Guoxin Health Advances Outpatient APG Reform to Close the Loop in China's Medical Insurance Payment System
Reading Guide:
DRG + APG: Closed-Loop Management of Health Insurance Payment Returns to the Essence of Medical Value
“Capitation” Model Introduced, Jinhua’s Advantages in Tiered Diagnosis and Treatment Become Evident
The "Jinhua Model" of Collaborative Management for Outpatient and Inpatient CareHow to Copy
APG Reform Points to “Health Performance” Through Synergy
In March 2022, the Zhejiang Provincial Healthcare Security Administration issued the "Three-Year Action Plan for Comprehensively Advancing the Reform of Medical Insurance Payment Methods in Zhejiang Province," ushering in a new phase of medical insurance payment reform. The province took the lead in comprehensively advancing the reform of outpatient capitation combined with Ambulatory Patient Groups (hereinafter referred to as APG) payment methods, aiming to establish a closed-loop system for payment method reforms covering both outpatient and inpatient expenses across the province.
Compared with DRG/DIP, which focus on controlling medical insurance costs, the value of closed-loop management integrated with APG extends beyond optimizing hospital operations and restructuring the healthcare service system. From a design perspective, this innovative approach can improve outpatient care outcomes by standardizing diagnosis and treatment and implementing whole-process management, reduce inpatient resource consumption, shift the responsibility for chronic disease management to primary care institutions, and move health interventions upstream. Ultimately, it aims to be accountable for the population’s “health performance” and drive the formation of a “Health Community.”
Over the past two years, Jinhua City in Zhejiang Province has taken the lead in demonstrating the value of Ambulatory Payment Groups (APG) through empirical data. Following the implementation of reforms, the growth rate of health insurance fund expenditures for outpatient medical expenses in Jinhua City decreased from approximately 25% before the reform to within the provincial target of 10% in 2020.[1], forming a closed-loop management system with total budget control alongside the inpatient “disease group point-based” payment method, further improving the long-term balance mechanism of medical insurance funds and enhancing the efficiency of their utilization.
These significant achievements have also been recognized by the highest industry regulatory authorities. At the Smart Medical Insurance Solutions Competition hosted by the National Healthcare Security Administration, China Reform Health’s “Refined Multi-Layered Composite Payment Service Scheme for Outpatient Medical Insurance,” developed based on Jinhua City’s reform experience, was honored as the only award-winning solution in the field of payment methods.
It is foreseeable that once the implementation of DRG/DIP systems is completed across all regions in China, adopting APG as the next step in reform may emerge as another trend promoting the healthy development of the industry.
At its core, the reform of health insurance payment methods for both outpatient and inpatient services represents a shift from volume-based to value-based reimbursement. This trend was already analyzed in a 2017 third-party evaluation conducted by the Institute of Hospital Management at Tsinghua University on the implementation effects of Jinhua’s “Diagnosis-Related Group (DRG) Point System” reform. According to Professor Yang Yansui of the Institute of Hospital Management at Tsinghua University, “This value-based payment approach differentiates physicians’ labor based on diagnostic importance, surgical necessity, and service effectiveness, and determines reimbursement rates and the allocation of health insurance fund points through negotiation using median values for the same conditions within the same region. Such a quality-oriented payment method marks significant progress for humanity and is now being implemented in China.”
Building on the strong performance of inpatient medical insurance funds and the operational efficiency of healthcare institutions, Jinhua City has taken a pioneering step in exploring and innovating outpatient Ambulatory Payment Group (APG) payment reform, adhering to the core value orientation of improving healthcare service quality. As an integral component of the systemic reform of medical insurance payment, the outpatient APG reform is calculated based on inpatient data, complementing the inpatient payment method reform to drive comprehensive progress.
Simply put, Ambulatory Patient Groups (APG) classify hospital outpatient cases based on procedures combined with diagnoses, grouping patients with similar clinical resource utilization. Similar to the payment logic of Diagnosis-Related Groups (DRG) and Big Data Diagnosis-Intervention Packet (DIP), APG adopts bundled payments for disease groups under the framework of global budgeting plus the point-based method.
