In October 2017, the FDA approved Yescarta, the second CAR-T therapy (and the first for non-Hodgkin lymphoma), for the treatment of large B-cell lymphoma; in 2021, its indications were expanded to include follicular lymphoma.
In 2019, Novartis announced the discontinuation of its CAR-T therapy development for solid tumors.
In 2019, Lovance Biotechnologies emerged as a benchmark company in the field of tumor-infiltrating lymphocyte (TIL) therapy, being the first to demonstrate the potential of TILs for treating solid tumors to regulatory agencies and oncology researchers in clinical studies. The U.S. Food and Drug Administration (FDA) granted Breakthrough Therapy Designation to LN-145 for the treatment of patients with recurrent, metastatic, or persistent cervical cancer following chemotherapy. With FDA approvals, TIL therapy has increasingly shown robust growth, with the number of TIL therapy trials reaching a decade-high peak during 2018–2019.
In February 2019, the FDA approved the IND application for FT516, the world’s first off-the-shelf NK cell therapy derived from iPSCs.
In July 2020, the FDA approved the third product, Tecartus, for the treatment of mantle cell lymphoma.
In 2021, fifth-generation CARs were introduced. These constructs require triple signaling—simultaneous activation of the TCR, the CD28 co-stimulatory domain, and cytokine signaling—as a prerequisite for T-cell activation upon antigen binding. Studies have confirmed that, compared with second-generation CARs, fifth-generation CARs enhance T-cell proliferation, survival, and anti-tumor efficacy through genetic engineering in both hematologic malignancy and solid tumor models.
In February 2021, the FDA approved Breyanzi, the fourth therapy for large B-cell lymphoma.
In March 2021, the FDA approved Abecma, the fifth such therapy and the world’s first treatment for multiple myeloma.
2021: “Year One of Cell Therapy in China”
In June 2021, the NMPA approved Yikaida, the first CAR-T cell therapy for the treatment of large B-cell lymphoma.
In September 2021, the NMPA approved the second BeiNuoDa for the treatment of large B-cell lymphoma.
In January 2022, the FDA approved Kimmtrak, the first TCR-T therapy, for the treatment of unresectable or metastatic uveal melanoma (mUM).
In February 2022, the FDA approved Carvykti, developed by Legend Biotech, as the sixth therapy and the first originally developed Chinese product for the treatment of multiple myeloma.
Source: Public information, VCBeat.
1.4 Global R&D Momentum in Immune Cell Therapy Remains Strong, with China Ranking Second Worldwide
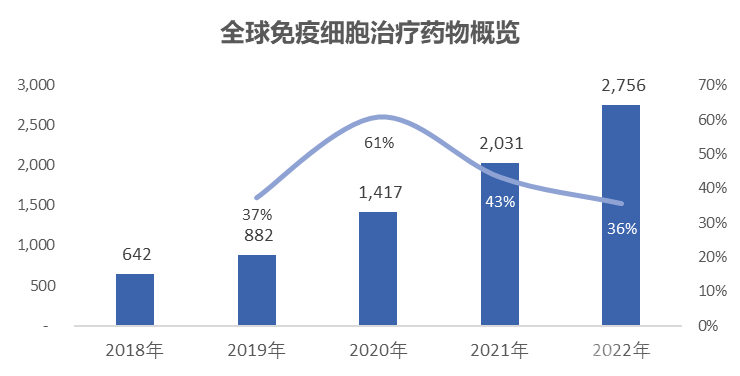
Global R&D Momentum in Immune Cell Therapy Remains Strong
Aggregate Perspective:According to Nature, as of April 15, 2022, there were a total of 2,756 immune cell therapy drugs worldwide, representing a robust 36% growth from the 2,031 active agents recorded in 2021.
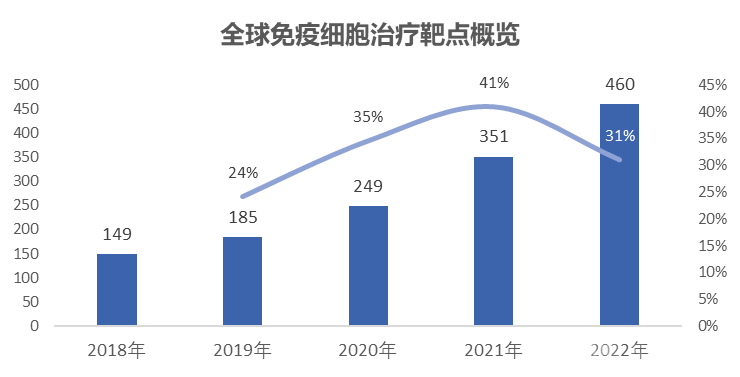
Target Perspective:In 2022, there were a total of 460 targets for immune cell therapy worldwide, representing a year-on-year growth rate of 31%.
Source: Nature, VCBeat
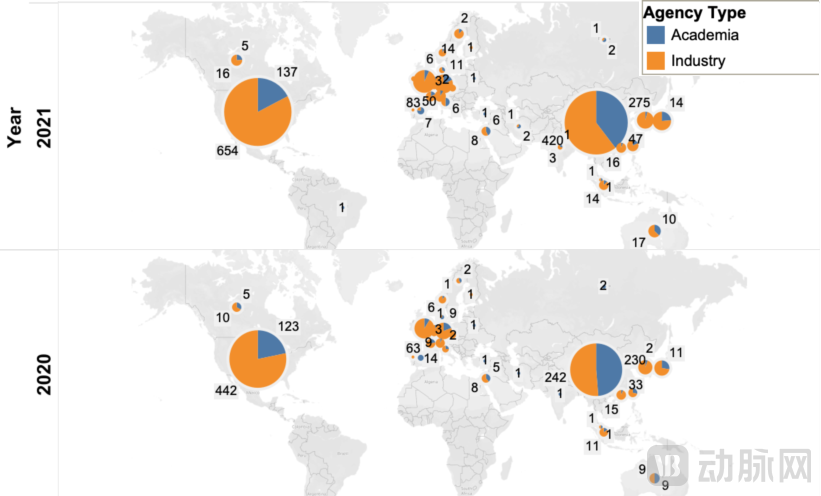
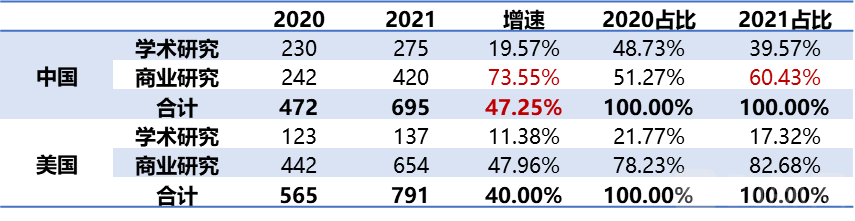
China Ranks Second Globally, Trailing Only the United States
Regional Perspective: China Ranks Second Globally in the Number of R&D Projects, Following Closely Behind the United States.In 2021, China’s total drug pipeline comprised 695 candidates, with a growth rate of 47%, surpassing that of the United States (which had a total of 791 candidates and a growth rate of 40%). From the perspective of R&D attributes, the number of commercial-stage studies in China grew by 74% in 2021, with their proportion rapidly increasing from 51% to 60% (during the same period, the number of commercial-stage studies in the U.S. grew by 48%, accounting for 83%).
