Dingke Medical Showcases Combination Therapy of Dissolve® AV and DKutting® for Refractory AVG Stenosis in Case Series by Prof. Hou Yikai’s Team

DK Medtech
Vascular Interventional Balloon Product Developer
Stenosis of autologous or artificial arteriovenous fistula (AVF/AVG) is the most common complication in hemodialysis patients. Percutaneous transluminal angioplasty (PTA) has become the primary method for maintaining dialysis access. However, the blunt and irregular tearing of the intima and part of the media by traditional balloons during PTA can cause excessive damage to the endothelial vessels, leading to intense proliferation of vascular smooth muscle cells and macrophages, which quickly results in restenosis.
In recent years, there have been continuous explorations and clinical studies internationally on the use of drug-coated balloons and other devices for PTA treatment in dialysis access. DK Medtech has developed...Dissolve® AVScored Drug-Coated Balloon, integrating "scoring," "high-pressure," and "drug-coating" three features in one, is the world's first third-generation drug-coated balloon:
Directional Scoring: Uniform and regular tearing of the intima to reduce damage from blunt dissection.
High Burst Pressure: For high-resistance lesions, improving technical success rate.
Paclitaxel Coating: Effectively Inhibits Excessive Proliferation of Smooth Muscle Cells.
DK Medtech Special Release[Professor Hou Yikai's Team:Dissolve®AV Combined with DKutting®For Endovascular Intervention in Refractory AVG Stenosis】Case Presentation: Demonstrating the precise operations of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized intraoperative procedures and technical applications, complication prevention, to perioperative management, etc., the aim is to promote the standardization of diagnosis and treatment for vascular stenosis and occlusive diseases, enhance technical exchange and experience sharing among physicians, with the hope of providing new ideas and methods for future diagnosis and treatment, benefiting more clinical patients.
Patient Information