In the "Jinhua City Basic Medical Insurance Outpatient Payment Measures (Trial)" issued by the Jinhua Municipal Healthcare Security Administration, the Jinhua Ambulatory Patient Groups (APG) system primarily consolidates multiple settlement cases with the same primary diagnosis for a single patient within one treatment cycle (currently provisionally defined as one day) at the same medical institution into a single case, based on similarities in clinical processes and resource utilization. Through clustering, APG groups tailored to the actual conditions of Jinhua City are formed. Following rigorous statistical analysis and calculations, the APG groups in Jinhua City are ultimately categorized into Surgical Procedure APGs, Diagnostic APGs, and Ancillary APGs, comprising 1,391 subgroups. Thus, an outpatient case grouper system with distinct local characteristics of Jinhua has been established.
The outpatient case grouper system, featuring such granular classification, has formed the “backbone” of Jinhua City’s reform in healthcare insurance payment methods. Specifically, this grouper can seamlessly integrate with the inpatient “Diagnosis-Related Group (DRG) point-based method,” creating a closed-loop system for global budget management and establishing positive incentives that simultaneously benefit healthcare institutions, physicians, and patients.
For medical institutions,, the APG payment method effectively stimulated the endogenous motivation of medical institutions to proactively control outpatient costs and treatment expenses, avoiding the “mole problem” under a single inpatient system (the shift of inpatient costs to outpatient services under DRG/DIP payment), and achieved effective and controllable budget management of medical insurance expenses at the hospital-wide level.
For physicians,The APG grouping design references outpatient diagnostic and procedural data from all medical institutions within a defined region, ensuring that disease categorization aligns closely with clinical practice and thereby reducing the complexity of clinical workflows for physicians. Meanwhile, the weights assigned to each group have been rigorously validated by experts, helping to reflect the true value of medical services and providing positive incentives for physicians’ clinical behavior.
For patients,, APG adopts standardized and unified medical diagnostic and procedural standards. The quality control department oversees the standardization of medical record documentation, the completeness of information, the accuracy of treatment plans, and the incidence of hospital-acquired infections. This approach effectively reduces patients’ financial burden, enabling them to access standardized clinical diagnostic and procedural services at relatively stable and lower costs, thereby enhancing the cost-effectiveness of healthcare services for patients.
This “closed-loop approach” has yielded immediate results in Jinhua City. Taking the municipal level as an example, the growth rate of the outpatient medical insurance fund was controlled at 7% in 2020, a significant decrease from the 20.08% growth rate in 2019, thereby initially achieving the goals of “controlling the fund” and “improving quality.”[2]。
It is worth noting that the introduction of APG grouping is not the entirety of Jinhua’s medical insurance reform. Establishing a closed-loop system for global budget management can resolve issues related to medical insurance payment and settlement within individual hospitals. However, given the broader trend of regional healthcare development, healthcare reforms cannot be limited to single hospitals; they must also ensure the effective implementation of tiered diagnosis and treatment, accelerate the synchronized development of primary care institutions and higher-level hospitals, and ultimately build a comprehensive and reliable regional healthcare service system.
Therefore, building upon the grouping of outpatient cases, Jinhua City has also introduced a capitation system. With the collaboration of China Reform Health Management and Services Group Co., Ltd., it has developed a composite payment method that combines global budgeting with capitation and the APG point-based system, selecting either capitation or APG point-based payment according to the specific circumstances of general outpatient care, chronic disease outpatient care, and special disease outpatient care.
Capitation-Based Lump-Sum Payment Model under Global Budgeting
Capitation-based payment is relatively rare in China, but it aligns well with Jinhua’s healthcare policies.
