GT Medical Technologies Secures $45M Series C Funding for GammaTile, the Only FDA-Approved Radiotherapy for Glioblastoma in Nearly a Decade

GT Medical Technologies
Brain Tumor Targeted Therapy Developer
Recently, GT Medical Technologies (hereinafter referred to as “GT”) announced the completion of a $45 million Series C financing round led by Gilde Healthcare Partners, with participation from existing investors. It was disclosed that the proceeds from this round will be used to enroll more patients with resectable brain tumors, expand the commercial footprint of the GammaTile therapy, and facilitate broader patient access to this advanced treatment modality.
To date, GT has completed five rounds of financing, raising a total of $74 million.
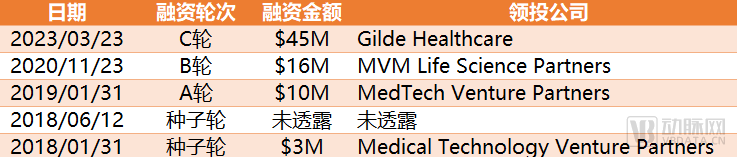
GT Financing Overview, Source: Compiled from Public Information
GT, founded in 2017 by a team of brain tumor specialists, is a medical technology company dedicated to improving the lives of patients with brain tumors. Its GammaTile Therapy is one of only a few FDA-approved treatments for glioblastoma (GBM) in the past 50 years.
GammaTile is a “small, bioabsorbable, conformal 3D collagen tile” that utilizes a cesium-131 radiation source with a half-life of 9.7 days. Its internal uniform radiation source and offset structural design help protect healthy tissue by preventing direct contact between harmful substances and the tissue, thereby helping to ensure predictable therapeutic radiation dosing. GammaTile therapy employs Surgical Targeted Radiation Therapy (STaRT) for resectable brain tumors, allowing the radiation source to be implanted immediately after tumor resection. This delivers high-intensity doses to areas most likely to harbor residual tumor cells while minimizing excessive radiation exposure to surrounding tissues.
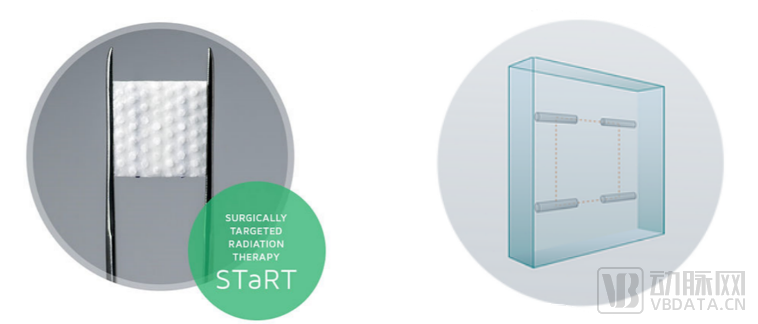
GammaTile External and Internal Design Diagrams, Source: GT Official Website
Compared with conventional treatment regimens, GammaTile therapy offers optimized improvements in four key aspects: local control, treatment duration, efficacy, and safety.
Localized Precision Control
GammaTile Therapy achieves local control through optimized dosimetry. Fifty percent of the therapeutic dose is delivered within the first 10 days post-surgery, helping to prevent the replication of residual tumor cells; 88% of the dose is delivered within 30 days; and over 95% of the dose is delivered within six weeks.
Compared with intensity-modulated radiation therapy (IMRT), GammaTile therapy’s favorable depth-dose distribution can optimize local tumor control; uniform spacing of radiation sources ensures homogeneous dose delivery, enabling more precise local tumor control while minimizing complications through optimized treatment margins.