Source: Nature, VCBeat.
2.1 Overview of the Four Common Types of Immune Cell Therapy
CAR-T: The Most Mature Immunotherapy Currently Available
■ Therapy Overview
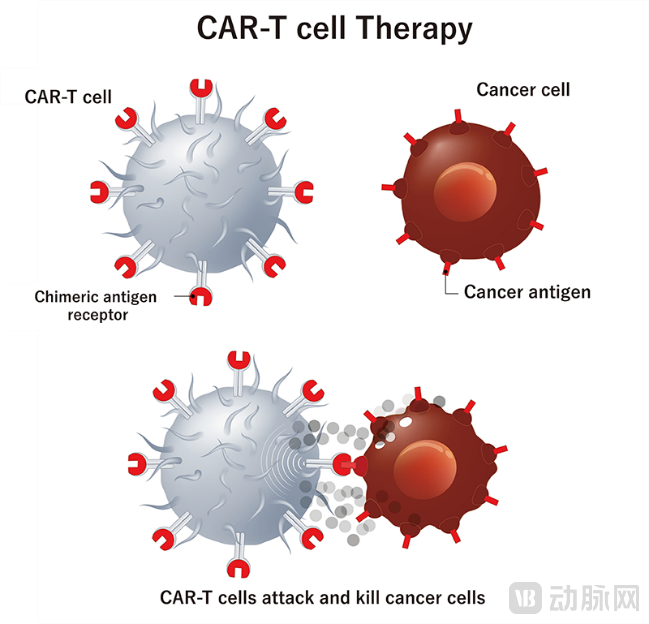
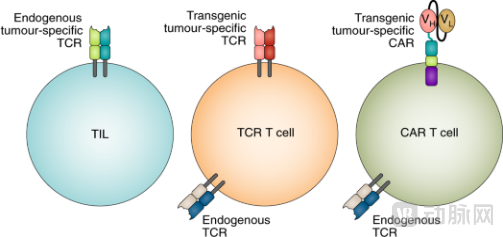
CAR-T (Chimeric Antigen Receptor T Cell): Chimeric Antigen Receptor T Cells.
Through genetic engineering, a chimeric antigen receptor (CAR) gene that artificially confers specific recognition of tumor antigens is introduced into T cells to construct CAR-T cells, which are then infused back into the patient.
The key to CAR-T therapy lies in the design of the CAR receptor molecule. Artificially engineered CAR-T cells are no longer restricted by MHC; T cells can directly bind to specific antigens on the surface of tumor cells and become activated, thereby efficiently killing tumor cells.
■ Tumor-killing mechanism
CAR-T cells are activated through the direct binding of the single-chain variable fragment (scFv) of the chimeric antigen receptor (CAR) to specific antigens on the surface of tumor cells.
(1) Release cytotoxic granules such as perforin and granzyme B, directly mediating the lysis of tumor cells;
(2) Release inflammatory cytokines such as granulocyte-macrophage colony-stimulating factor (GM-CSF) and interferon-gamma (IFN-γ) to recruit endogenous innate immune cells, including macrophages, to kill tumor cells. During this process, memory T cells are also generated, thereby establishing a specific, long-lasting anti-tumor immune response.
■ Indications & Primary Targets
Indications:Primarily hematologic malignancies, including multiple myeloma, acute lymphoblastic leukemia, non-Hodgkin lymphoma (diffuse large B-cell lymphoma, follicular lymphoma, mantle cell lymphoma), Hodgkin lymphoma, and acute myeloid leukemia.
Primary Targets:Tumor cell surface proteins, such as CD19 and BCMA.
Source: Cell and Gene, VCBeat
TCR-T: The First-Generation Immune Cell Therapy, from Which CAR-T Was Derived
■ Therapy Overview
TCR-T (T Cell Receptor-T cell): T cell receptor-engineered T cells.
By using genetic engineering to introduce TCR genes that naturally and specifically bind to tumor antigens into T cells, TCR-T cells are constructed and then infused back into the patient.
TCR-T is the most primitive form of cell therapy and is MHC-restricted, which led to the development of first-generation CAR-T. Since the variable region of TCR can only bind to antigens presented in complex with MHC molecules, whereas the variable region of antibodies can directly bind to antigens, scientists replaced the TCR’s variable region with that of an antibody, thereby constructing first-generation CAR-T cells that are not MHC-restricted and can directly recognize specific antigens.
■ Tumor-Killing Mechanism
TCR-T therapy is based on TCR recognition of a broader range of potential tumor-specific antigens, exhibiting ultra-sensitive detection of low-abundance or mutated intracellular antigens.
(1) Antigen-presenting cells (APCs) phagocytose tumor antigens and degrade them into peptides, which then bind to major histocompatibility complexes (MHCs) and are presented on the APC membrane surface;
(2) When the TCR of a subset of T cells binds to the MHC-peptide complex on the surface of APCs, the T cells are activated through co-stimulatory receptor/ligand interactions (e.g., B7-CD28), thereby specifically killing tumor cells.
■ Indications & Primary Targets
Indications:Primarily solid tumors (accounting for 86%), including melanoma, synovial sarcoma, soft tissue sarcoma, liver cancer, non-small cell lung cancer, ovarian cancer, head and neck squamous cell carcinoma, and epithelial carcinoma; as well as hematologic malignancies, including multiple myeloma and lymphocytic leukemia.
Primary Targets:MHC–antigen complexes formed after antigen-presenting cells (APCs) present tumor cell surface and intracellular antigens, such as NY-ESO-1, MAGE-A4, GPC3, and AFP.
Source: zelluna, VCBeat
CAR-NK: Broad Cell Sources and Promising Commercialization Prospects
■ Therapy Overview
CAR-NK (Chimeric Antigen Receptor-Natural Killer): Chimeric antigen receptor natural killer cells.
By using genetic engineering, artificial CAR genes are introduced into NK cells, which are then infused back into the patient's body.
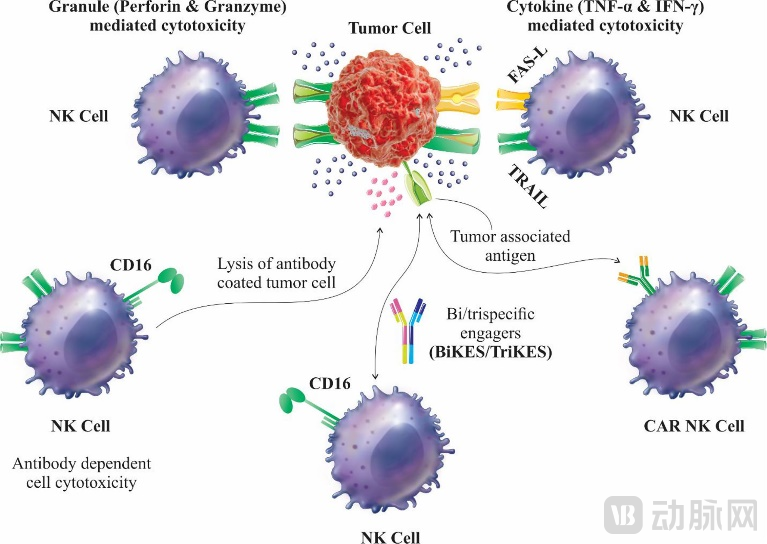
Unlike T cells, NK cells are innate immune cells that do not require prior antigen sensitization. They serve as the body’s first line of defense against tumors and are MHC-unrestricted. As “natural killers,” they rapidly recognize and eliminate mutated tumor cells. NK cells primarily originate from CD34+ lymphocytes in the bone marrow and constitute 10–20% of peripheral blood lymphocytes. The cytotoxic mechanism of NK cells differs from that of T cells; NK cell activity is regulated by the balance between a series of killer-cell immunoglobulin-like receptors (KIRs) and killer activation receptors (KARs) on their surface, rather than depending on any specific antigen on tumor cells.
