The Next $100 Billion Market: Where Are the Real Investment Opportunities in Brain-Computer Interfaces?
At the opening ceremony of the 2014 FIFA World Cup in Brazil, witnessed by over one billion viewers worldwide, a paraplegic young man wearing an Iron Man-style bodysuit used a “mechanical armor” exoskeleton device to control his “legs” via brainwaves and kick the first ball. This moment was undoubtedly astonishing and deeply moving.
This groundbreaking milestone also holds epoch-making significance for the scientific and technological community. It marks the first case in the history of science and technology where a mechanical exoskeleton device was controlled by the brain activity of a paralyzed patient, representing a historic breakthrough in human-brain-to-machine interaction. In recent years, with the continuous advancement of neuroscience and related technologies, models of human-computer interaction have been constantly evolving and changing. As the most cutting-edge field in neuroscience, brain-computer interfaces (BCIs) have emerged as the latest generation of human-computer interaction, garnering significant attention and strategic support from countries around the world.
Brain-Computer InterfacesIn simple terms, brain-computer interfaces (BCIs) establish a direct connection between the human brain and external devices (such as computers or other external apparatuses) to enable direct communication. Building on past research and exploration, BCI technology has moved beyond its early days of scientific fantasy and is now entering a phase of rapid technological advancement, drawing significant attention from industry professionals and capital markets.
So, what exactly is brain-computer interface (BCI) technology? What is the current state of the market? And what are its application scenarios and investment opportunities?
Recently, China Renaissance released an industry research and analysis report on brain-computer interfaces (BCI). The healthcare technology team of China Renaissance New Economy Fund analyzed the fundamental concepts of BCI, as well as its implementation and clinical applications. Furthermore, the team conducted an in-depth discussion on market size, the industrial chain, and investment logic. This article consolidates these insights, with the aim of providing readers with valuable inspiration and takeaways.
1. Definition and Development Trends of Brain-Computer Interfaces
Brain-Computer Interface (BCI): A system that enables direct communication between the human brain and the external environment (computers or other external devices) without relying on the brain’s normal output pathways (i.e., peripheral nerves and muscle tissues).
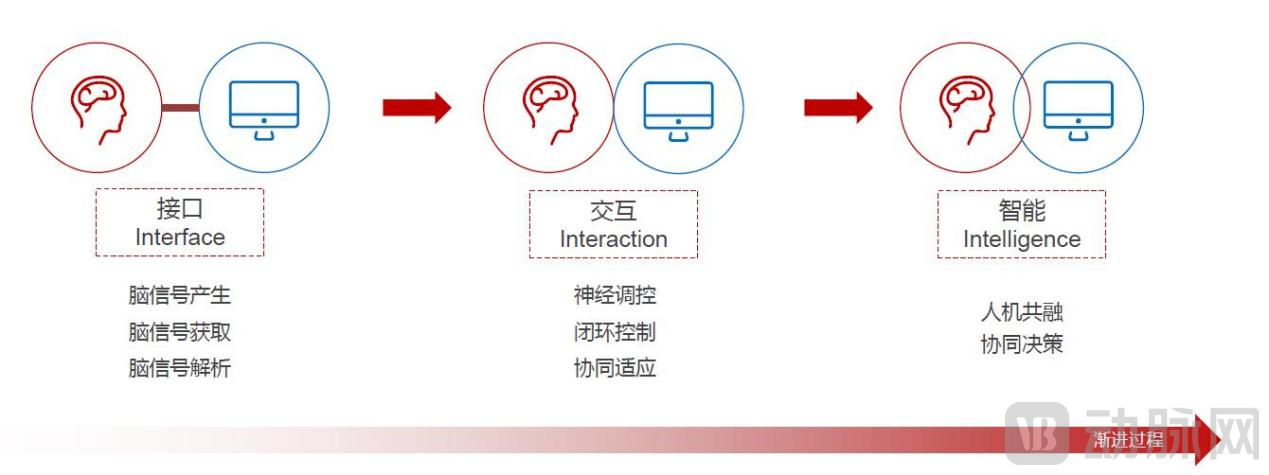
Development Trends: Gradually evolving from simple unidirectional brain-computer interfaces (generation, acquisition, and decoding of brain signals) to human-computer interaction, ultimately achieving a highly intelligent state characterized by human-machine integration and collaborative decision-making.
Source: China Renaissance Analysis
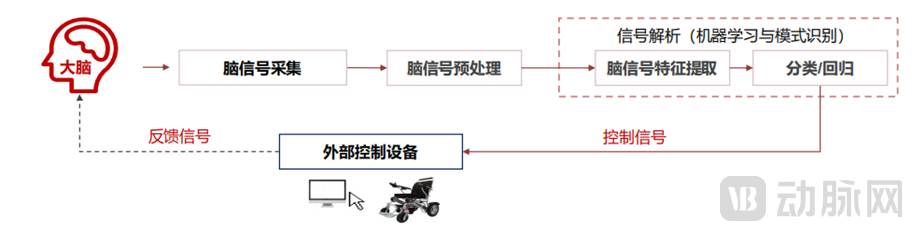
Brain-computer interface (BCI) systems consist of seven major components: the brain, brain signal acquisition, brain signal preprocessing, signal decoding, control interface, external control devices, and neural feedback, forming a closed loop. External devices can include computers of various models or a range of instrumental equipment, such as everyday laptops, deep brain stimulators for therapeutic purposes, or external control devices like wheelchairs and prosthetic limbs.
Source: China Renaissance Analysis
2. History of Brain-Computer Interface Development
Academic validation and practical applications of brain-computer interfaces have a history spanning several decades, while academic exploration of electroencephalography (EEG) dates back even further.
