China's New Hypertension Guideline Sparks Market Surge: Over 200 Million Additional Patients and a Billion-Dollar Opportunity
On November 14, the home medical device sector of China’s A-share market rallied, with Cofoe Medical closing up 14%, Yuwell Medical hitting the daily price limit, and Lifesense Medical closing up 8.48%. This surge was driven by the official release of the “Chinese Clinical Practice Guidelines for Hypertension” (hereinafter referred to as the “New Guidelines”), jointly developed by academic institutions including the National Center for Cardiovascular Diseases and the Chinese Medical Doctor Association.
“The New Guidelines” recommend lowering the diagnostic threshold for hypertension in Chinese adults to 130/80 mmHg. Based on the new criteria, the number of hypertensive patients in China is estimated to rise from 245 million to nearly 500 million, meaning that more than one-third of the population will be diagnosed with hypertension. The hypertension market is poised for explosive expansion.
On the evening of November 15, Xinhua News Agency republished content from the “Healthy China” WeChat official account, stating thatThe state has established standardized procedural requirements for the formulation and issuance of diagnostic criteria for diseases such as hypertension. Guidelines, consensus statements, and similar documents independently published by professional institutions, industry associations, or individuals represent expert research findings and do not constitute national diagnostic standards for diseases.Regarding the diagnostic criteria for hypertension, key educational materials, prevention and treatment guidelines, clinical pathways, and other documents issued by the national health administrative authorities in 2005, 2010, and 2017 have all clearly stated that the diagnostic criterion for hypertension in adults is blood pressure exceeding 140/90 mmHg on three separate occasions.Currently, the national diagnostic criteria for hypertension in adults have not been adjusted.Although the diagnostic criteria for hypertension remain unchanged, the market response has been tangible, reigniting activity in this sector.
Given that the national authorities have not yet adjusted the diagnostic criteria for hypertension, why does the New Guidelines recommend lowering the threshold?
At the press conference, Professor Zhao Dong from Beijing Anzhen Hospital, Capital Medical University, introduced that the adjustments in the New Guidelines are based on ample international and domestic evidence-based medical support. Moreover, individuals with blood pressure levels of 130–139 mmHg or 80–89 mmHg are predominantly young and middle-aged adults. Lowering the diagnostic criteria reflects the concept of moving the prevention line forward and strengthening initial prevention; otherwise, we will miss the critical opportunity to reduce the harm caused by hypertension-related cardiovascular diseases and other conditions.
Meanwhile, the New Guidelines recommend that all patients with hypertension should undergo lifestyle interventions, including dietary modifications, physical exercise, stress management, weight reduction, smoking cessation, alcohol moderation, and comprehensive lifestyle interventions. Furthermore, based on substantial evidence from evidence-based medicine, it is recommended that most hypertensive patients lower their blood pressure to below 130/80 mmHg, including those without cardiovascular comorbidities, as well as those with coronary heart disease, chronic heart failure, a history of stroke, chronic kidney disease, diabetes, or elderly hypertension.