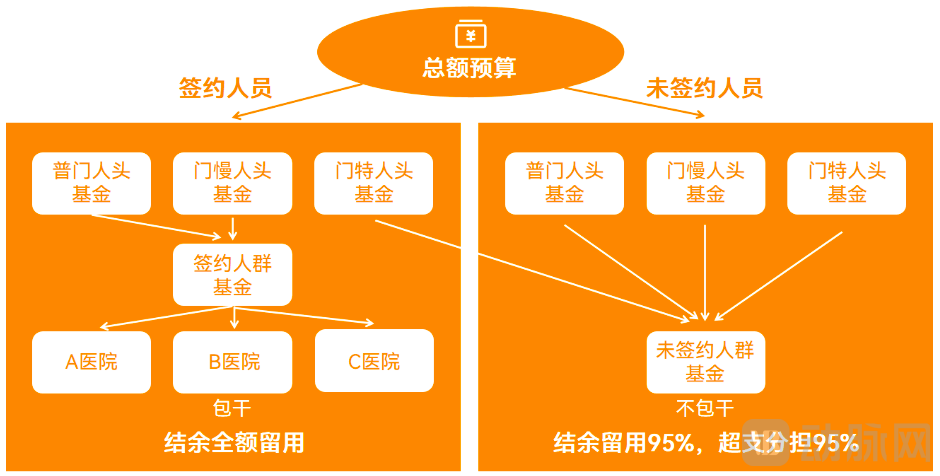
The so-called "capitation-based global budget" refers to a mechanism promoted by the Healthcare Security Administration, whereby medical institutions sign contracts with insured individuals, thereby allocating the outpatient capitation fund for these enrollees to the contracted medical institutions (or medical consortia) for pooled use. Under a fixed total budget, the greater the surplus generated from outpatient services, the larger the amount retained by the medical institution; conversely, any deficits shall be borne solely by the institution itself.
Under the current outpatient payment mechanism, all outpatient services constitute revenue for healthcare institutions. This structure may incentivize providers to pursue higher outpatient volumes and more diagnostic tests, thereby siphoning off patients, while offering little motivation to prioritize disease prevention and health management. Such a system is also detrimental to the healthy development of primary care.
Capitation-based payment can steer health insurance funds toward contracted services and primary care institutions. On one hand, by binding insured individuals to contracts with corresponding capitation payments, primary medical institutions can sustain and develop their operations, thereby further enhancing their medical technical capabilities. On the other hand, as chronic disease management, which accounts for a significant proportion of outpatient visits, is shifted to primary care institutions, small and medium-sized clinics have become key instruments for resident health management, allowing large hospitals to allocate more resources to addressing complex and intractable diseases. Driven by the synergistic effect of these two incentives, the virtuous cycle of “tiered diagnosis and treatment” is gradually being realized through the reform of health insurance payment mechanisms.
Public data provides a detailed account of the achievements made over the two-year pilot period of outpatient payment reform in Jinhua City:
First, the growth in outpatient fund expenditures has been effectively controlled. The growth rate has decreased from approximately 25% prior to the reform to within the provincial target of 10%, with over 70% of medical institutions benefiting from the “retention of surplus” incentive policy, involving a total surplus of RMB 9.49 million.
Secondly,, the capacity of primary healthcare institutions and the number of contracted residents have continued to increase. The annual number of visits by contracted insured patients has risen by 18% per year, with the proportion of visits at the primary care level increasing from 29.04% in 2019 to 34.74% in 2021, representing an average annual growth rate of 9.4%. Meanwhile, the ratio of outpatient visits to hospitalizations decreased from 1.54% in 2019 to 1.36% in 2021, with an average annual decline of 6.4%, effectively retaining more patients within the primary care system.
Finally, the average cost per visit for enrolled insured individuals decreased. It fell from 104.94 yuan in 2019 to 98.08 yuan, a decline of 6.54%, indicating a continuous reduction in medical expenses for the public.
Overall, with the support of China Reform Health Management and Services Group Co., Ltd. (Guoxin Health), Jinhua has completed a closed-loop reform of medical insurance payment spanning both inpatient and outpatient services. This initiative has ensured safe and controllable fund expenditures, enabled precise and efficient medical insurance payments, and rationally optimized healthcare delivery order. It has achieved a win-win outcome for insured individuals, medical institutions, and the medical insurance fund, while establishing a cost “benchmark” recognized by four key stakeholders: the medical insurance system, hospitals, physicians, and patients. These efforts have tangibly enhanced public satisfaction and sense of gain in accessing healthcare services.