In 1924, German psychiatrist Hans Berger discovered brainwaves, ushering in the era of digital recording of human brain activity. In 1970, the first paper on brain-computer interfaces (BCIs) was published, and the U.S. Defense Advanced Research Projects Agency (DARPA) began to venture into the field of BCIs. In 2004, BCI technology advanced from the stage of scientific validation to that of applied experimentation, exemplified by the pioneering BCI company BrainGate’s achievement in treating paralyzed patients using invasive brain-computer interfaces. Notably, in 2014, this same paralyzed patient performed the ceremonial kickoff at the FIFA World Cup in Brazil with the aid of a BCI and an exoskeleton.
In recent years, brain-computer interface (BCI) startups both in China and abroad have unveiled their conceptual products, with Elon Musk’s Neuralink being the most representative. As neuroscience and related technologies continue to achieve breakthroughs, BCI technology has entered a phase of rapid development.
3. The Significance of Brain-Computer Interfaces
As a disruptive technology, brain-computer interfaces (BCIs) demonstrate significant value in disease treatment and functional recovery within the medical field.
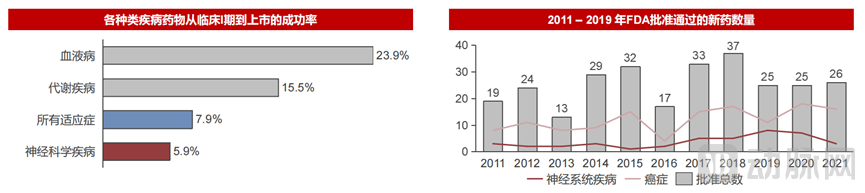
First, the global population of patients with brain disorders is substantial, and significant unmet clinical needs persist. Second, drug development for brain diseases is highly challenging; the pathogenic mechanisms of many neurological and psychiatric disorders remain poorly understood, clinical trial design is complex, and neurotherapeutic agents are often associated with pronounced side effects.
Source: BIO, QLS Advisors, Biomedtracker
As shown in the figure, the probability of brain disease-related drugs progressing from clinical trials to final market approval is only 5.9%, the lowest R&D success rate among all therapeutic areas. Furthermore, the number of newly approved drugs for neurological disorders has remained in the single digits in recent years. Therefore, as a strong candidate for innovative therapies, brain-computer interfaces (BCIs) hold promise for breaking this deadlock by overcoming the limitations of current treatment modalities and drug development, thereby curing brain diseases and restoring impaired brain function.
4. Governments of various countries attach great importance to brain science research
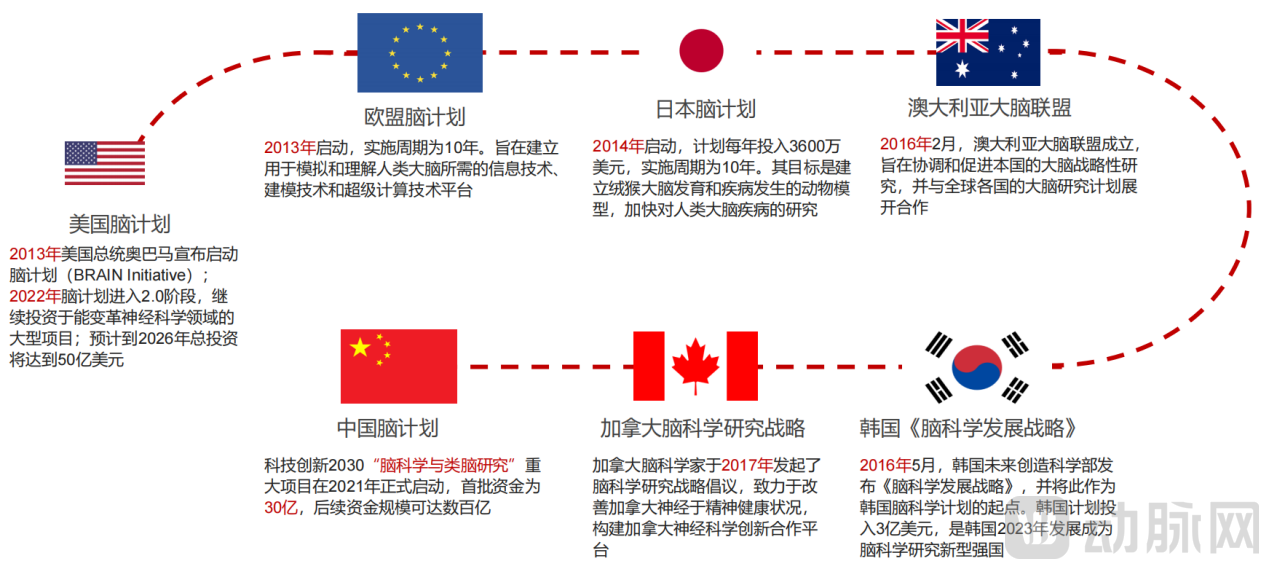
In response to unmet clinical needs, governments worldwide have begun to prioritize brain science research, launching major national-level initiatives. China’s Brain Project focuses on brain science and brain-inspired intelligence research.
Neuroscience research focuses on the neural basis of cognitive functions, aiming to unravel the secrets of the brain; brain-inspired research leverages our understanding of the brain to develop next-generation artificial intelligence technologies. Research and technology transfer in these fields will attract significant attention. However, we must clearly recognize that many core technologies in neuroscience and brain-computer interface (BCI) fields are not yet fully independent and controllable. For instance, domestic electroencephalogram (EEG) signal acquisition equipment heavily relies on imports, and there is an urgent need to develop Chinese-made core BCI components such as BCI chips and electrodes. Particularly against the backdrop of the U.S. Department of Commerce adding brain-computer interface technology to its export control list in October 2021, achieving full independence and controllability over BCI technology has become a long-term, arduous, yet imperative task for us.