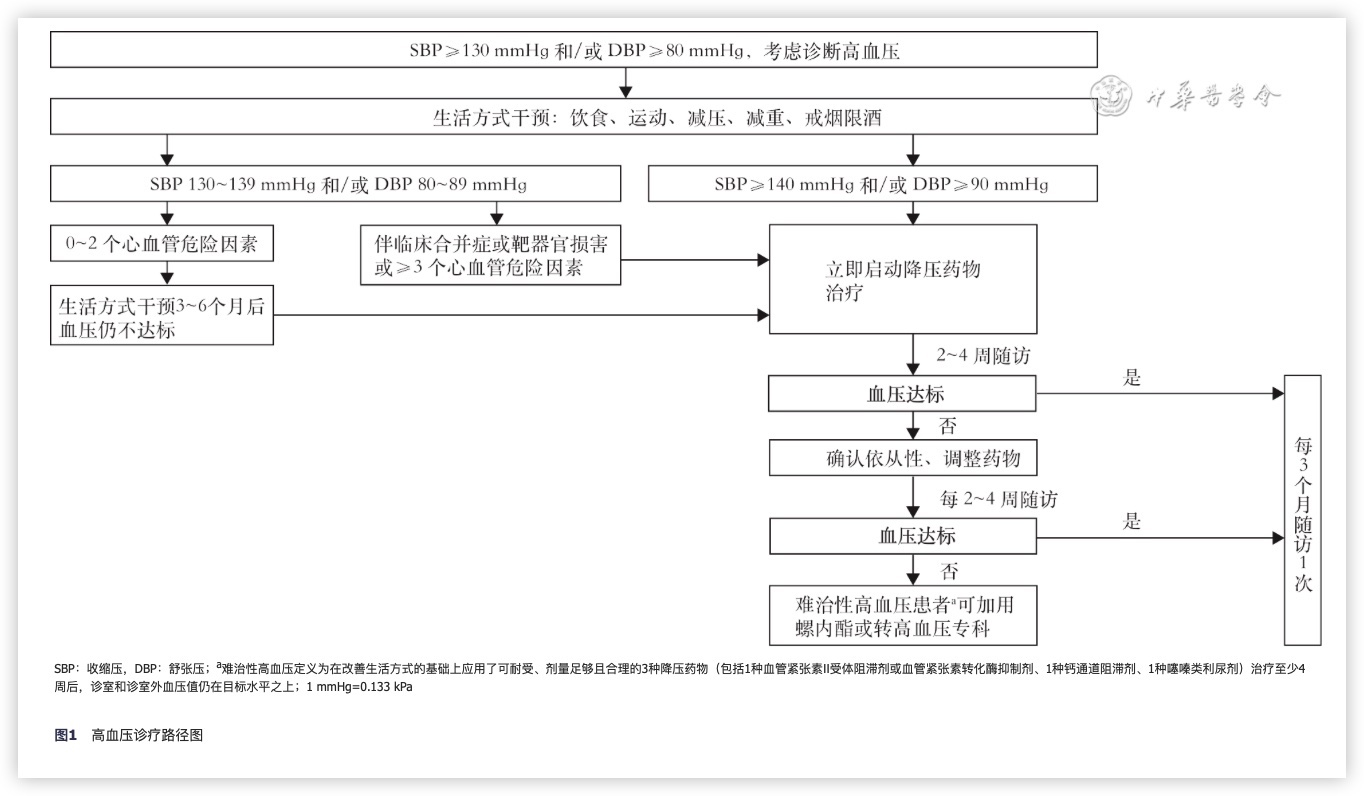
New Diagnostic and Treatment Pathway for Hypertension, Image Source: “New Guidelines”
For frontline clinicians, the more simplified the stratification criteria are, the greater their operability and scalability, facilitating prompt determination of the timing for initiating antihypertensive therapy in patients with hypertension. At the press conference, Professor Yu Jing from the Second Hospital of Lanzhou University also stated that the New Guidelines recommend the active initiation of antihypertensive pharmacotherapy for patients at high cardiovascular risk, while low-risk patients may undergo 3–6 months of lifestyle interventions; if blood pressure targets remain unmet, antihypertensive pharmacotherapy may be initiated.
At the press conference, Han Yaling, an academician of the Chinese Academy of Engineering, pointed out that although lowering the diagnostic threshold for hypertension has expanded the population classified as hypertensive and may slightly increase costs for early-stage treatment, it will substantially reduce the high expenses associated with treating severe complications—such as stroke, myocardial infarction, and renal insufficiency—thereby significantly improving patients’ quality of life.
From the information released at the launch event of the New Guidelines, we can see that:
1. The original intention behind lowering the threshold was to alert individuals at risk of hypertension;
2. Shift the focus of hypertension treatment to an earlier stage, aiming to reduce the costs of treating subsequent complications by increasing upfront expenditures;
3. Newly enrolled participants shall receive lifestyle interventions or pharmacological treatment based on individual circumstances.
If the new standards are adopted, they will have a certain impact on patients, relevant enterprises, and the market.
The New Guidelines have updated the classification criteria for hypertension, in addition to the diagnostic indicators.