As products of the post-healthcare informatization era, DRG and APG impose stringent requirements on the local “blood” and “musculoskeletal” foundations. The achievements made today in Zhejiang Province’s healthcare insurance payment system reform are attributable to the combined effects of multiple factors at both macro and micro levels.
Macro-level policy support has provided fertile ground for reform and innovation in Jinhua City. As early as July 2017, 49 medical institutions in the urban area of Jinhua had fully implemented the “Diagnosis-Related Group (DRG) Point-Based Method” for inpatient payment reform. In September of the same year, Jinhua was designated as the sole pilot city in Zhejiang Province for healthcare security payment method reforms, further accelerating the implementation of these systemic changes. By 2018, the Municipal Healthcare Security Administration required all designated medical institutions to adopt the “DRG Point-Based Method” for inpatient healthcare security payments, establishing 634 disease groups and achieving full coverage of all inpatient conditions across the city.
Support from provincial and municipal healthcare security administrations for Jinhua City’s implementation of innovative healthcare payment methods has enabled the city to undertake innovative reforms based on the national Diagnosis-Related Group (DRG) framework. In this process, in addition to aligning with key conditions such as Jinhua’s “family doctor” contracting system and the annual global budget for healthcare fund expenditures, the Healthcare Security Administration has continuously refined the “Disease Group Point System” in collaboration with hospitals. This effort has progressively advanced the closed-loop healthcare payment reform, shifting focus from “inpatient care” to an integrated “inpatient-outpatient” model, ultimately achieving the grand objective of “Health for All” while ensuring the sustainable growth of healthcare funds.
Furthermore, the Jinhua Municipal Healthcare Security Administration has established a collaborative regulatory mechanism for healthcare insurance funds in conjunction with the Health Commission, Public Security Bureau, Market Supervision Administration, Intermediate People’s Court, and People’s Procuratorate. By instituting robust frameworks for joint conferences, case consultations, and routine interdepartmental coordination, the city is accelerating the development of a regulatory landscape characterized by information sharing, mutual recognition of findings, and synergistic enforcement efforts. This multi-agency approach has effectively ensured the positive progression of the overall reform process from a regulatory standpoint.
Multiple macro-level factors have collectively contributed to Zhejiang Province’s current achievements in healthcare insurance reform. Policy formulation originates at the grassroots level, with implementation being the key, thereby establishing a replicable and scalable model and set of best practices. This requires a micro-level approach that takes into account the comprehensive circumstances of each region, enhancing the standardized service delivery and management capabilities of hospitals to improve the coordinated management efficiency of inpatient and outpatient care. In this process, improving the development and practical application of medical information management systems has become a crucial lever for facilitating the implementation of composite outpatient healthcare insurance payment methods.
The construction of outpatient information systems primarily encompasses foundational APG payment infrastructure, such as the implementation of outpatient electronic medical records (EMR) and the APG-based medical insurance settlement data upload system. It also includes APG payment application systems, such as APG patient classification and APG data operation management platforms. Given that the volume of outpatient classification data far exceeds that of inpatient data, there are stringent requirements for the structuring and standardization of patient data, as well as for the substantive quality of medical records, thereby posing a significant challenge to hospitals’ informatization capabilities. Furthermore, the successful adoption of APG necessitates the formulation of localized strategies tailored to regional development needs by integrating comprehensive local factors, including disease spectra, demographic characteristics, and health economics.
On the other hand, Ambulatory Patient Groups (APGs) represent a significant innovation under the bundled payment model for outpatient services. In response to the closed-loop management of outpatient and inpatient care within the health insurance payment mechanism, healthcare institutions must further strengthen standardized and coordinated management:
From the Perspective of Clinical Collaboration, whether in outpatient or inpatient settings, clinical departments are the direct providers of diagnostic and therapeutic services and constitute the core focus of hospital care process management. Therefore, establishing a collaborative clinical management mechanism, standardizing diagnostic and therapeutic practices, optimizing service workflows, and forming a high-quality, efficient bidirectional diagnostic and therapeutic service mechanism linking outpatient and inpatient care are essential pathways to achieving high-quality hospital development.