Source: China Renaissance Analysis
Essentially, brain-computer interfaces (BCIs) utilize neural activity as control signals to enable direct communication between the human brain and the external environment (computers or other external devices). Signals of neural activity include electrical signals, magnetic signals, hemodynamic changes, and metabolic information. Since the essence of neural activity lies in the generation and transmission of electrical signals, this study will focus on elaborating methods for detecting and stimulating electrical signals, as well as the types of electroencephalogram (EEG)-based BCI signals.
1. Three Interaction Paradigms Between Brain-Computer Interfaces and the Brain
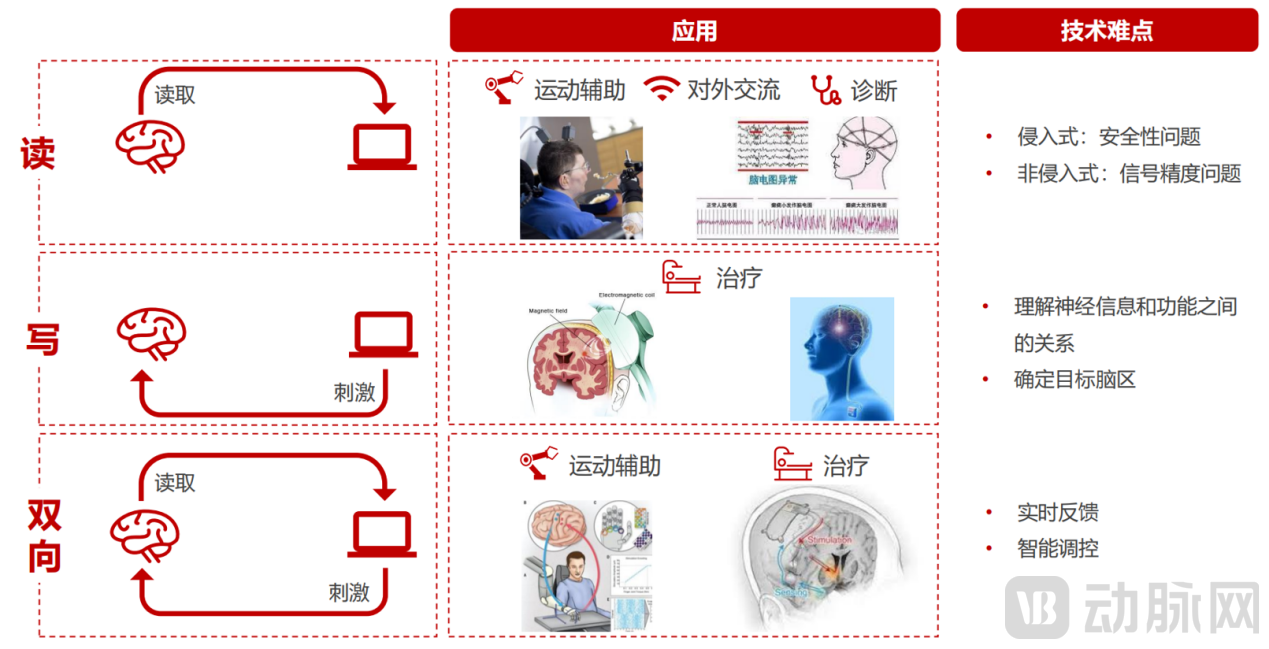
There are three paradigms for interaction between brain-computer interfaces (BCIs) and the brain: read, write, and bidirectional. The first is “read,” which involves recording brain signals—for example, using invasive or non-invasive techniques to detect neural activity by reading electrical signals or blood oxygenation levels from the brain. The second is “write,” which entails delivering energy or signals into the brain through electrical, magnetic, or ultrasonic stimulation, thereby exciting, inhibiting, or modulating neural signals to improve brain function. The third is “bidirectional,” which integrates the previous two interaction paradigms to achieve coordinated recording and stimulation.
1) Reading (recording brain signals)
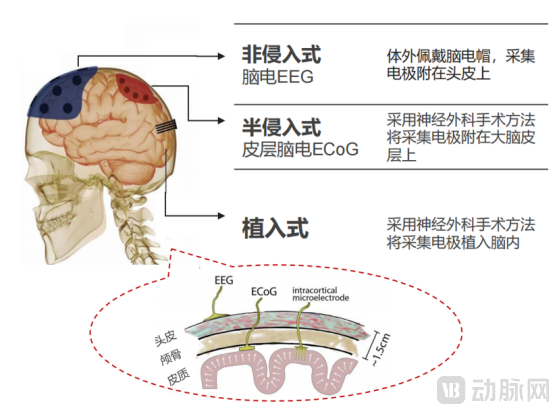
Classified by operating mode, technologies for recording electroencephalogram (EEG) signals are divided into invasive and non-invasive types, with the distinction lying in whether penetration of the skull is required.