■ Tumor-Killing Mechanism
(1) Direct cytotoxicity via release of cytoplasmic granules:Cytotoxic granules, such as perforin and granzymes;
(2) Cytokine-mediated cytotoxicity:Release IFN-γ, TNF-α, G-CSF, etc., which interact with receptors on the surface of tumor cells to induce apoptosis;
(3) Activation of ADCC effect:NK cells' Fc receptor CD16 binds to the Fc region of tumor antigen-specific antibodies, triggering antibody-dependent cell-mediated cytotoxicity (ADCC) to kill tumor cells;
(4) Expression of tumor necrosis factor-induced apoptosis:Fas ligand (FasL), binding of tumor necrosis factor-related apoptosis-inducing ligand (TRAIL), etc.
■ Indications & Primary Targets
Indications:Hematologic Malignancies & Solid Tumors, such as acute myeloid leukemia, multiple myeloma, lymphocytic leukemia, gastric cancer, non-small cell lung cancer, ovarian cancer, breast cancer, and pancreatic cancer.
Primary Targets:Tumor cell surface proteins, such as CD19, CD20, and HER2.
Sources: Frontiers, VCBeat
TIL—Unmatched Advantages of Broad-Spectrum Anti-Solid Tumor Therapy
■ Therapy Overview
TIL (Tumor-Infiltrating Lymphocytes): Tumor-infiltrating lymphocytes.
TILs are naturally occurring T cells isolated from patient tumor tissues, which are expanded ex vivo and then reinfused into the patient.
TILs possess the ability to recognize tumor-specific antigens (with a tumor recognition rate exceeding 60%), penetrate deep into tumor tissue, and kill tumor cells, representing a specific anti-tumor immune response of the body. Unlike genetically engineered cell therapies, TILs are not clones of individual T or NK cells; rather, they comprise T cells targeting multiple tumor-specific antigens and are typically composed of effector memory T (Tem) cells.
■ Tumor-killing mechanism
Under dual stimulation signals from TCR and CD28, T cells differentiate into effector T cells, which directly kill tumor cells or secrete factors such as interferons to mediate tumor cell killing.
(1) Release of cytoplasmic granules: perforin, granzymes, etc. Perforin forms polymeric pores on the surface of tumor cells, inducing tumor cell lysis or apoptosis through osmotic changes or in synergy with granzymes.
(2) Expression of tumor necrosis factor-induced apoptosis: Fas on the surface of T cells binds to FasL on the surface of tumor cells.
■ Indications & Primary Targets
Indications:A wide range of solid tumors (20+ types), predominantly including melanoma (>50%), non-small cell lung cancer, ovarian cancer, and head and neck cancer, as well as cervical cancer, breast cancer, colorectal cancer, liver cancer, pancreatic cancer, cholangiocarcinoma, fallopian tube cancer, nasopharyngeal carcinoma, and pleural mesothelioma.
Primary Targets:No specific target requirements; it can simultaneously elicit anti-tumor effects against multiple targets.
Source: Nature Nanotechnology, public information, VCBeat