Basic Information:Male, 68 years old.
Chief Complaint:Elevated venous pressure during hemodialysis for 1 week.
Details of Present Illness:
In August 2016, abnormal kidney function was detected during a physical examination, with a blood creatinine level of 500 umol/l. Diagnosed with CKD Stage 5 (uremia), the patient refused renal replacement therapy and opted for conservative treatment with medication.
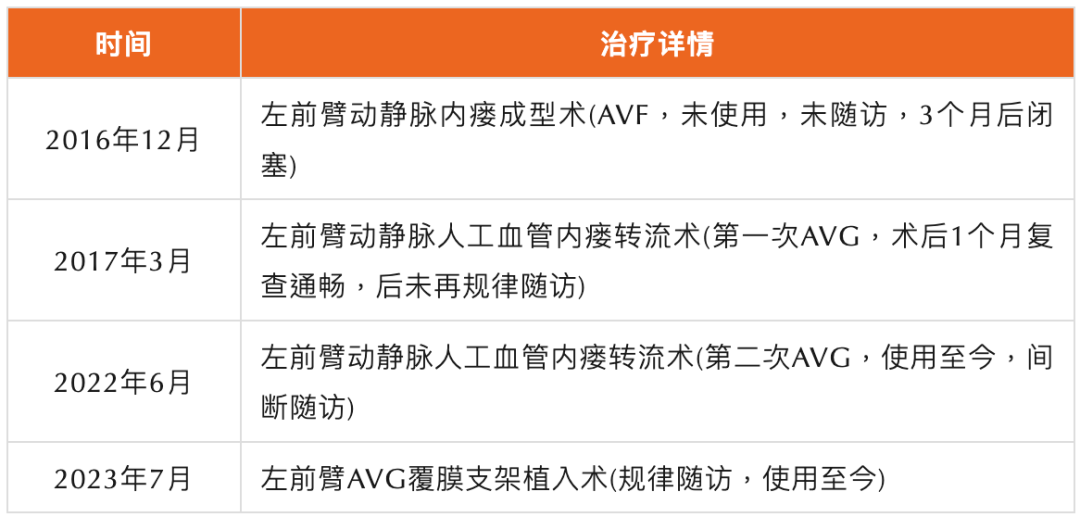
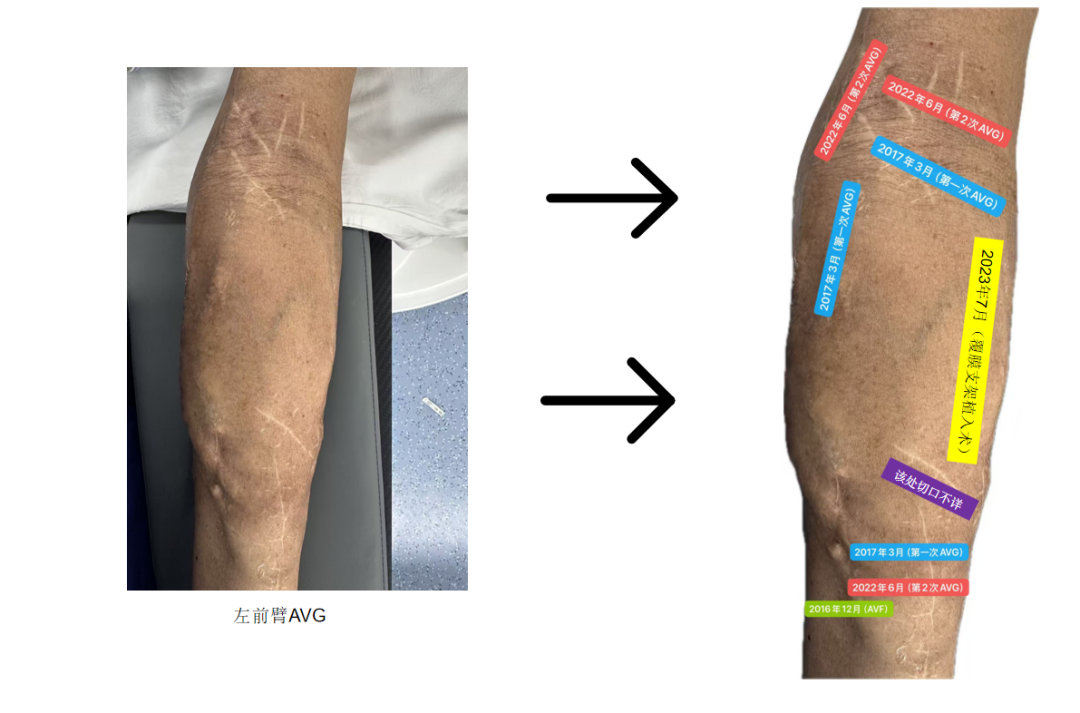
In December 2016, the patient underwent left forearm arteriovenous fistula formation (AVF). Without regular follow-up, the blood flow gradually decreased and became occluded three months post-surgery.
In March 2017, underwent left forearm arteriovenous graft (AVG) bypass surgery. One month post-operation, thrill was palpable upon assessment, but follow-up was irregular thereafter.
In May 2017, a re-examination of renal function showed Scr 778 umol/l, accompanied by complications such as gastrointestinal issues and skin itching, without immediate renal replacement therapy.
On July 1, 2017, hemodialysis treatment was initiated due to cardiovascular complications, performed three times a week, using low-molecular-weight anticoagulants along with erythropoietin and L-carnitine treatment.
In June 2022, right internal jugular vein catheterization was performed for hemodialysis due to AVG occlusion, followed by re-implantation of an artificial arteriovenous graft (AVG) in the left forearm.
In July 2023, due to poor blood flow in the internal fistula, a covered stent was implanted at the AVG arterial puncture site. Regular follow-up was not conducted after the surgery.
On March 16, 2026, the patient presented with elevated venous pressure during hemodialysis accompanied by difficulty in achieving hemostasis at the puncture site.
History of Previous Interventional Treatments
Preoperative Assessment
Ultrasound Examination
Visible forearm artificial vascular fistula stent image, with irregular inner walls of the stent, uneven blood flow, and imaging showing narrowing near the venous anastomosis on the proximal side.