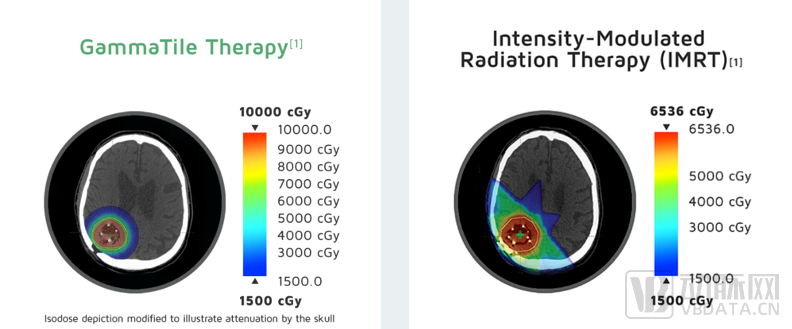
Comparison of Radiation Location and Intensity Between GammaTile Therapy and IMRT,Image source: GT official website
Shorten Treatment Time, Reduce Radiation Dose
Currently, the standard treatment for brain tumors is surgery, followed by external beam radiation therapy (EBRT). The latter typically requires patients to undergo outpatient radiation therapy five times a week for up to six weeks. In contrast, GammaTile therapy delivers high-dose-intensity treatment immediately after tumor resection, significantly reducing the time commitment required for post-resection radiation therapy in brain tumor patients.
Moreover, many patients with recurrent brain tumors have already undergone a certain degree of radiation therapy, and further radiotherapy may pose greater risks. Therefore, surgery remains their only option; however, tumor resection alone without adjuvant radiotherapy may leave behind residual tumor cells.
GammaTile Therapy delivers targeted radiation directly to the residual tumor bed, emitting a highly lethal dose to remaining cancer cells before they can replicate. This approach eliminates the need for patients to travel to hospitals or clinics for additional external beam radiation therapy, thereby significantly reducing their overall radiation exposure.
Furthermore, GammaTile does not require surgical removal after implantation and is ultimately absorbed by brain tissue. Due to the short half-life of Cs-131, 88.3% of the radiation dose is delivered within the first month after implantation, and the GammaTile radiation source becomes completely non-radioactive after 100 days.
Efficacy
In studies on the treatment of glioblastoma, comparisons of the efficacy of combining surgery with GammaTile therapy versus other treatment modalities have shown that GammaTile therapy has greater potential to improve overall survival.
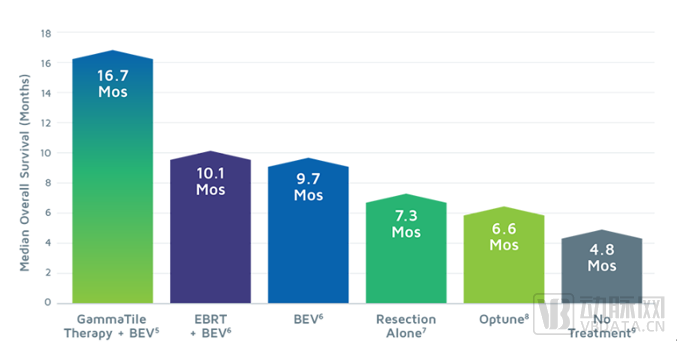
Comparison of the Effectiveness of Different Treatment Regimens,Image source: GT official website
Safety
Relevant clinical study data indicate that the incidence of radiation-related adverse events in surrounding brain tissue with GammaTile therapy is 7.6%, significantly lower than the 18%–48% observed with conventional therapies, and no Grade 4–5 adverse events associated with GammaTile therapy have been reported.
According to the "Report on the Development of Malignant Tumor Disciplines in China (2021)," the annual incidence rate of gliomas is 3–6.4 per 100,000 population, accounting for approximately 23.3% of all central nervous system tumors and 78.3% of malignant tumors. Gliomas are highly malignant, prone to recurrence, and carry a poor prognosis even after comprehensive treatment. Currently, glioblastoma has surpassed pancreatic cancer and liver cancer to become the most refractory tumor.