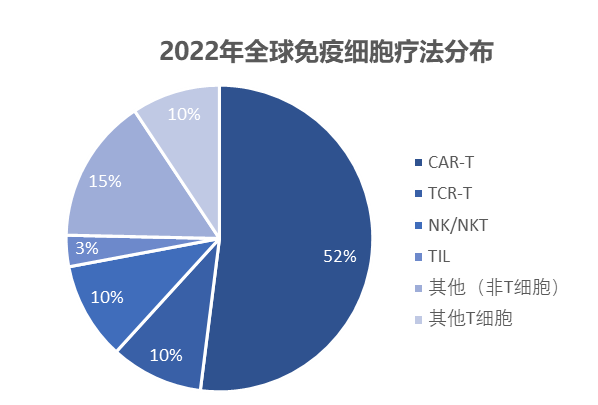
2.2 CAR-T Captures Half the Market, NK Shows Sustained High Growth, and TCR-T and TIL Therapies Slow Down
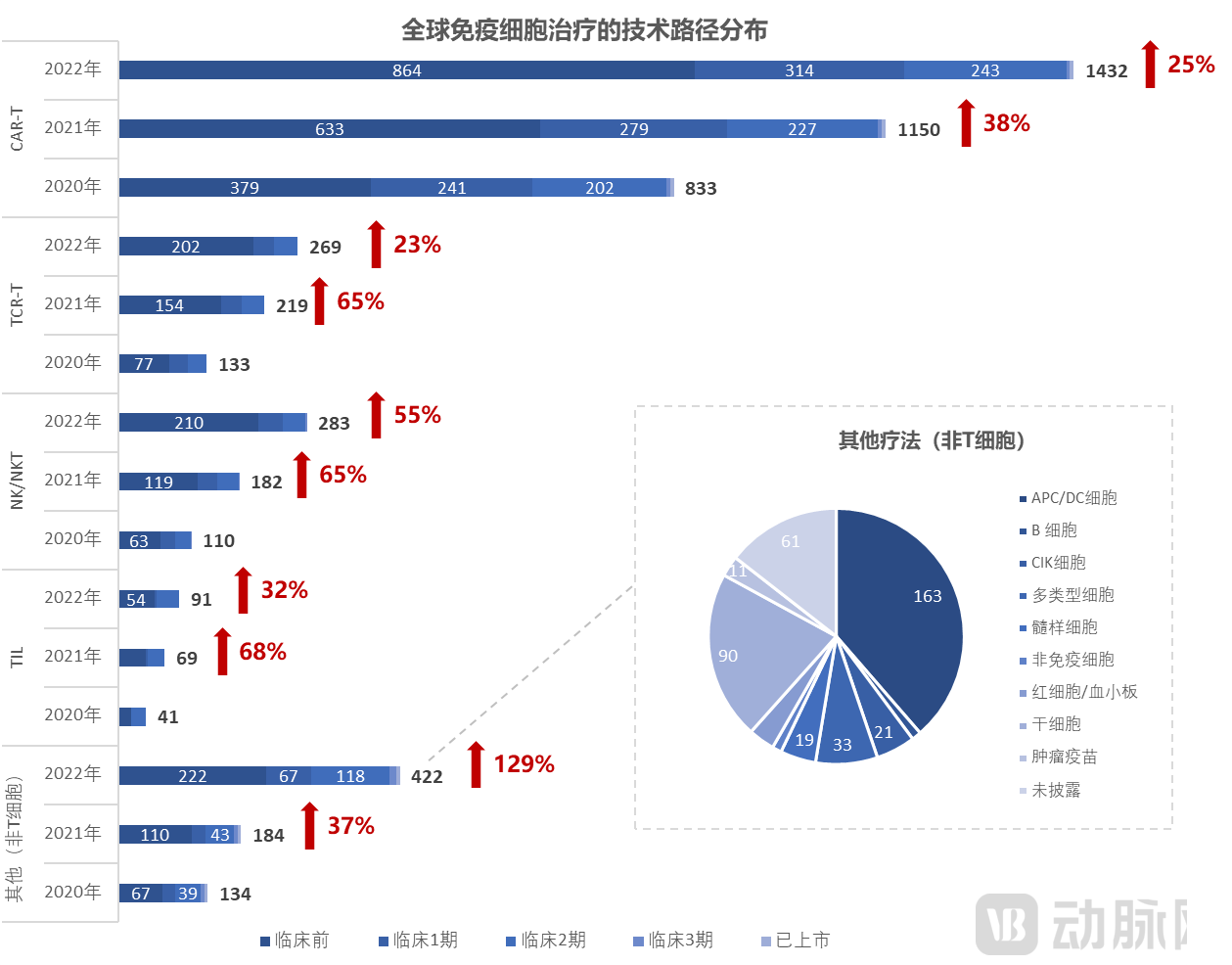
Technical Pathway Perspective: CAR-T Commands Half the Market, While NK Cells Show Sustained High Growth.As of April 15, 2022, there were 2,756 global immune cell therapy drugs (+36%), among which CAR-T cell therapies accounted for 1,432 types (52%), with a growth rate of 25%, slowing down from 38% in the same period last year; NK cell therapies numbered 283 types, maintaining a high growth rate of 55% (compared to +65% in the same period last year). Additionally, other therapies distinct from T cells (such as APC/DC cells) experienced explosive growth of 129% in 2022 (compared to +37% in the same period last year).TCR-T and TIL Growth Slows.There are 269 TCR-T cell therapies, with a growth rate of 23%, representing a significant slowdown from the 65% year-on-year growth in the previous period; there are 91 TIL cell therapies, with a growth rate of 32%, also marking a substantial deceleration from the 68% year-on-year growth recorded previously.
R&D Progress Perspective: Most of the pipeline is still in the preclinical stage.The proportions of preclinical studies for CAR-T, TCR-T, NK, and TIL therapies are 60%, 75%, 74%, and 59%, respectively. The proportion of CAR-T, TCR-T, and NK therapies in Phase I/II clinical trials is approximately 10–20%, while TIL therapies account for 36% in Phase II clinical trials.
Source: Nature, VCBeat
2.3 Autologous Manufacturing and High Pricing of Approved CAR-T Products Hinder Patient Accessibility, with Indications Concentrated in Hematologic Malignancies
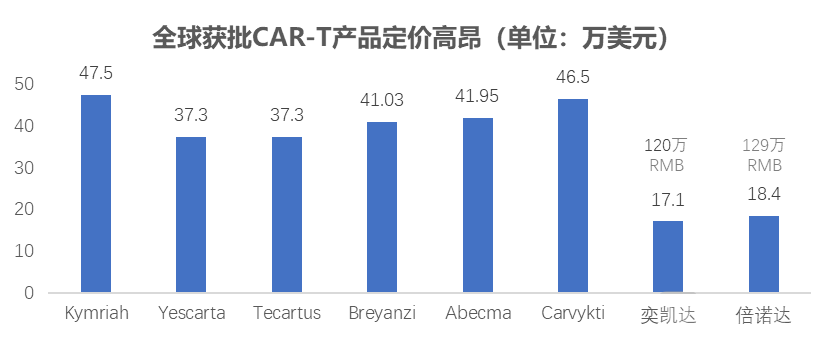
All globally approved indications for CAR-T therapy are hematologic malignancies, and the use of autologous patient-derived cells results in high end-user pricing.
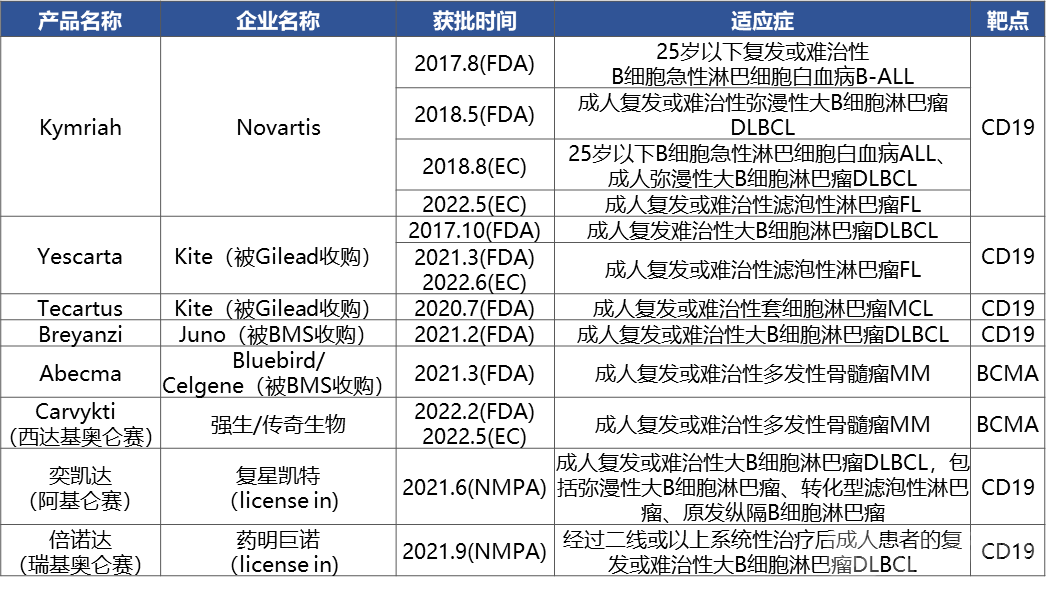
The FDA approved the market launch of six products, and the NMPA approved the license-in of two products.In August 2017, the FDA approved Novartis’s Kymriah, the world’s first CAR-T therapy, which has subsequently received approval for three indications. Notably, Legend Biotech’s independently developed Carvykti (ciltacabtagene autoleucel) was approved by the FDA in February 2022 and by the European Commission in May 2022 for the treatment of adult patients with relapsed or refractory multiple myeloma.
Approved indications are concentrated in hematologic malignancies, with targets clustered around CD19/BCMA:Including adult relapsed or refractory diffuse large B-cell lymphoma (DLBCL), relapsed or refractory B-cell acute lymphoblastic leukemia (B-ALL), adult relapsed or refractory multiple myeloma (MM), adult relapsed or refractory follicular lymphoma (FL), and adult relapsed or refractory mantle cell lymphoma (MCL).