In addition to classifying hypertension into three grades, the 2018 guidelines did not classify blood pressure in the range of 130–139/80–89 mmHg as hypertension, but rather categorized it as high-normal. The New Guidelines reclassify the high-normal range as Grade 1 hypertension, with all higher blood pressure values uniformly classified as Grade 2 hypertension, thereby further simplifying the diagnostic criteria.
In other words, the *New Guidelines* focus on the population previously classified as having high-normal values.
According to data released in the New Guidelines, 23.2% of adults aged 18 and above in China have high-normal blood pressure, corresponding to an estimated total of nearly 243 million people. This population primarily consists of young and middle-aged adults aged 18–54 years. A long-term study led by Beijing Anzhen Hospital showed that 65% of young and middle-aged individuals with high-normal blood pressure progressed to hypertension (≥140/90 mmHg) within 15 years. Their risk of cardiovascular disease was 2.01 times higher than that of individuals whose blood pressure remained below 130/80 mmHg. Even if blood pressure remained within the range of 130–139/80–89 mmHg over the 15-year period, the disease risk still increased by a factor of 1.28.
The purpose of adjusting the standards is precisely to protect the health of this population of nearly 243 million people.
Hypertension is a chronic disease, requiring patients to undergo regular blood pressure monitoring in their daily lives. The establishment of new standards has added more than 200 million potential target customers for related industries, further expanding the electronic blood pressure monitor market. This is also the reason behind the surge in stock prices of companies such as Cofoe Medical and Yuwell Medical.
Compared with traditional mercury sphygmomanometers, electronic blood pressure monitors offer advantages such as being pollution-free, easy to operate, and capable of data storage, making them more suitable for patient use in home settings. The electronic blood pressure monitor market is experiencing rapid growth. According to data from a report by the Zhongyan Puhua Research Institute, China’s production volume of electronic blood pressure monitors has maintained high-speed growth in recent years, with an annual growth rate exceeding 25% over the past four years.
Yuwell Medical, a well-known domestic brand of blood pressure monitors, also mentioned in its 2021 annual report that the year-on-year growth rate of its electronic blood pressure monitor products exceeded 35% during the reporting period. As a cornerstone business product of the company, it is still in a stage of rapid growth. Yuwell Medical also revealed in the annual report that it is developing multiple new models of electronic blood pressure monitors to achieve more functions and enhance product competitiveness, while iteratively upgrading existing products.
In addition to Yuwell, Andon Health, which gained significant prominence during the pandemic, and Lifesense Medical, which specializes in home healthcare electronic products, have also entered this sector. Andon Health’s blood pressure monitors have obtained UKCA certification in the United Kingdom, FDA clearance in the United States, and CE marking in the European Union. Lifesense’s electronic blood pressure monitors have passed FDA review and received 510(k) clearance.
Under the new standards, the target customer base would expand from 245 million to 500 million, potentially making electronic blood pressure monitors a household-essential medical device, much like thermometers. Only with the widespread adoption of electronic blood pressure monitors in homes can we hope to achieve early detection, diagnosis, and treatment of hypertension.
The lowering of diagnostic criteria signifies a shift toward earlier intervention in hypertension management, which aligns with the classification of high-normal blood pressure under current national standards. Both approaches share the same beneficial intent: to serve as a warning and reminder for this population.
“The New Guidelines” provide clear, categorized guidance for this population and expand on non-pharmacological interventions, rather than resorting indiscriminately to drug therapy whenever target values are not met. Lifestyle intervention is also a critical component of treatment, with chronic disease management and digital therapeutics playing significant roles in this context.
In the New Guidelines, patients with blood pressure ≥140/90 mmHg, as well as those with blood pressure in the range of 130–139/80–89 mmHg accompanied by clinical comorbidities, target organ damage, or ≥3 cardiovascular risk factors, are classified as high-risk; individuals with blood pressure solely in the 130–139/80–89 mmHg range and without any other qualifying criteria are classified as non-high-risk.