Source: China Renaissance Analysis
a. Non-invasive EEG Detection
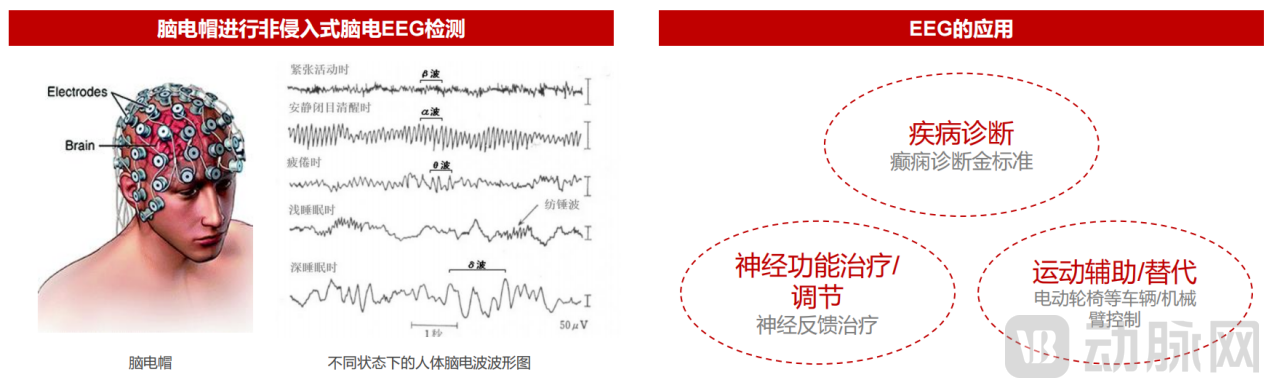
Non-invasive EEG detection primarily relies on electroencephalography (EEG) to capture the coordinated activity of multiple neurons. The acquisition devices do not penetrate the human brain and require only external wear.
Because the skull and dura mater attenuate certain high-frequency signals, and EEG signals are highly susceptible to external interference, EEG exhibits a low signal-to-noise ratio, limited spatial resolution, and reduced functional information content. However, due to its non-invasive nature and low cost, EEG is widely used in numerous consumer healthcare applications as well as select clinical medical settings. Currently, electroencephalography (EEG) is the gold standard for epilepsy diagnosis and is also applied in neuromodulation therapies and the control of electric wheelchairs or robotic arms.
Source: China Renaissance Analysis
b. Invasive Electroencephalography (EEG) Monitoring
Invasive electroencephalography (EEG) requires craniotomy for electrode placement to directly acquire brain signals from the cerebral cortex. This approach features a short signal acquisition path with minimal interference, achieving a temporal resolution of less than 0.01 seconds and a spatial resolution at the micrometer level, thereby capturing higher-quality EEG signals. However, its widespread application is limited by significant technical challenges, high clinical risks, and prohibitive costs.
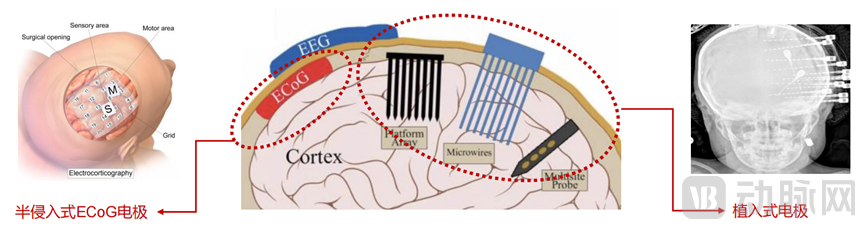
As shown in the figure below, invasive electroencephalography (EEG) can be further subdivided into semi-invasive EEG and implanted EEG, depending on whether the electrodes are placed within the cortex or based on the degree of invasiveness.
Source: China Renaissance Analysis
(1) Semi-invasive electrocorticography (ECoG)
A planar flexible electrode is applied directly onto the cerebral cortex, akin to a plaster, following craniotomy, without penetrating the cortical tissue. Compared with electroencephalography (EEG), electrocorticography (ECoG) mitigates the attenuation caused by the skull, offering higher spatial resolution, and is frequently employed for the precise preoperative localization of epileptic foci.
(2) Implantable EEG
Implantable electrodes typically require a craniotomy for placement. Both the surgical implantation and long-term displacement between the electrodes and brain tissue can cause damage to neural structures, posing significant safety concerns. Nevertheless, due to their ability to record high-frequency signals, precisely localize abnormal neurons, and directly target pathological foci, implantable electrodes remain powerful tools for neuroscience research and the management of neurological disorders.
In summary, in terms of signal quality, the ranking is: invasive > semi-invasive > non-invasive. However, both surgical trauma and long-term injury risks are higher for invasive approaches than for non-invasive ones, making non-invasive methods safer. Invasive techniques require neurosurgical procedures and pose risks of physical and immune-mediated damage from long-term electrode presence in the brain. The high technical complexity has resulted in fewer than 5% of current brain-computer interface (BCI) companies relying on invasive technologies.

Source: China Renaissance Analysis
2) Writing (Stimulates the Brain)
In addition to outputting brain signals, we can also attempt to input signals into the brain. Based on their mode of operation, stimulation methods can be categorized as non-invasive or invasive; based on technical approach, they can be classified as electrical stimulation or non-electrical stimulation.