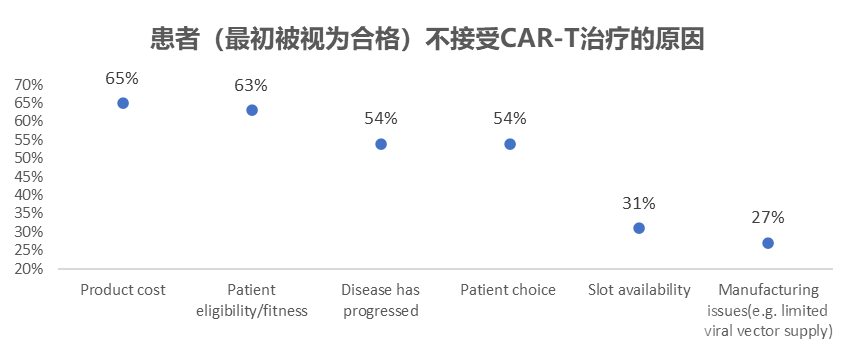
All approved products are autologous CAR-T therapies; high end-user pricing hinders patient accessibility:Nature Real-World Study: An Investigation into the Reasons Why Patients Initially Deemed Eligible Ultimately Did Not Receive Treatment. Results: Cost was the primary barrier to patients receiving cell therapy (65%), followed by patient suitability (63%) and disease progression (54%). Patient wait times and insufficient supply of viral vectors were also significant factors.
Sources: Public information, Nature, VCBeat.
2.4 Breakthrough Strategy 1—Off-the-Shelf General-Purpose Products Offer Greater Commercial Potential
Cell Source Perspective: Autologous Sources Remain Mainstream, While Off-the-Shelf Sources Are Rapidly Catching Up.As of April 15, 2022, there were 2,756 immune cell therapy drugs globally. Among the disclosed drugs with specified cell sources, 1,019 were autologous (+24%), while only 531 were off-the-shelf (allogeneic) (+33%). The ratio of autologous to off-the-shelf therapies decreased from nearly 2.5:1 in 2020 to less than 2:1 in 2022. However, from a commercialization perspective, autologous cell therapy resembles more of a “service,” with manufacturing costs and patient accessibility remaining persistent pain points. In contrast, off-the-shelf cell therapy is more akin to a traditional “drug,” offering prospects for scalable application. Therefore, the current distribution of the development pipeline warrants further optimization.
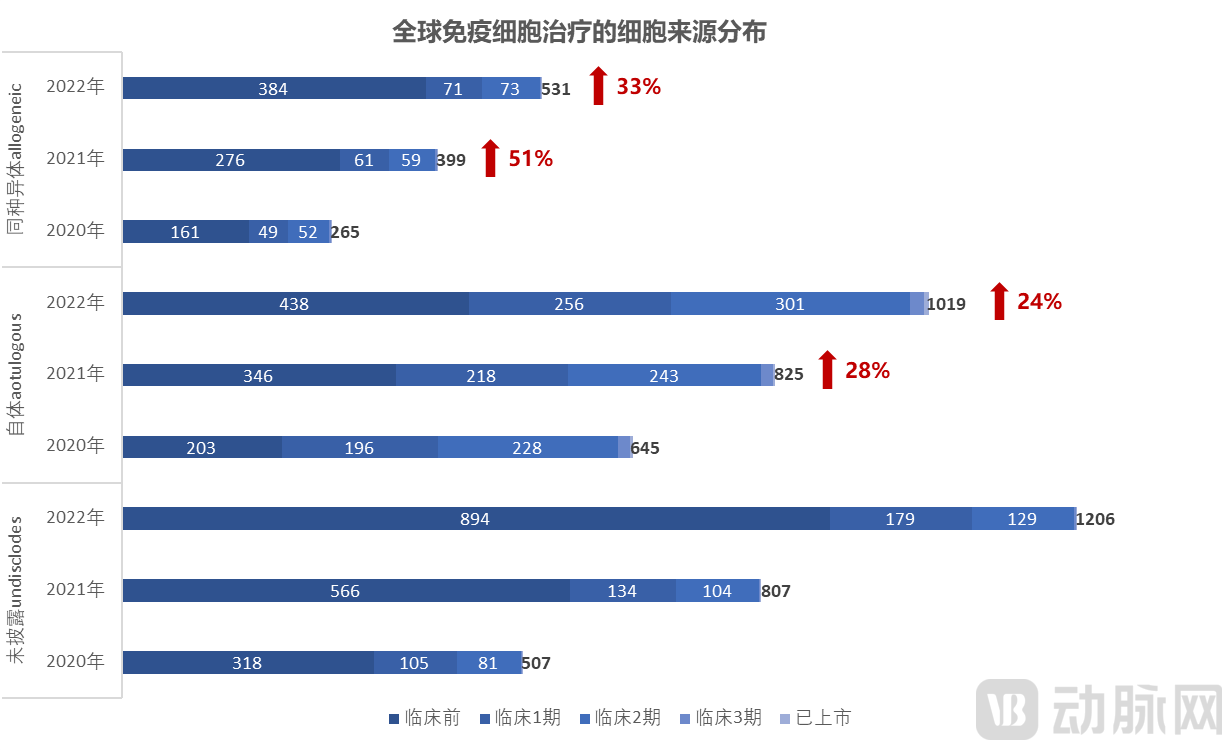
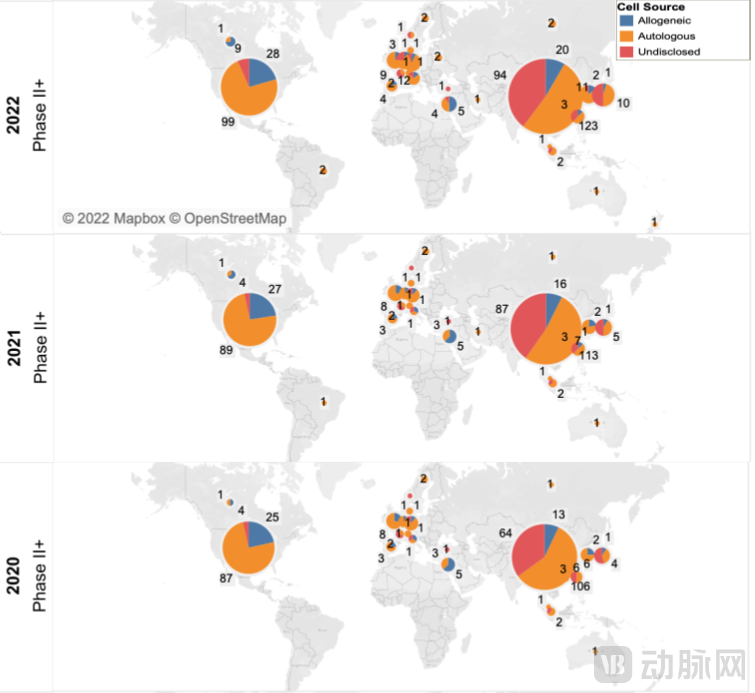
Source: Nature, VCBeat
2.5 Breakthrough Strategy 2—Targeting Solid Tumors, Which Account for 90% of the Market, by Identifying Differentiated Targets
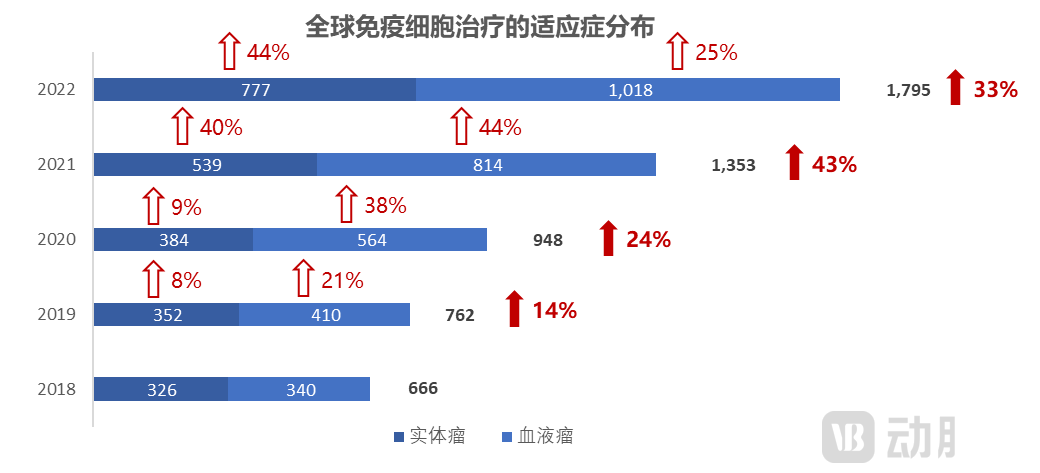
Indication Perspective:Over 50% are focused on hematologic malignancies, with the number of solid tumor pipeline candidates growing rapidly in the past two years.In 2022, the number of pipeline candidates for solid tumors and hematologic malignancies increased by 44% and 25%, respectively. Although the solid tumor pipeline has maintained a growth rate of over 40% in the past two years and accounts for 43% of the total, solid tumors remain a key therapeutic focus given that they represent 90% of market demand.