In 2005, the Stupp protocol became the standard of care for patients undergoing tumor resection, consisting of adjuvant temozolomide (TMZ) and external beam radiotherapy (EBRT) initiated a few weeks postoperatively. Unfortunately, patient prognosis remains poor, with little improvement in therapeutic regimens over the past few decades.
GammaTile therapy received FDA approval in 2018 for the treatment of recurrent malignant brain tumors, including recurrent high-grade gliomas, glioblastoma, meningioma, and brain metastases. In 2020, the FDA expanded this indication to include newly diagnosed malignant brain tumors. Since its availability, more than 80 hospitals across the United States have offered GammaTile to patients with brain tumors, and hundreds of patients have received this therapy.
Furthermore, GT selected hospitals that had performed 10 or more GammaTile procedures for brain tumor treatment in the past year from over 80 hospitals offering GammaTile therapy, granting them ELITE status and forming the GammaTile®ELITE Brain Tumor Centers: These ELITE centers share a common mission with GT Medical Technologies to improve the lives of patients with brain tumors.
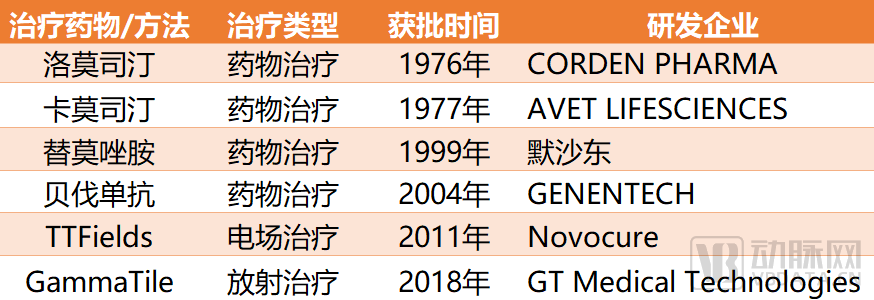
FDA-Approved Treatment Methods for GBM, Source: Compiled from Public Information
GT’s founding team consists of five experts with years of research experience in the field of radiological neuro-oncology.
Dr. David G. Brachman played a pivotal role in the development of GammaTile Therapy, serving as Co-Founder and Chief Technology Officer of GT Medical Technologies, Inc., and is the inventor of more than 25 licensed patents held by the company. Prior to the commercialization of GammaTile Therapy, Dr. Brachman worked for over 15 years at the Barrow Neurological Institute in Phoenix, Arizona, where he served as Chair and Medical Director of the Department of Radiation Oncology, as well as Co-Director of the Gamma Knife and CyberKnife programs.
The other four co-founders are all colleagues of Dr. Brachman at the Barrow Neurological Institute and the University of Arizona College of Medicine – Phoenix, namely: Dr. McBride, a radiation oncologist; Dr. Nakaji, a pioneer in neuroendoscopy; Dr. Youssef, Associate Professor in the Department of Neuroradiation Oncology at the University of Arizona; and Ms. Thomas, Research Director of Oncology Services in Arizona.
The founding team of GT Medical Technologies,Image source: GT official website
According to the latest guidelines for the diagnosis and treatment of gliomas, there are four main therapeutic modalities: surgical resection, radiation therapy, pharmacological therapy, and tumor treating fields. Surgery serves as the foundational treatment, while radiation and chemotherapy are indispensable and critical components of care. The emergence of GammaTile therapy has opened new possibilities for the treatment of brain tumor patients. As stated by Dr. John David, Assistant Professor in the Department of Radiology at the USF Health Morsani College of Medicine in Tampa, Florida, “GammaTile is a game-changer for patients with recurrent or newly diagnosed brain tumors, as it provides innovative options that were previously unavailable to them.”
Looking to the future, GT is not limiting its focus to the domestic U.S. market. Matthew Likens, CEO and President of Technology at GT, stated that the company will also allocate funds to “invest in substantial additional clinical studies to further validate safety and efficacy, expand regulatory approvals to markets outside the United States, and continue to enhance the company’s radionuclide manufacturing and supply operations.”