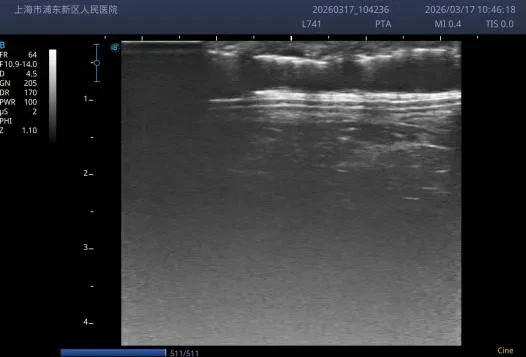

AVG Arterial Segment Stent Image
AVG-Cephalic Vein Stenosis Near the Proximal Anastomosis
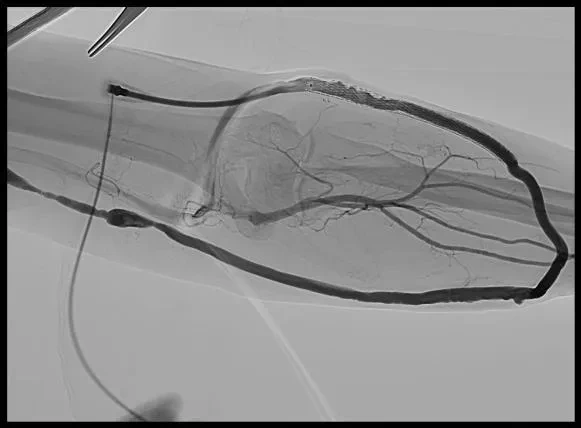
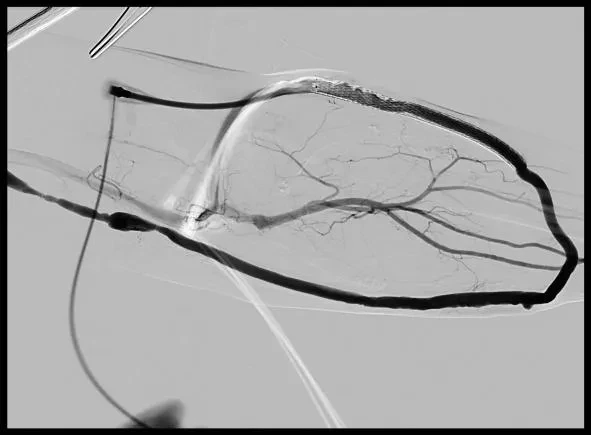
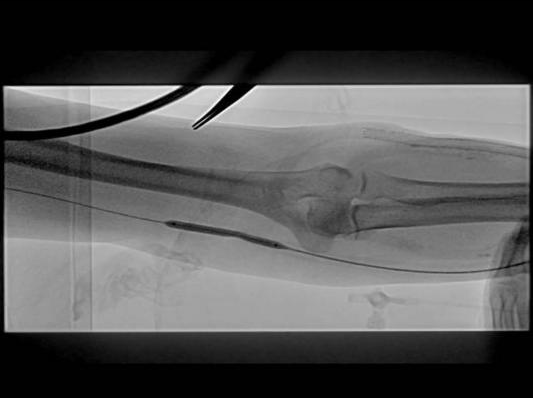
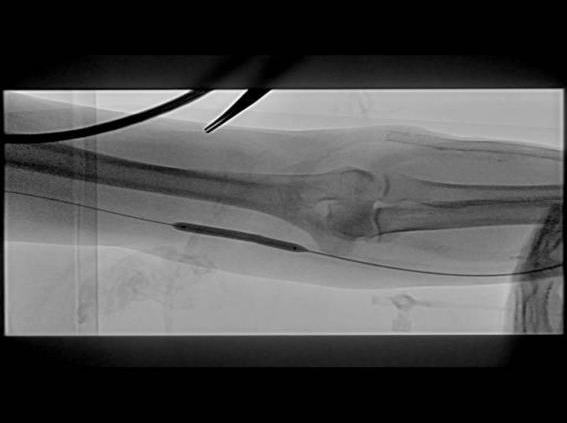
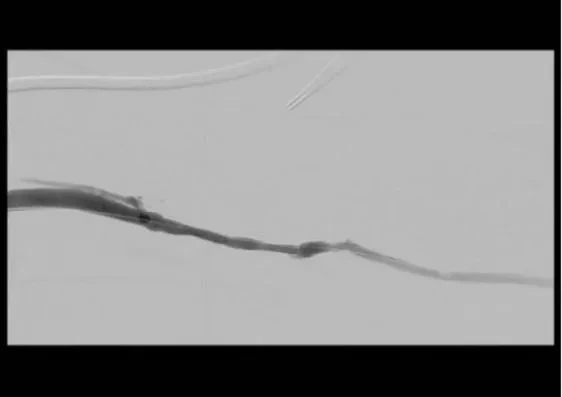
Angiography
Obvious stenosis is visible in the forearm arteriovenous graft, with tortuous vascular pathway and blood flow filling defect in the stenotic area, indicating outflow obstruction.