Target Perspective: Still Congested.Hematologic Malignancies: CD19, BCMA, and CD22 remain the top targets. Several emerging targets are experiencing rapid growth, including GPRC5D (+200%), CLEC12A (+114%), and CD7 (+78%). Solid Tumors: TAAs, HER2, and MSLN remain the most common targets, with TAAs showing a 220% growth rate. Other rapidly growing targets include CLDN18 (+400%), CD276 (+160%), KRAS (+125%), and CD22 (+100%).
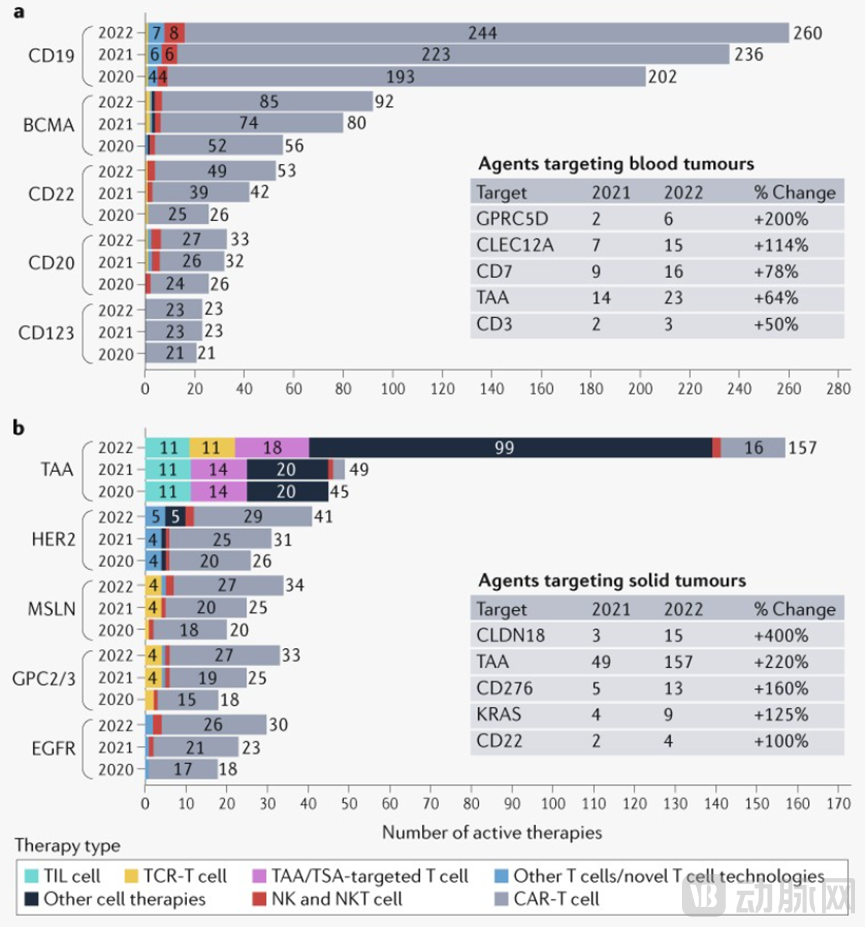
Source: Nature, VCBeat
3.1 CAR-NK Combines Safety and Efficacy Advantages, with Broad Commercial Prospects for iPSC-Derived NK Cells
Hematologic Malignancies: Autologous CAR-TIts efficacy has been validated, with the FDA approving six products.
Solid Tumor Field: TILDerived from the patient’s own tumor tissue, it can theoretically target all cancer types, offering unparalleled advantages in terms of broad-spectrum anticancer efficacy; additionally,TCR-TIts advantages lie in the highly sensitive recognition of intracellular antigens (accounting for 90%) and strong penetration into the interior of solid tumors;CAR-NKThe multi-mechanistic synergistic tumor-killing advantage is significant. It not only identifies tumor antigen-positive cancer cells through CAR-dependent pathways, but also leverages the innate immune capabilities of NK cells as natural killer cells, particularly by inducing antibody-dependent cell-mediated cytotoxicity (ADCC) to achieve tumor eradication.
Commercialization Perspective: CAR-NKmost advantageous, as NK cells are widely available from diverse sources and exhibit homogeneity and stability, making them suitable for large-scale commercial production; additionally,UCAR-TIt also offers the advantage of being ready-to-use, but its cost reduction is not as significant as that of NK.
Source: Public information, compiled by VCBeat.
