China's Innovation Shines Globally: 2023 Industry Report on Transcatheter Tricuspid Valve Intervention
Introduction
2023 Transcatheter Tricuspid Valve Intervention (TTVI) Industry Report, released by VCBeat.It is the only in-depth report dedicated to transcatheter tricuspid valves on the market.Tricuspid regurgitation is projected to affect over 50 million people worldwide in the future. Due to the significantly higher risks associated with surgical intervention for tricuspid regurgitation compared to mitral regurgitation, patients are often limited to conservative management. Consequently, the tricuspid valve has historically been referred to as the “forgotten valve” by the medical community.
This Report is Jointly Released byThe Team of President Wang Yan, Xiamen University Affiliated Cardiovascular HospitalThis report provides a comprehensive analysis and in-depth insights into the field of transcatheter tricuspid valve intervention from technical, clinical, and industrial perspectives. As the only industry research report in the market dedicated exclusively to tricuspid valve studies, it clearly contrasts the unique characteristics of the tricuspid valve with those of the mitral valve, highlighting the differentiated technological innovations driven by these distinctions. Furthermore, it showcases the experience of Chinese operators and the influence of China’s original technologies in this domain. Finally, we outline future trends in tricuspid valve intervention, offering valuable guidance for future research and clinical practice, with the aim of improving treatment outcomes and quality of life for patients with tricuspid valve disease worldwide.
Question
1. Should the Tricuspid Valve Really Be “Forgotten”?
2. Which Holds the Upper Hand in Tricuspid Regurgitation Treatment: Surgical or Interventional Therapy?
3. What is the global influence of China’s original innovative drugs?
4. What are the accumulated experiences and future trends in interventional tricuspid valve therapy?
Article 1: The Interventional Tricuspid Valve Market: Urgently Needs Awakening, with Significant Opportunities Amid Challenges
The tricuspid valve is one of the four cardiac valves, located between the right ventricle and the right atrium. It consists of four components: the leaflets, the annulus, the chordae tendineae, and the papillary muscles.Tricuspid Annulus (TA) is normally an asymmetric, saddle-shaped ellipsoid with two distinct components (as shown in the figure): a larger C-shaped portion corresponding to the free walls of the right atrium and right ventricle (anterior and posterior margins); and a shorter, relatively straight portion corresponding to the septal leaflet and interventricular septum (septal margin). The structural complexity of the TA lies in its dynamic nature, as it changes in shape and size under varying loading conditions.
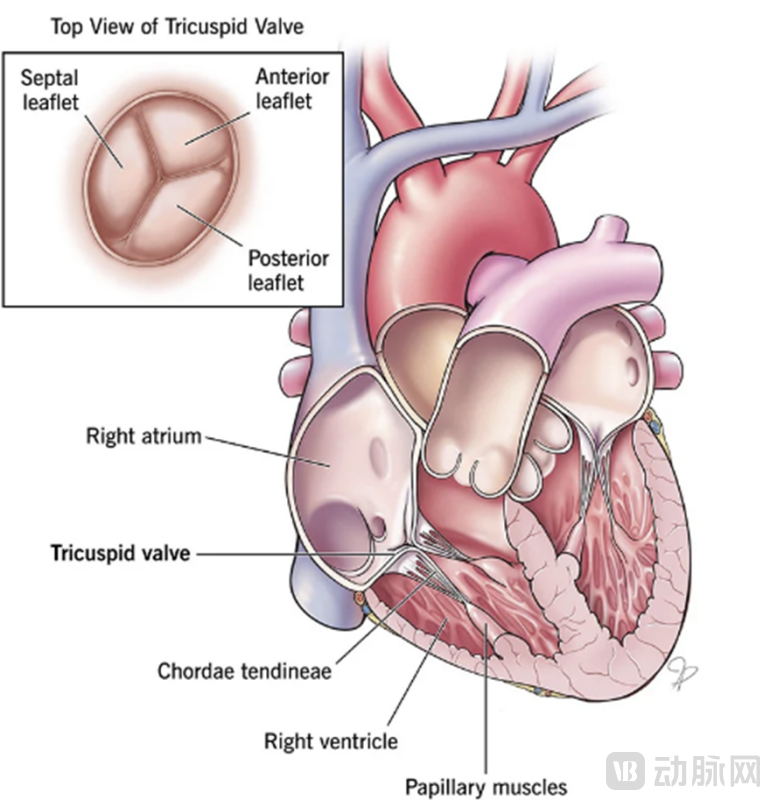
Figure 1: Overall Structure of the Tricuspid Valve
Sources: Anatomy and Physiology of the Tricuspid Valve, Cleveland Clinic, VCBeat
1.1 Urgent Call to Action: Late-Stage TR “Syndrome” Patients Face Extremely High Mortality and Should Not Be “Forgotten”
"The tricuspid valve has long been referred to as the 'forgotten valve' by the medical community."Tricuspid Valve (TV) disease, which primarily manifests in adults asTricuspid Regurgitation (TR), is the most common right-sided valvular heart disease. For decades, even moderate or greater tricuspid regurgitation (TR) was considered a benign condition, leading to undertreatment and long-term neglect. However, patients with late-stage TR “syndrome” often present with poor general health and face higher mortality rates. Coupled with the large patient population, this condition has garnered increasing attention from various clinical stakeholders in recent years.