Source: China Renaissance Analysis
There are three approaches based on electrical stimulation:
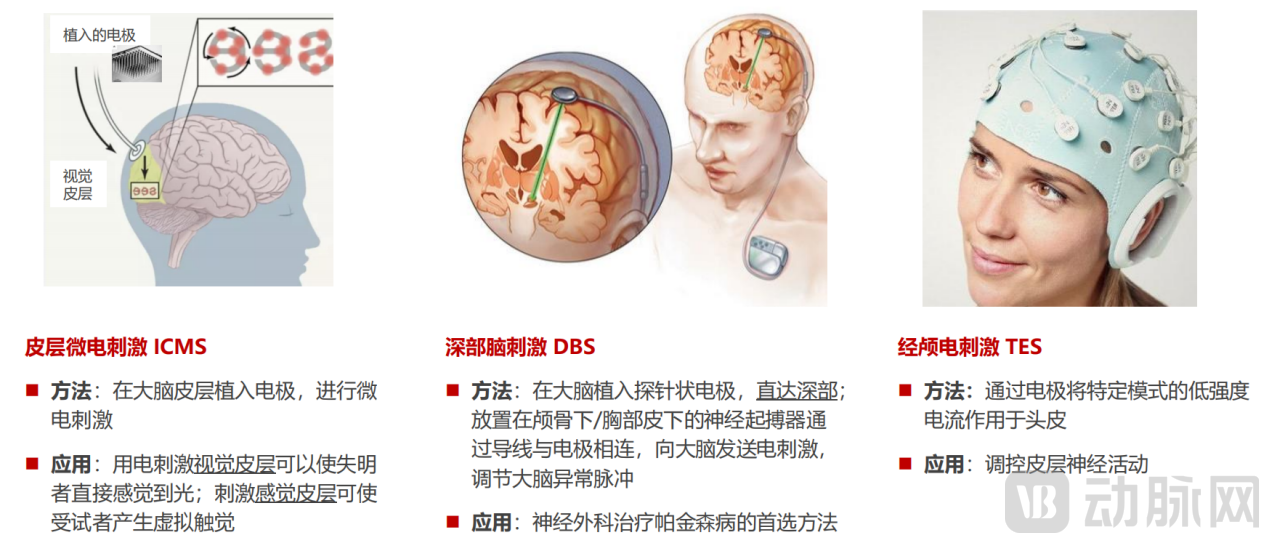
Source: China Renaissance Analysis
Two non-electrical stimulation approaches are as follows:
Source: China Renaissance Analysis
3) Bidirectional Interaction (Synchronous Recording and Stimulation)
What we hope to see is a more intelligent form of brain-computer interface (BCI): a closed-loop BCI that integrates both recording and stimulation, enabling bidirectional information flow with both output and input capabilities.
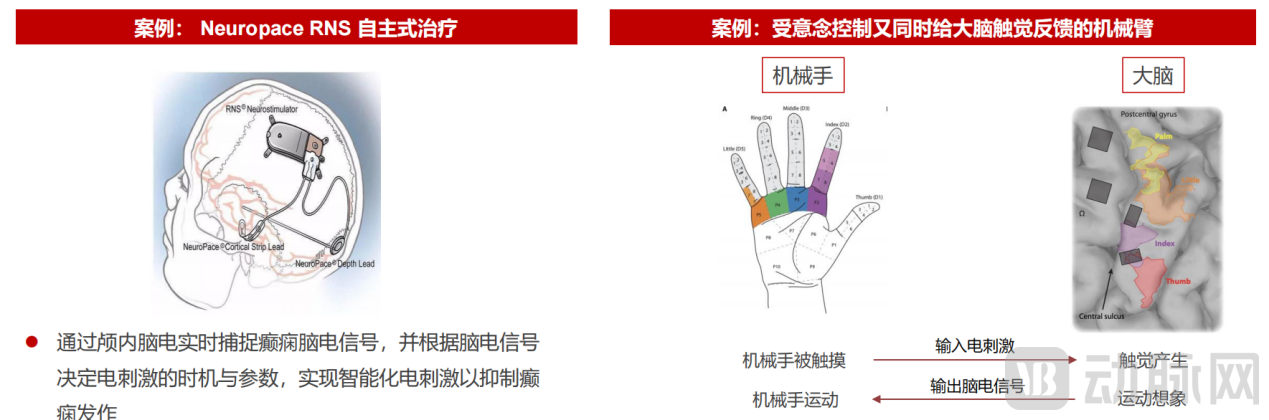
A representative example of such closed-loop brain-computer interfaces is Neuropace’s autonomous epilepsy treatment system. It comprises recording electrodes, a neurostimulator, and stimulation electrodes, with the neurostimulator serving as the intelligent core. By analyzing monitored abnormal cerebral discharges, it determines when to deliver electrical stimulation, thereby enabling more precise and effective therapy.
Another example is the robotic hand with haptic feedback. Traditional robotic hands are controlled via electroencephalography (EEG) or electromyography (EMG), featuring only signal output without active response to external stimuli; for instance, they do not withdraw when pricked by a sharp object. However, there should be interaction between the brain and the hand: while the brain sends motor control commands to the hand, the hand should also feed information back to the brain in the form of tactile sensations. Robotic hands with haptic feedback achieve this bidirectional interaction, more authentically replicating the communication patterns of native neural pathways, thereby offering greater application value.
Source: China Renaissance Capital Analysis, Neuropace Official Website
Summary of these three interaction methods: Reading, primarily applied in motor assistance and external communication (such as mind-controlled robotic arms and thought-based typing), is also used in disease diagnosis.