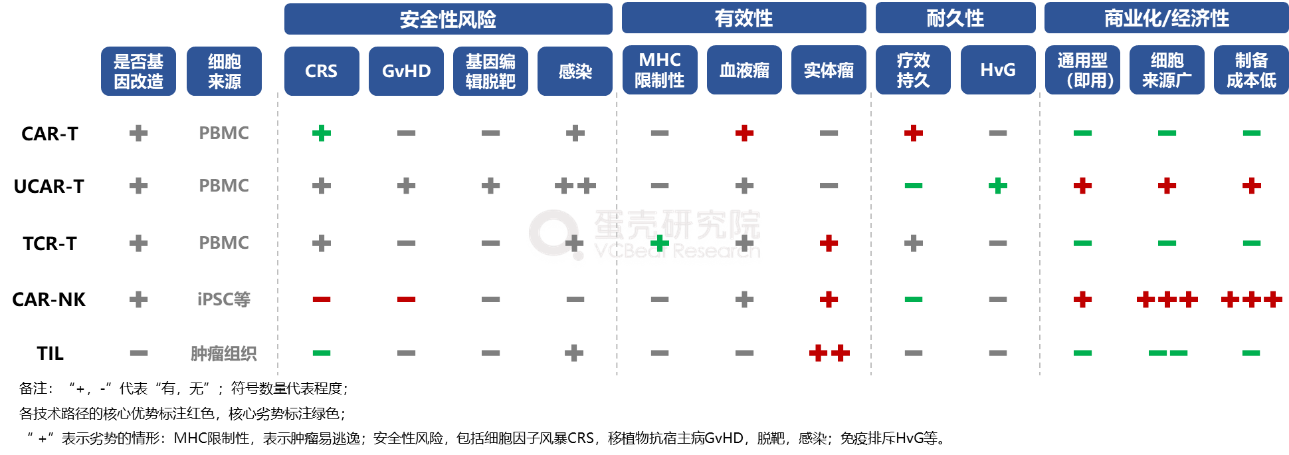
3.2 Diverse Technological Approaches Demonstrate Their Unique Strengths, with CAR-NK Emerging as the Ultimate Path
CAR-T: Strong Efficacy in Hematologic Malignancies, but Dim Commercialization Prospects
■ Advantages
[Efficacy] Demonstrates potent cytotoxic activity against hematologic malignancies:Based on the target antigen, the CAR receptor structure is rationally designed and optimized, enabling CAR-T cells to be activated immediately upon binding to the target molecule. This activation is independent of MHC restriction and co-stimulatory molecules, thereby exerting anti-tumor effects.
【Durability】 Long-lasting therapeutic effect:After CAR-T cells are infused into the patient, they proliferate and become activated, persisting long-term in the body to deliver durable therapeutic effects. A single infusion of CAR-T cells can sustain efficacy for several years, eliminating the need for repeated administrations of antibody-based therapies or chemotherapy.
■ Weaknesses
[Safety] Cytokine Release Syndrome (CRS), Neurotoxicity:leading to serious adverse events such as cerebral edema.
【Commercialization】Autologous products involve non-standardized manufacturing, high costs, and long production cycles, resulting in poor patient accessibility:Listed products cost $400,000–$500,000 and require approximately three weeks for preparation; however, patients with advanced-stage disease often “cannot afford to wait” or struggle to obtain T cells of sufficient quality and quantity, leading to manufacturing failure.
【Efficacy】Suboptimal efficacy in solid tumors:Due to their excessively high affinity, CAR-T cells tend to be retained outside solid tumors in patients and struggle to penetrate into the tumor interior.
UCAR-T—Significantly Reduced Costs; Compromised Efficacy
■ Advantages
【Commercialization】Universal, standardized manufacturing, low cost, ready-to-use, and broad patient accessibility:T cells derived from healthy donors are of high quality, allowing a single manufacturing run to yield over one hundred patient doses. The cost is significantly reduced to one-tenth that of autologous therapies. GMP-standardized processes ensure quality control of all parameters, resulting in a stable product. Patients can receive immediate infusion without waiting, which is particularly significant for those with advanced-stage disease whose T cells cannot be expanded.
■ Weaknesses
【Durability】Therapeutic effects are not long-lasting; immune rejection (HvG):Impact on CAR-T Expansion: Many Leading Pipelines Fail to Surpass the Six-Month Milestone.
[Safety](1) Cytokine Release Syndrome (CRS).(2) Graft-versus-host disease (GvHD):Poses a risk of organ damage.(3) Off-target effects of gene editing:Knockout of TCR/HLA, etc., in allogeneic CAR-T cells.(4) Repeated catheterization increases the risk of infection:More reliant on lymphodepleting chemotherapy than autologous CAR-T.
TCR-T—Broad Intracellular Antigen Recognition; However, Not Suitable for Universal Application
■ Advantages
【Efficacy】(1) Broad recognition of solid tumor antigens:Recognizes intracellular antigens, which account for 90% of all antigens (whereas CAR-T cells only recognize surface antigens).(2) High sensitivity:It can identify a broader range of low-abundance or variant intracellular antigens with high sensitivity (CAR-T cells exhibit much lower antigen sensitivity, requiring 300–400 surface antigens).(3) Strong permeability:
【Durability】Long-lasting efficacy:TCRs are naturally derived and less likely to induce host-versus-graft (HvG) immune rejection. Because TCR-T therapy introduces TCR structural sequences that are entirely derived from natural human selection, the body’s rejection response is weaker compared with CAR-T therapy, which introduces artificially engineered CAR genes.
■ Weaknesses
[Commercialization] Autologous type, with high preparation costs:Because TCR-T therapy is MHC-dependent (the targeted killing of tumor cells by TCR-T requires MHC molecules), and HLA specificity in the population is highly diverse, it is not possible to develop universal TCR-T therapies analogous to CAR-T; instead, TCR-T can only be used in patients with specific HLA phenotypes.
【Efficacy】MHC restriction; tumors are prone to immune escape:Because TCR-T cell activation relies on MHC class I molecules to present tumor antigens to the TCR and requires co-stimulatory signals, the activation process of TCR-T cells is more challenging than that of CAR-T cells. Meanwhile, tumor cells can evade TCR-T cell immunotherapy by downregulating MHC class I molecules, leading to suboptimal therapeutic efficacy.
CAR-NK: Best Safety Profile, Ultra-Low Cost; Repeated Infusions Overcome Durability Limitations
■ Advantages
[Safety] (1) No cases of cytokine release syndrome (CRS) or neurotoxicity have been reported to date; no graft-versus-host disease (GvHD) was observed in allogeneic settings:CAR-NK cells do not secrete pro-inflammatory cytokines such as IL-1 and IL-6. Furthermore, NK cells have a short in vivo lifespan and cannot penetrate the blood-brain barrier. Consequently, they are less likely than CAR-T cells to cause damage to normal tissues due to prolonged activation and persistence in the body, thereby reducing the risk of long-term toxic side effects. Since graft-versus-host disease (GvHD) associated with UCAR-T is mediated by T-cell HLA mismatches, NK cells, which lack this mechanism, do not pose such a risk.(2) NK cells naturally possess anti-infective capabilities:CAR-NK cells also provide defense against pathogens such as bacteria, fungi, and other viruses, helping to prevent and treat concurrent and secondary infections.