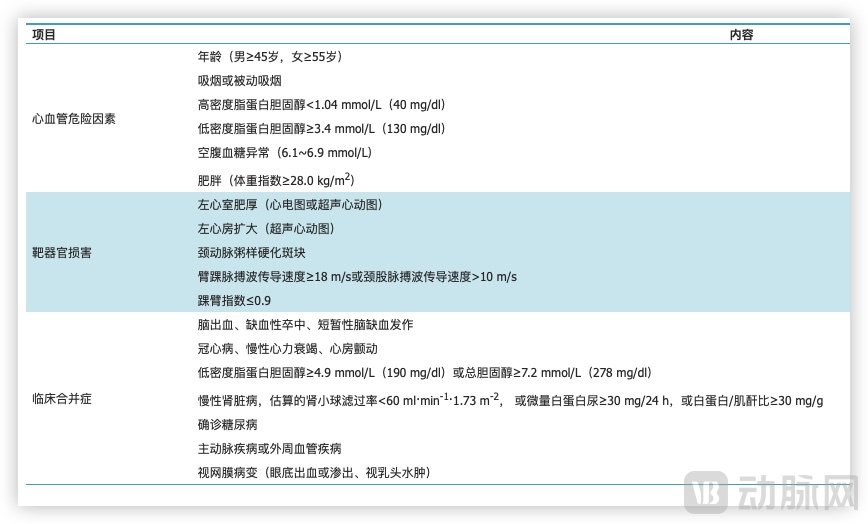
Key Factors for Assessing High Risk in Hypertensive Patients, Source: "New Guidelines"
For non-high-risk patients, the New Guidelines recommend a 3- to 6-month period of lifestyle intervention; pharmacological therapy should be initiated only if blood pressure targets are not achieved thereafter.
Lifestyle interventions encompass dietary modifications, exercise programs, stress management, weight reduction, smoking cessation and alcohol moderation, as well as comprehensive lifestyle interventions. From another perspective, aspects that were previously easily overlooked by patients are now being emphasized. This implies that chronic disease management and digital therapeutics will play a significant role in this field in the future.
In the past, chronic disease management faced a significant challenge: its approach relied on altering individuals’ cognition to modify their behavior, thereby promoting lifestyle changes. While this was not problematic for diagnosed patients, it proved far more difficult for suboptimal health populations, such as those with high-normal blood pressure. Individuals in these groups generally do not perceive themselves as ill, leading them to avoid medical consultation and resist making necessary changes.
“The New Guidelines” have lowered the diagnostic threshold while also providing a 3–6-month grace period. Individuals who return to normal blood pressure levels through lifestyle interventions during this period are still considered part of the normal population; otherwise, they will progress to pharmacological treatment and be formally diagnosed with hypertension. With such official endorsement, companies offering related services will find it easier to conduct patient education, thereby facilitating the practical implementation of their services.
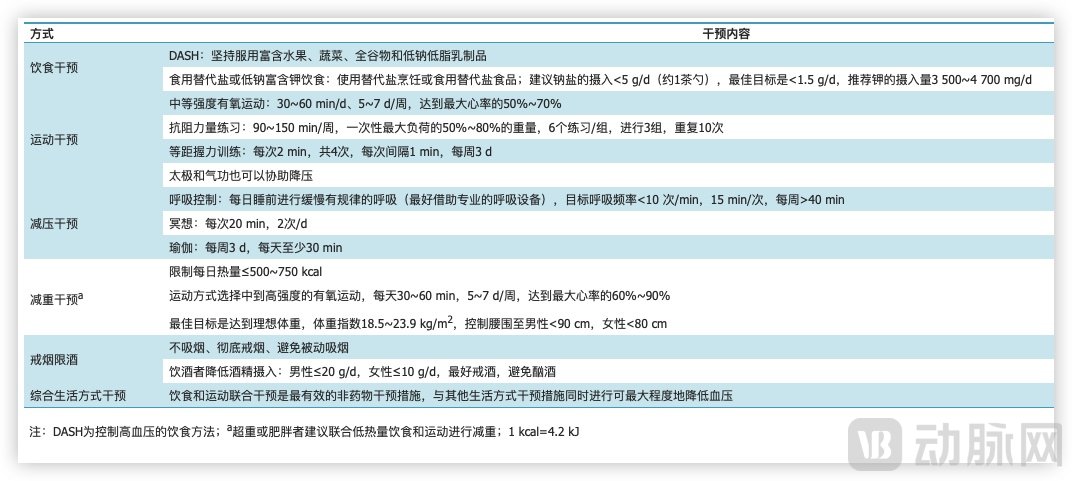
Lifestyle Intervention Content for Non-High-Risk Patients, Source: "New Guidelines"
Furthermore, just as digital therapeutics for diabetes have spurred the development of continuous glucose monitoring (CGM), chronic disease management for hypertension may similarly drive the growth of the ambulatory blood pressure monitoring market in the future.