Fluoroscopic Image Data
Silhouette Image Data
Surgical Procedure
Use DK MedtechDissolve®AV Notch Drug-Coated Balloon(6×60mm) Treat the stenotic segment of the basilic vein near the venous anastomosis (pressure 20ATM for 2 minutes), complete inflation sequentially.Filling, Expansion, and Depressurization Operations.
After two dilations, the stenosis was significantly improved.
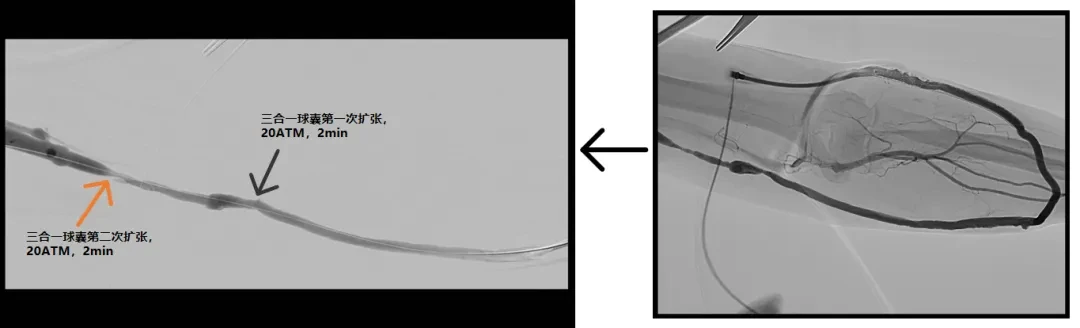
For residual stenosis of the venous anastomosis and the proximal basilic vein, use DKutting by DK Medtech.®A scored balloon (7×40mm) was used for enhanced dilation.


Postoperative Effect Evaluation
Final Angiography:The original stenotic segment is patent with unobstructed blood flow. Ultrasound measurement of brachial artery blood flow is 780 ml/min.
Clinical Significance:Successfully relieved the stenosis, restored normal blood flow of the dialysis access, ensuring the maintenance of hemodialysis.
Case Summary and Reflection
Reasonable Selection of Instruments
The AVG venous anastomosis and the proximal basilic vein predominantly exhibit intimal hyperplasia leading to stenosis, with relatively thinner vessel walls. ThereforeA balloon that can uniformly dilate the blood vessel wall and effectively inhibit intimal hyperplasia is required; frequent surgeries should be avoided to prevent the risk of vascular rupture and bleeding.Disslove®AV integrates high pressure, scoring, and drug coating, dilating the lesion while delivering the drug directly to the media layer for long-term inhibition of intimal hyperplasia.