[Efficacy] (1) Significant advantages in synergistic multi-mechanism killing of solid tumors:Not only does it identify tumor antigen-positive cancer cells through CAR-dependent pathways; meanwhile, NK cells themselves possess innate immune capabilities, enabling them to recognize cancer cells expressing ligands for NK cell receptors, release cytoplasmic granules and cytokines, and activate the expression of apoptosis receptors on the surface of tumor cells. Key emphasis: By triggering antibody-dependent cellular cytotoxicity (ADCC) and combining with antibody drugs, this approach can enhance the mechanism by which antibody drugs induce NK cell-mediated tumor killing via ADCC.(2) MHC-unrestricted tumor cell killing:NK cells express lower levels of immune checkpoint molecules (such as PD-1) than CAR-T cells, resulting in weaker suppression by the immunosuppressive microenvironment. Even when tumor cells downregulate the target antigens of CARs, NK cells can still kill tumor cells, offering greater advantages in the treatment of solid tumors.
[Commercialization] Universal type, with extensive cell sources and extremely low preparation costs:NK cells are derived from a wide range of sources and are available in large quantities (particularly those derived from iPSCs; if the estimated cost is reduced to the level of antibody drugs, they would have a two-order-of-magnitude advantage over UCAR-T). Their isolation and expansion in vitro are relatively simple, with consistent quality and high efficiency, making them suitable for large-scale commercial production. They do not require extraction from patients themselves, enabling timely access to treatment.
■ Weaknesses
【Durability】Short in vivo survival time:In the absence of IL-2 and IL-15, CAR-NK cells exhibit limited in vivo persistence. Furthermore, NK cells are inherently sensitive to freeze-thaw processes, and their premature death results in suboptimal therapeutic efficacy. However, repeated infusions can overcome the limitation of poor durability, while the sufficiently low cost enables patients to afford multiple infusion treatments.
TIL—Broad-spectrum activity against solid tumors; but sample preparation is cumbersome.
■ Advantages
[Safety] Derived from the patient's own tumor tissue, with virtually no toxic side effects:Tumor-infiltrating lymphocytes (TILs) are innate T cells that undergo in vivo selection. TILs specifically recognize tumor antigens without recognizing normal tissues, and they are non-immunogenic (i.e., not recognized by the immune system as foreign antigens). They exhibit minimal adverse effects (with high-dose interleukin-2 [IL-2] toxicity being the sole concern), virtually no off-target toxicity (as their targeting capability is derived from natural host training rather than artificial engineering), and do not induce cytokine release syndrome (CRS).
[Efficacy] (1) Unparalleled advantages of broad-spectrum anti-solid tumor activity:TILs are derived from patients’ own tumor tissues and can specifically recognize a variety of tumor antigens, theoretically enabling their application across all cancer types. Clinical trials have been conducted worldwide for multiple solid tumors, including metastatic melanoma, nasopharyngeal carcinoma, head and neck squamous cell carcinoma, cholangiocarcinoma, recurrent/refractory ovarian cancer, osteosarcoma, cervical cancer, ovarian cancer, non-small cell lung cancer, glioma, and pleural mesothelioma, demonstrating a broader scope than TCR-T and CAR-NK therapies.(2) Natural tumor recognition and infiltration capabilities:TILs are isolated from tumor-infiltrating cells that have undergone complete sensitization and lymph node activation. They exhibit high expression of homing receptors and superior cell motility, enabling more efficient recruitment by tumor-associated chemokines and subsequent tumor infiltration upon reinfusion. Unlike CAR-T/TCR-T cells derived from peripheral blood, TILs demonstrate a tumor recognition rate exceeding 60%.(3) Natural multi-targeting, no need for artificial discovery:Overcoming the Challenge of Tumor Heterogeneity. Tumors are composed of cancer cells with various genetic mutations. Therapies such as CAR-T, which target only a specific mutation type, may completely eliminate that particular subset of cancer cells but often fail to prevent the growth of other mutant clones. In contrast, Tumor-Infiltrating Lymphocytes (TILs) naturally reside within the tumor microenvironment and have been exposed to a broad range of tumor-specific antigens. Rather than consisting of a single T-cell clone, TIL therapy comprises a heterogeneous population of T cells capable of recognizing multiple tumor-specific antigens.
■ Weaknesses
[Commercialization] (1) Autologous type: highly customized, high cost, and long cycle.Low success rate of in vitro expansion.(2) Difficulty in obtaining cell sources:Fresh tumor samples are difficult to obtain and are not patient-friendly (requiring surgery), while TILs with strong anti-tumor activity and proliferative capacity are also challenging to acquire (depending on whether there is sufficient T-cell infiltration in the surrounding tumor tissue).
【Durability】Short survival time in the body:TILs are predominantly exhausted T cells, and prolonged in vitro screening, expansion, and culture further exacerbate their exhaustion. Meanwhile, TILs also face suppression from the immune microenvironment within tumor tissues: PD-L1/L2, ligands for PD-1, are expressed in various tumor types and interact with their receptors to establish an immunosuppressive microenvironment, thereby inhibiting effector T cell function and accelerating T cell exhaustion.
The above is an excerpt of the main content of the report. The complete framework of the report is as follows:Scan the QR code and proactively inquire to download the full report for free.

Part I: Efficacy of Immune Cell Therapy as “Living Drugs” Stands Out, with Unabated Global R&D Momentum
1.1 Immune Cell Therapy—“Live Drugs” in Tumor Immunotherapy, with Prominent Efficacy Advantages
1.2 The first generation of CARs overcomes the MHC restriction of TCRs, with each subsequent generation aiming to enhance cellular proliferation and cytotoxicity.
1.3 Development History: CAR-T Overtakes Competitors, Demonstrates Significant Efficacy in Hematologic Malignancies, and Receives Repeated FDA Approvals (2/2)
1.4 Global R&D Momentum in Immune Cell Therapy Remains Strong, with China Ranking Second Worldwide
Part II: Current Status of R&D in Immune Cell Therapy and Strategies for Breakthroughs
2.1 Overview of the Four Common Types of Immune Cell Therapy
2.2 CAR-T Accounts for Half the Market, NK Cells Show Sustained High Growth, and TCR-T and TIL Therapies Experience Slowing Growth
2.3 High Costs of Autologous Preparation and Pricing for Approved CAR-T Products Hinder Patient Accessibility, with Indications Concentrated in Hematologic Malignancies
2.4 Breakthrough Strategy 1: Off-the-Shelf General-Purpose Products Offer Greater Commercial Potential
2.5 Breakthrough Strategy 2: Conquering Solid Tumors, Which Account for 90% of the Market, by Identifying Differentiated Targets
Part III: A Brief Discussion on Development Prospects from the Perspective of Technological Pathways
3.1 CAR-NK Combines Safety and Efficacy Advantages, with Broad Commercial Prospects for iPSC-Derived NK Cells
3.2 Diverse Technical Approaches Demonstrate Their Unique Strengths; CAR-NK May Emerge as the Ultimate Pathway
CAR-T: Strong Efficacy in Hematologic Malignancies, but Dim Commercial Prospects
UCAR-T: Significantly Reduced Costs, but Compromised Efficacy
TCR-T: Broad Recognition of Intracellular Antigens; However, Not Universally Applicable
CAR-NK: Optimal safety, ultra-low cost; repeated infusions to overcome durability limitations
TIL—Broad-spectrum activity against solid tumors; but sample preparation is cumbersome.