From the Perspective of Coding CollaborationWhether it is APG grouping or DRG/DIP grouping, the standardization of diagnoses, procedures, and medical items serves as a critical foundation for payment reform. Healthcare institutions should ensure the comprehensive implementation of the 15 national healthcare security information business codes, establish a collaborative coding management mechanism for outpatient and inpatient services, ensure standardized and unified coding across both settings, and safeguard the basis for fund payments.
From the Perspective of Medical Record Collaboration, the diagnostic information in outpatient medical records serves as the basis for APG payment. Strengthening the development and quality control of electronic outpatient medical records, and establishing a collaborative management and quality control mechanism for outpatient medical records and the front pages of inpatient medical records, has become the core of hospital internal management reform.
From the Perspective of Information CollaborationInternally, healthcare institutions should procure information systems with relatively unified standards for outpatient and inpatient management to avoid administrative chaos caused by inconsistencies among multiple systems. Externally, they should transmit the data required for APG/DRG/DIP payment models in a timely, accurate, and comprehensive manner, ensuring real-time transmission of health insurance information and prompt feedback on grouping results and relevant management indicators.
To meet the needs of multiple stakeholders from various perspectives, it is essential not only to ensure full communication between supply and demand sides but also to foster collaborative development with professional third-party service providers. These agencies assist the Healthcare Security Administration in thoroughly implementing a comprehensive reform framework within medical institutions, thereby achieving coordinated reforms between healthcare security and medical institutions. This approach serves as an effective guarantee for fulfilling the “Promoting Coordinated Reforms in Medical Institutions” requirement outlined in the National Healthcare Security Administration’s “Three-Year Action Plan,” and represents an inevitable trend toward high-quality development in the “three medicals” sector.
As early as when Jinhua City initiated its DRG reform, China Reform Health Management and Services Group Co., Ltd. (China Reform Health) joined the effort. The company has consistently partnered with the Jinhua Municipal Healthcare Security Administration to explore innovative approaches. Upon recognizing the necessity of implementing Ambulatory Patient Groups (APGs), China Reform Health promptly initiated discussions, and both parties jointly launched an APG point-based system tailored to Jinhua’s local context.
To ensure the smooth implementation of healthcare insurance payment reform in Jinhua City, China Reform Health has conducted an in-depth deconstruction of refined, multi-layered composite payment services for outpatient care. By establishing tiered positioning and categorized designs for tertiary hospitals and primary care institutions, and leveraging three core technologies—ACG (Adjusted Clinical Groups) capitation grouping, APG (Ambulatory Patient Groups) case grouping, and population health assessment—the company has developed an integrated outpatient payment solution. This solution combines refined capitation budget allocation, precise outpatient payment mechanisms, and detailed performance evaluation for contracted services. It reconstructs a composite payment system that applies diagnosis-related group (DRG)-based payments to tertiary hospitals and capitation-based payments to primary care institutions, thereby establishing a service mechanism that drives tertiary hospitals to take responsibility for disease diagnosis and treatment, while holding primary care institutions accountable for the health outcomes of insured individuals.
Meanwhile, China Reform Health has further explored and implemented initiatives in its collaboration with Jinhua City.APG-Based Intelligent Outpatient Management Services Centered on Lean Management of APG Disease GroupsBy implementing pre-visit medical record validation and medical record quality control management, we standardize the documentation of outpatient diagnoses and clinical practices, thereby enhancing the substantive quality of medical records. Through comprehensive query and analysis of cases and case-mix groups across three dimensions (hospital-wide, departmental, and physician-level) and two categories (APG grouping status and case-mix group types), we support internal hospital management and establish a standardized, comparable evaluation system for outpatient cost indicators. By conducting APG profit-and-loss analysis, we integrate process management with final account management to understand disease spectrum structure, optimize the admission and treatment of outpatient conditions, and provide strategic direction for disciplinary development. Furthermore, by monitoring changes in key indicators, we optimize the structure of outpatient costs and enhance cost control capabilities.