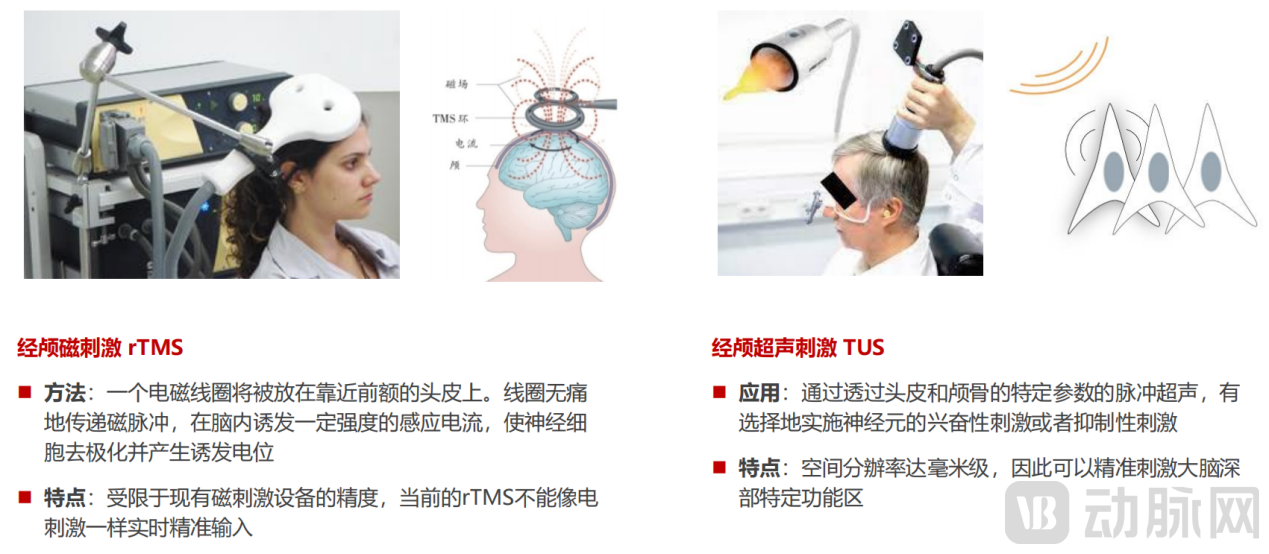
Brain stimulation, primarily applied in disease treatment—such as transcranial magnetic stimulation (TMS) for autism—faces two major technical challenges. The first lies in understanding the relationship between neural information and function; for instance, determining how the amplitude and frequency of electrical signals input into the sensory cortex to evoke virtual touch influence the perceived intensity of that sensation. The second challenge pertains to therapeutic brain stimulation techniques, which require identifying the specific brain regions whose stimulation yields optimal therapeutic outcomes.
Bidirectional Interaction: This is the technological approach we anticipate most. When applied to therapy, bidirectional brain-computer interfaces (BCIs) offer superior therapeutic efficacy compared to unidirectional systems; when used for motor assistance, they can better replicate the interaction patterns of natural neural pathways. Bidirectional BCIs require real-time feedback and intelligent regulation, making them more challenging to implement but also more valuable.
Source: China Renaissance Analysis
2. Application Scenarios of Brain-Computer Interfaces:
Non-invasive brain-computer interfaces are applied in both consumer and clinical settings. Typical consumer-grade applications include sleep monitoring, early detection and recovery monitoring of depressive mood, and stress emotion monitoring. Clinical-grade applications include consciousness monitoring, improvement of disorders of consciousness, amelioration of cognitive impairment, reduction of disability associated with mental illnesses, management of attention-deficit/hyperactivity disorder (ADHD) in children, and sensory substitution for auditory, visual, and tactile deficits.

Source: China Renaissance Analysis
In contrast, invasive brain-computer interfaces are primarily used for clinical-grade applications, with specific clinical indications leaning toward refractory neurological disorders such as epilepsy and motor impairments.

Source: China Renaissance Analysis
1) Application Examples in the Consumer Healthcare Sector—Emotional Assessment and Intervention
For emotions such as depression, traditional identification methods in the field of psychotherapy primarily rely on comprehensive scales based on dimensions like facial expressions, body language, and speech, making accurate quantitative assessment challenging. However, by recognizing the phase and amplitude of electroencephalogram (EEG) signals, it is possible to more accurately monitor and assess patients' emotional states. Furthermore, specialized training tasks can be designed targeting EEG signatures associated with specific emotions to adjust patients' conditions, thereby achieving precise regulation.
2) Application Examples in the Field of Serious Medical Care—Treatment of Central Nervous System (CNS) Diseases
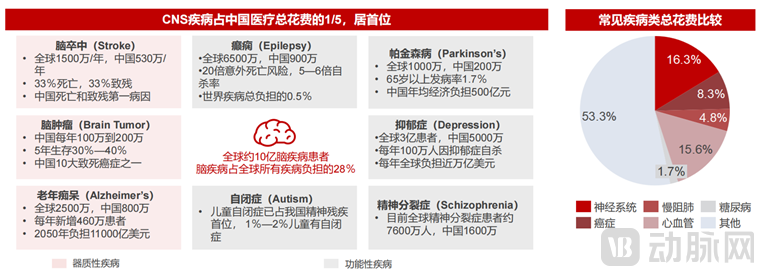
The most significant application of brain-computer interfaces in serious medical care is the treatment of central nervous system (CNS) disorders. CNS disorders currently account for one-fifth of total healthcare expenditures among Chinese residents, ranking first and surpassing cancer. These disorders are categorized into organic and functional diseases, both of which affect a substantial patient population.
Source: China Renaissance Analysis
Among these, organic diseases involve brain tissue damage caused by external forces, cerebral ischemia, or cellular pathology; typical examples include concussion, stroke, Alzheimer’s disease, and brain tumors. For such conditions, brain-computer interface (BCI) interventions are primarily palliative, aiming to improve patients’ quality of life. In contrast, functional brain disorders arise from neural dysfunction; typical examples include epilepsy, Parkinson’s disease, schizophrenia, depression, anxiety disorders, and addiction. For these conditions, BCI therapies aim to achieve a cure.