Inhibition of Intimal Hyperplasia + Minimal Residual Stenosis = Prolonged Patency of Fistula
The intimal hyperplasia of the target lesion in this case was severe, with a high degree of stenosis.,In Use: Disslove®After AV dilation is completed, select the next larger size of DKutting again.®Post-dilation with a scored balloon further reduces residual stenosis, helping patients maximize the patency of their fistula and ensuring smooth dialysis access.。
A single-center randomized controlled trial in Greece included 40 dialysis patients with dysfunctional mature arteriovenous fistulas (AVF) having a single >50% stenosis. Patients were randomly divided into a paclitaxel-coated balloon group (PCB, n=20) and a high-pressure plain balloon group (HPB, n=20) at a 1:1 ratio. There was no statistically significant difference in baseline data between the two groups.All procedures were performed with standard intraluminal techniques without pre-dilation. In the PCB group, if residual stenosis was >30% after the procedure, HPB dilation was performed for 2 minutes. If necessary, a high-pressure balloon 1mm larger in diameter was used for further dilation.In terms of procedural success rates and complications, the HPB group achieved a 100% device success rate, while the PCB group only reached 35%. In 65% of the PCB group cases, post-dilation with HPB was required to achieve a residual stenosis of <30%. Both groups achieved 100% anatomical and clinical success rates, with no minor or major procedure-related complications reported. Regarding long-term outcomes, the PCB group showed significantly better TLR-free survival (median 308 days) and primary patency of dialysis access (median 270 days) compared to the HPB group (both median 161 days), with hazard ratios of 0.478 and 0.479, respectively.PThe values are 0.03 and 0.04, respectively.Confirmed that the use of a drug-coated balloon in combination with a larger-sized high-pressure balloon for post-dilation is complication-free and can significantly improve long-term patency rates.[1]。
References:
[1]Kitrou P M, Spiliopoulos S, Katsanos K, et al. Paclitaxel-Coated versus Plain Balloon Angioplasty for Dysfunctional Arteriovenous Fistulae: One-Year Results of a Prospective Randomized Controlled Trial[J]. Journal of Vascular and Interventional Radiology, 2015, 26(3): 348-354.
Expert Introduction

Professor Yikai Hou
Surgeon of This Case
Department of Nephrology, People's Hospital of Pudong New Area, Shanghai, Associate Chief Physician
Member of the Nephrology and Dialysis Professional Committee of the China Non-Public Medical Institutions Association
Member of the Nephrology Professional Committee of the Medical Association of High-Tech Zone, Suzhou City
Proficient in the clinical diagnosis and treatment of common and frequently-occurring diseases in nephrology, as well as various modes of blood purification treatment and complication management. Skilled in establishing and maintaining various dialysis vascular accesses, such asAVFAngioplasty,TCCCatheterization,AVF/AVGStenosis/ThrombusPTATreatment, Percutaneous Intravenous Catheter Thrombolysis, Open Thrombectomy,DSATreatment of central venous stenosis, etc.
As the project leader, completed two new hospital-level technologies, participated in one municipal scientific research fund project, and co-authored one monograph.
PublishSCIAnd several Chinese core and national journals
Department Introduction
The Department of Nephrology at People's Hospital of Pudong New Area is a key discipline of the Pudong New Area Health Commission, the leading unit of the Hemodialysis Quality Control Group under the Pudong Medical Quality Control Center, a flagship department of integrated traditional Chinese and Western medicine of the Pudong New Area Health Commission, and a member unit of the National Chronic Kidney Disease Network. It has also been awarded the title of "National Model Unit of Women's Civilization." Currently, the department has 40 open beds, 80 hemodialysis machines, and 9 CRRT machines. It has established both hemodialysis and peritoneal dialysis centers, serving more than 480 patients on maintenance dialysis.(330/150), the largest hemodialysis and peritoneal dialysis center in Pudong New Area, where peritoneal dialysis has risen to the top three among district-level hospitals in Shanghai after three years of development. The department has now established a hemodialysis vascular access team, fully implementing hemodialysis vascular access techniques, including autologous arteriovenous fistula formation, arteriovenous graft fistula bypass surgery, balloon angioplasty for arteriovenous fistula stenosis (PTA), balloon angioplasty for graft stenosis, thrombectomy for fistula thrombosis, surgical treatment for steal syndrome, and DSA-guided interventional treatment for swollen hand syndrome, serving a large number of hemodialysis patients around the hospitals in Pudong New Area.