Ambulatory Blood Pressure Monitoring (ABPM) is the “gold standard” for diagnosing hypertension. Patients are required to wear a blood pressure monitoring device that measures blood pressure every 15–20 minutes during the day and every 30 minutes at night, thereby providing comprehensive ambulatory blood pressure data to facilitate physician diagnosis.
It is precisely for this reason that some manufacturers have begun to incorporate the concept of ambulatory blood pressure monitoring (ABPM) into home electronic blood pressure monitors. Through functional upgrades and iterations, as well as optimization of device size, these devices now enable patients to perform a certain degree of ambulatory blood pressure monitoring at home.
Beyond functionality, ease of use is another key area where manufacturers are focusing their efforts. Compared to continuous glucose monitoring (CGM) systems, which are nearly imperceptible during use, home electronic blood pressure monitors still fall short in wearing comfort, despite ongoing optimizations to integrate the main unit and cuff into a single design. Consequently, many manufacturers are pinning their hopes on wearable devices. The “Guiding Principles for Registration Review of Remote Monitoring Systems (Draft for Comment),” released by the National Medical Products Administration (NMPA) in late August, also reflects this policy stance—wearable medical devices are expected to play an increasingly important role in healthcare in the future.
With technological advancements, wearable devices have made significant progress. From heart rate to ECG, and from blood oxygen to blood pressure, wearables can now continuously monitor vital signs with medical-grade precision—signals that play a critical role in the diagnosis and treatment of diseases.
In recent years, companies such as Huawei, Samsung, Huami, Kangkang Blood Pressure, and Yanhe Intelligence have successively launched smartwatches with blood pressure monitoring capabilities, ranging from tech giants to startups. Compared to traditional upper-arm and wrist blood pressure monitors, watch-form-factor devices offer superior wearing comfort, achieving a virtually unobtrusive user experience.
Blood pressure monitoring via smartwatches is a highly challenging technology. To ensure a certain level of accuracy, it is necessary not only to monitor the frequency of pulse wave oscillations but also to collect and comprehensively analyze structural and morphological information of the pulse waves. External factors such as the wearer’s skin tone, skin condition, movements, and behaviors can all affect the results. Due to these technical barriers, blood pressure monitoring remains a blue ocean segment within the wearable device market.
In the future, as the target audience expands, market demand may experience explosive growth, and wearable devices in the field of blood pressure monitoring may become more widely adopted alongside the implementation of digital therapeutics.
“The New Guidelines” not only recommend lifestyle interventions for all patients with hypertension, but also propose that drug therapy should be initiated immediately for patients with blood pressure values ≥140/90 mmHg, which is consistent with current diagnostic criteria.
The aforementioned population of over 200 million does not necessarily require pharmacological intervention, and the antihypertensive drug market itself faces numerous pressing issues that need to be addressed.
From a business model perspective, antihypertensive drugs boast a robust commercial framework—characterized by large scale and long duration.
According to Frost & Sullivan data, China already had 326 million hypertension patients in 2020, with the incidence rate of hypertension continuing to rise in recent years and the patient population steadily increasing. Furthermore, the condition can be well controlled as long as patients adhere to long-term medication. This implies that hypertension patients require an extremely prolonged course of treatment.
With these two major conditions as support, antihypertensive drugs should be a golden track. As early as 1996, Novartis' valsartan was approved for marketing and reached sales of $6 billion in 2010. Since then, the patent has expired, and although Novartis has developed various valsartan combination preparations based on valsartan, it is difficult to reach the previous peak again.