For example, brain-computer interfaces (BCIs) help stroke patients with aphasia and paralysis achieve communication freedom by reconstructing pathways for external brain interaction. Additionally, the principle of using BCIs for rehabilitative brain stimulation has been applied to spinal cord stimulation within the central nervous system to restore motor function. Some paralyzed patients retain intact limbs and can still perform motor imagery in the brain; however, due to nerve damage, motor commands fail to reach the limbs. In such cases, motor function can be restored by establishing external neural pathways. For instance, Onward has designed a spinal cord electrical stimulator that targets all nerves in the spinal cord associated with leg and trunk movement, enabling paralyzed patients to rapidly regain independent mobility.
1. Market Size of Brain-Computer Interfaces
According to McKinsey’s estimates, the potential market size for global medical applications of brain-computer interfaces (BCIs) is expected to reach $40–145 billion between 2030 and 2040. Within this, the potential market size for serious medical applications ranges from $15–85 billion, while that for consumer healthcare applications ranges from $25–60 billion.
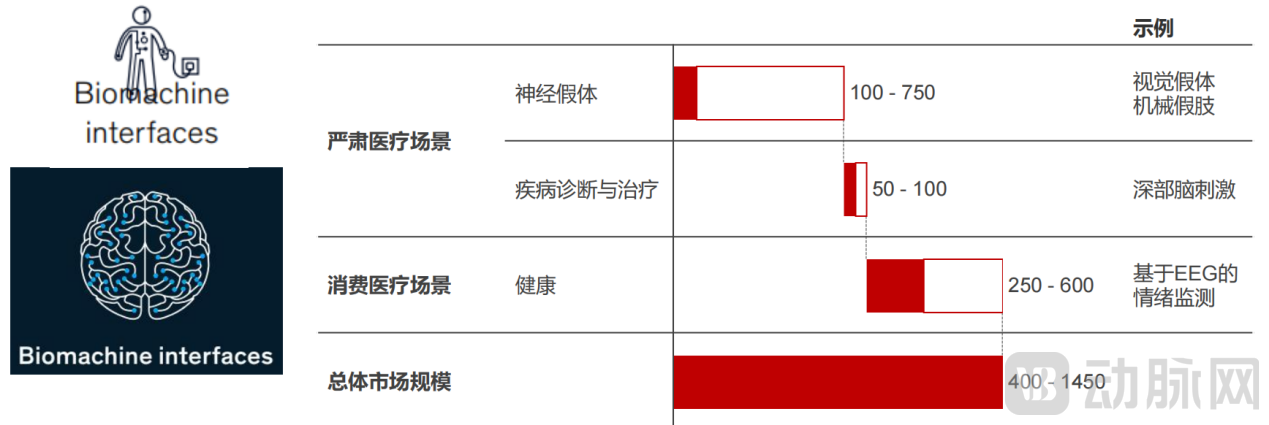
Source: McKinsey, Huaxing Capital Analysis
According to research and estimates by the Huaxing Medical Investment Team, based on a unit price of RMB 50,000 per brain-computer interface (BCI) device (excluding sales of services and other consumables), the potential market size for BCI in China’s serious medical sector exceeds RMB 100 billion. Among this, stroke rehabilitation and refractory epilepsy represent the largest market segments and are currently the most clinically mature areas in terms of exploration and application.
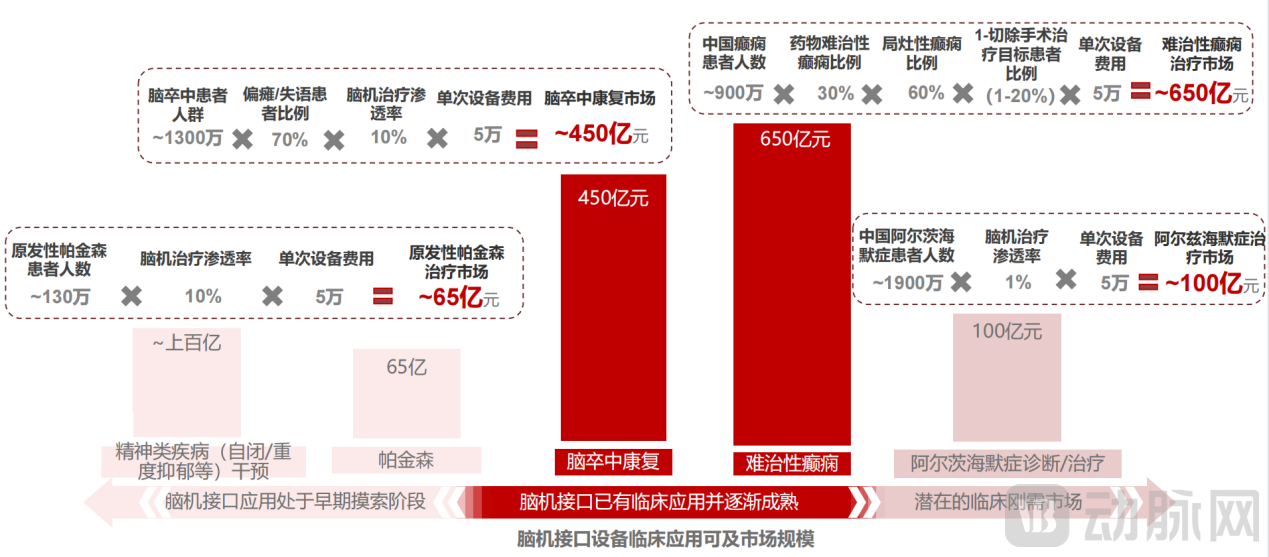
Source: China Renaissance Analysis
2. Analysis of the Brain-Computer Interface Industry Chain and Core Barriers
The upstream segment of the brain-computer interface (BCI) industry chain comprises hardware, software, and brain function research. Hardware primarily includes chips, electrodes, probes, and robotic systems for electrode implantation; software mainly consists of algorithms and platforms for decoding BCI signals; and brain function research serves as foundational infrastructure for the entire industry. Currently, clinical research on the brain remains in its early stages. With the aid of imaging modalities such as CT and MRI, we can assess whether the morphological structure of various brain regions is intact based on neuroimaging findings. However, brain region functionality remains a “black box,” and the clinical community lacks the capability to quantitatively evaluate brain function.