Currently, Zhejiang Province has launched a province-wide promotion of the APG point-based payment system. The experience accumulated through the “Jinhua Model” will be rapidly disseminated across the entire province in the near future. Building on this foundation, China Reform Health Management and Services Group Co., Ltd. (Guoxin Health) has demonstrated innovation in its practical implementation, enriching the system’s substance.R&D Upgrade of “APG2.0”, its core feature is the comprehensive consideration of local medical insurance policies and data conditions, adjusting the grouping logic and connotations, and categorizing APG groups into four types: separate payment, emergency care, outpatient single-disease, and general outpatient groups, enabling flexible adaptation to varying local circumstances.
Leveraging the advanced medical and health insurance informatization capabilities across cities in Zhejiang Province, their proactive embrace of reform, and the “localized” innovative service capabilities of third-party professional service providers, we are strengthening the “musculoskeletal” framework while enriching the “bloodstream.” As a result, we may witness a broader landscape of APG-based health insurance payment system reforms within the next few years.
Looking back on the more than two-year journey of Jinhua City’s APG reform, we have found that the implementation pathways and supporting elements for high-quality development—such as medical quality, cost control, resource utilization efficiency, healthcare service capacity, organizational management, institutional framework, and patient satisfaction—are being systematically linked and integrated through a closed-loop reform centered on the full cycle of health insurance payment and the entire management process, with data governance serving as the connecting thread.
Furthermore, from the perspective of health governance, Professor Yang Yansui’s team proposes that implementing health performance evaluations based on high-quality clinical data (resource utilization and patient information), and incorporating the evaluation results into capitation-weighted budgets (with high weighting) and incentive mechanisms, can guide tightly integrated medical consortia to adopt a development strategy and performance management model characterized by “excelling in treating diseases and saving lives by managing severe cases (increasing the Case Mix Index [CMI]), while grounding efforts in health maintenance (reducing disease incidence).” This approach facilitates the transition of health insurance payment systems from a disease-treatment-centric model to a health-maintenance-centric model.[3]。
In practice, the Jinhua Municipal Healthcare Security Administration, medical institutions represented by Jinhua Central Hospital, Tsinghua University’s Institute of Hospital Management, and China Reform Health have continuously optimized their collaborative efforts. By implementing a practical pathway grounded in clinical practice, driven by data, guided by rules, focused on disease groups, controlled by costs, refined through operations, and strengthened by performance management, they are further exploring the realization of a comprehensive closed-loop management system spanning both inpatient and outpatient care. This initiative aims to holistically enhance hospital service efficiency, operational effectiveness, and managerial performance.
When it comes to the future of medical insurance payment reform,Multiple parties have long reached a strong consensus.: The value orientation centered on people’s health and the development approach emphasizing quality and efficiency have permeated reforms across the entire “three medicals” (healthcare, medical insurance, and pharmaceutical) sectors. Against the backdrop of comprehensive advancement in healthcare payment method reforms, reducing unnecessary financial penalties for hospitals is not a zero-sum game favoring only regulators; nor is improving the utilization efficiency of medical insurance funds merely about generating surplus for payers. Ultimately, with medical institutions serving as the interactive hub, medical insurance agencies, health administrative authorities, hospitals, and third-party service providers are working in concert toward a common goal. They align their efforts around a shared “performance assessment indicator”—the “health outcomes” of the general population—thereby forming a patient-centered, health-focused community of collaborative care.
The spiral ascent of collaborative exploration among government, industry, academia, research institutions, and end-users also represents a pathway for multi-party cooperation to drive the high-quality development of medical insurance and healthcare services. As we actively respond to the evolving landscape of medical insurance payment reform, a new era characterized by more focused medical value, more inclusive medical services, and more sustainable medical security may be emerging.
References
[1][2] Jiang Xiaozhou. Exploratory Practice of Implementing the Outpatient “APG Point-Based” Payment Reform in Jinhua City[J]. China Health Insurance, 2021, 08: 49+52.
[3] Yang Yansui, Yu Miao, Zhang Dan. County-level Medical Communities Must Be Tightly Integrated; Mechanisms for Health Insurance Payment Need to Be Established [EB/OL]. https://www.yicai.com/news/101436502.html