Currently, the main types of antihypertensive drugs include calcium channel blockers, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, diuretics, beta-blockers, and angiotensin receptor-neprilysin inhibitors. However, most of these “legacy” drugs have passed their patent protection periods, and the market is dominated by numerous generic drug manufacturers.
According to data from China Research Network, under the diagnostic criterion of 140/90 mmHg, the market size of antihypertensive drugs in China was approximately RMB 95.6 billion in 2020, representing a year-on-year growth of 8%. Based on this trend, the market size is projected to reach RMB 111.5 billion in 2022. Following the adjustment of diagnostic criteria, the antihypertensive drug market is expected to expand further.
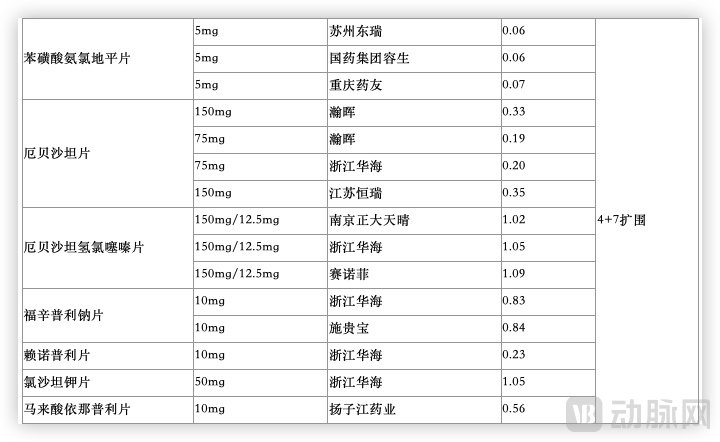
Price List of Amlodipine Besylate Tablets Selected in Centralized Procurement, with Data Sourced from Procurement Results
However, following volume-based procurement (VBP), the prices of antihypertensive drugs have plummeted to rock-bottom levels. For instance, after VBP, each tablet of valsartan, a commonly used antihypertensive, costs only RMB 0.1, while amlodipine tablets have dropped to as low as RMB 0.07 per tablet. Such extremely low drug prices make it difficult to assess how much additional performance growth this favorable policy can bring to many generic drug manufacturers.
For innovative drugs, a relaxation of diagnostic criteria may create some room for growth. However, this is predicated on the drug achieving genuine innovation, demonstrating significant advantages in either efficacy or safety compared to existing therapies. Otherwise, breaking through in a market saturated with rock-bottom-priced generics would be an immensely challenging endeavor.
Although there have been no breakthrough R&D advancements in the field of antihypertensive drugs in recent years, many companies continue to invest in this area. At the beginning of this year, Huahai Pharmaceutical announced that its Metoprolol Succinate Sustained-release Tablets, used for the treatment of hypertension, had received review and approval from the U.S. FDA. Salubris also issued an announcement stating that its New Drug Application (NDA) for SAL0107 (Allisartan Isoproxil and Amlodipine Tablets), filed under Category 2.3 of new drugs, had been accepted by the National Medical Products Administration (NMPA). Upon market launch, this product will create strategic synergy with Salubris’s already marketed Category 1.1 antihypertensive drug, Allisartan Isoproxil Tablets (brand name: Xinlitan), further enriching the company’s innovative product pipeline in the cardiovascular field and covering a broader population of patients with hypertension.
It is evident that the original intention behind the release of the “New Guidelines” was to target the 243 million individuals with high-normal blood pressure, aiming to raise their awareness. During the dissemination process, the lowering of diagnostic criteria sparked significant controversy; fortunately, the authorities promptly issued an official announcement, thereby preventing further misunderstanding. Nevertheless, this group of 243 million people remains worthy of close attention.
Returning to the diagnostic criteria that have sparked the most debate, numerical values are not the sole target of treatment, nor is hypertension management as simple as “rolling up your sleeve, measuring your blood pressure, and taking medication.” How can we encourage these 243 million individuals to pay greater attention to their own health? In light of their actual conditions, how should we design evaluation and management systems? Establishing a multidimensional cardiovascular health management system based on comprehensive interventions remains a key issue that the industry must continue to explore.