In the upstream segment of the industry chain, electrodes and chips constitute the core barriers to entry, and are currently the focus of intensive technological breakthroughs by many domestic and international companies, including Neuralink, Blackrock Neurotech, and Neuropixels.
The midstream segment of the industry chain comprises companies that develop brain-computer interface (BCI) platforms and BCI access devices, such as exoskeletons and wearable equipment. This category includes not only traditional deep brain stimulation (DBS) and vagus nerve stimulation (VNS) devices but also other novel invasive BCIs, as well as non-invasive and minimally invasive endovascular BCIs. Downstream applications of BCIs primarily encompass digital therapeutics, augmented reality/virtual reality (AR/VR), and interactive communication.

Source: China Renaissance Analysis
3. New Technological Directions in Brain-Computer Interfaces: Endovascular Stent Technology
Previous implantable brain-computer interface (BCI) technologies involved procedures such as drilling holes in the skull and inserting electrode needles directly into brain tissue, methods that could lead to chronic neuroinflammation in patients. Synchron’s Stentrode, a minimally invasive BCI device, is distinctive in that it utilizes endovascular techniques to deliver a stent-like BCI device from the jugular vein at the base of the neck into the cerebral vasculature, where it records and translates neural activity from within the blood vessels. Synchron’s product has received the FDA Breakthrough Device designation and is currently advancing through clinical trials, while several companies in China are also pursuing similar technological approaches.

Source: China Renaissance Capital Analysis, Synchron Official Website
1. Classification of Brain-Computer Interfaces

Source: China Renaissance Analysis
Brain-computer interfaces (BCIs) can be classified into output, input, and closed-loop feedback types based on the direction of information flow; into invasive and non-invasive types based on their mode of operation; into serious medical and consumer scenarios based on application contexts; into upstream (hardware, software, and brain function research), midstream (product manufacturers), and downstream services based on the industry chain; and into product-based and service-based models based on business models.
In the treatment and functional rehabilitation of most major brain disorders, invasive brain-computer interfaces (BCIs) offer more pronounced technical advantages and are likely to become the mainstream approach addressing the needs of these patient populations.
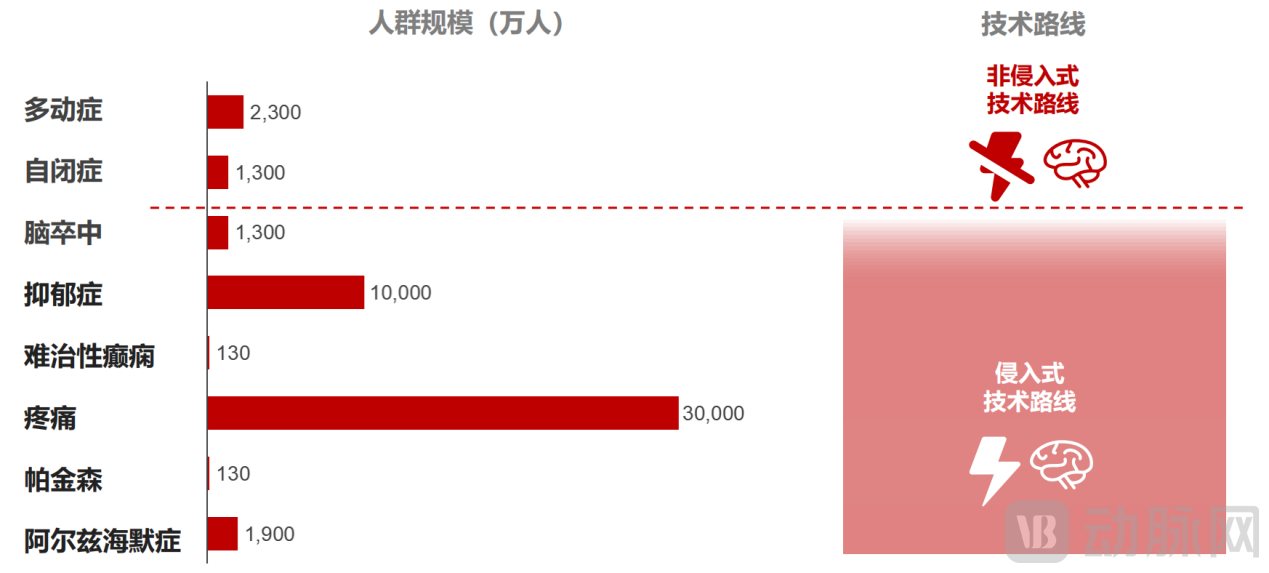
Source: China Renaissance Analysis
Based on a comprehensive analysis of various technological approaches, application scenarios, and business models, and considering the essential demand and market size for products related to the treatment and rehabilitation of major brain diseases, as well as the high technical barriers associated with invasive brain-computer interfaces (BCIs)—including electrodes, chips, electrode implantation robots, batteries, and signal acquisition and decoding—invasive BCIs will be our current primary focus.

Source: China Renaissance Analysis