The number of patients with tricuspid regurgitation (TR) is substantial, second only to that of patients with mitral regurgitation.According to data disclosed by Frost & Sullivan, the global number of patients with tricuspid regurgitation is second only to that of mitral regurgitation, and it is projected to affect more than 50 million people worldwide in the future. In terms of prevalence (based on the total population), the prevalence of tricuspid regurgitation exceeds 0.62%, ranking second only to mitral regurgitation and surpassing aortic stenosis. In China, the number of patients with tricuspid valve disease is also second only to those with mitral valve disease, and it is expected to affect approximately 9.9 million patients in the future. Regarding the proportion of patients (among the total number of patients with valvular heart disease), tricuspid valve disease is relatively close to mitral valve disease and accounts for a significant share. According to the "China Cardiovascular Disease Report 2019," the number of patients with valvular heart disease in China reached 36.3 million in 2019, among whom patients with aortic stenosis, mitral regurgitation, and tricuspid regurgitation accounted for 11.8%, 29.2%, and 25.1% of all valvular heart disease cases, respectively. Based on the total population, the prevalence of tricuspid regurgitation in China ranges from 0.62% to 0.7%, second only to mitral regurgitation and significantly higher than that of aortic stenosis.
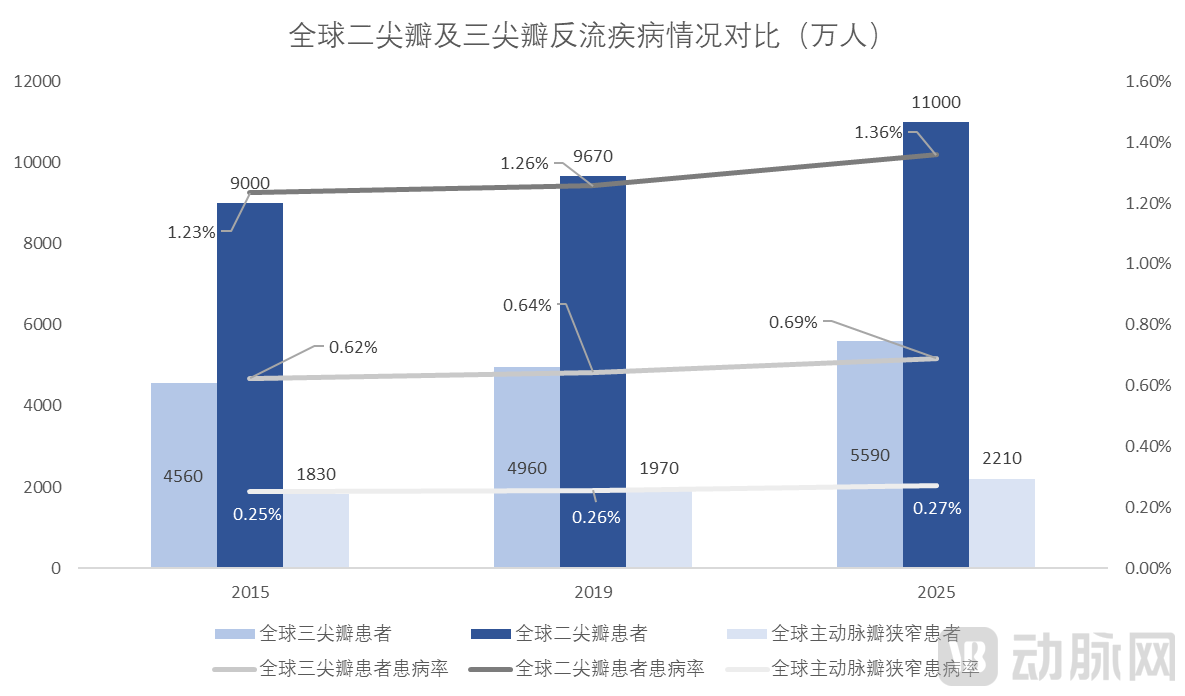
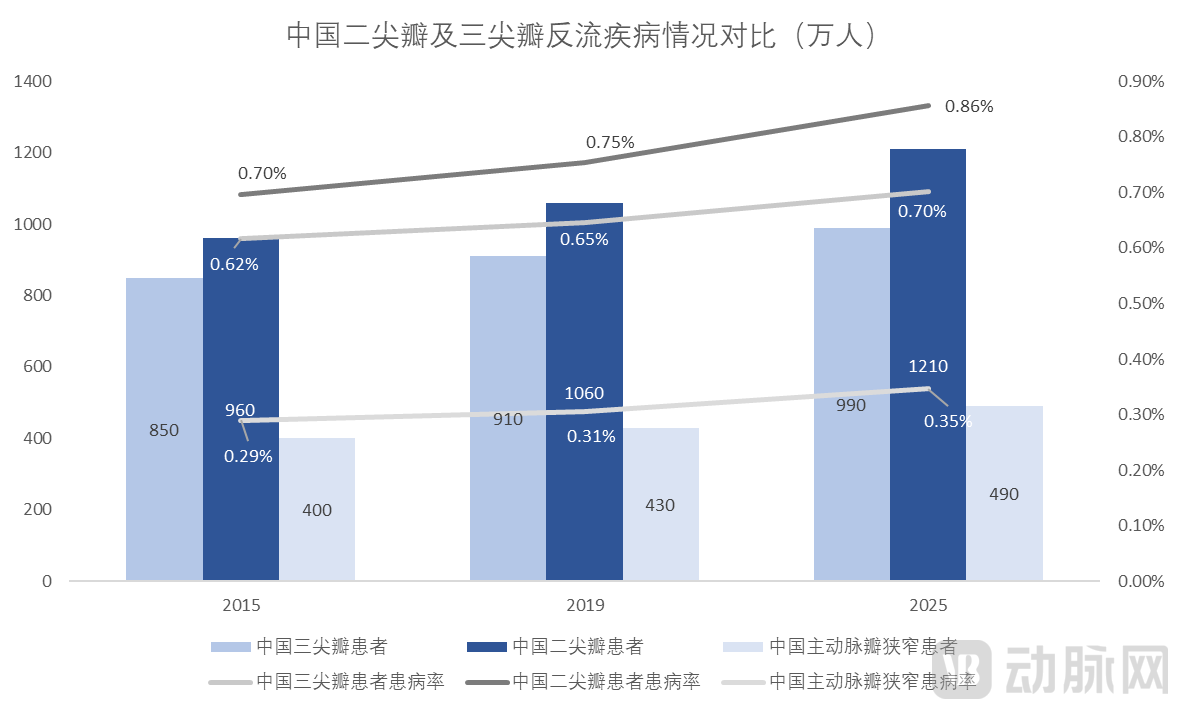
Figure 7: Comparison of the Epidemiology of Mitral and Tricuspid Regurgitation Globally and in China
Source: Frost & Sullivan, VCBeat
On the other hand, conservative management in patients with tricuspid regurgitation is associated with extremely high mortality, while surgical intervention carries the highest risk.In light of the epidemiology associated with valvular heart disease,Overall Mortality with Conservative Management Is Higher in Patients with Severe Tricuspid Regurgitation Than in Those with Severe Mitral Regurgitation. The 1- to 5-year mortality rates for patients with severe tricuspid regurgitation are approximately 35%, 42%, 50%, 58%, and 66%, respectively, reaching 86% at 10 years; for patients with severe mitral regurgitation, the 1- to 5-year mortality rates are approximately 20%, 29%, 37%, 46%, and 50%, respectively.
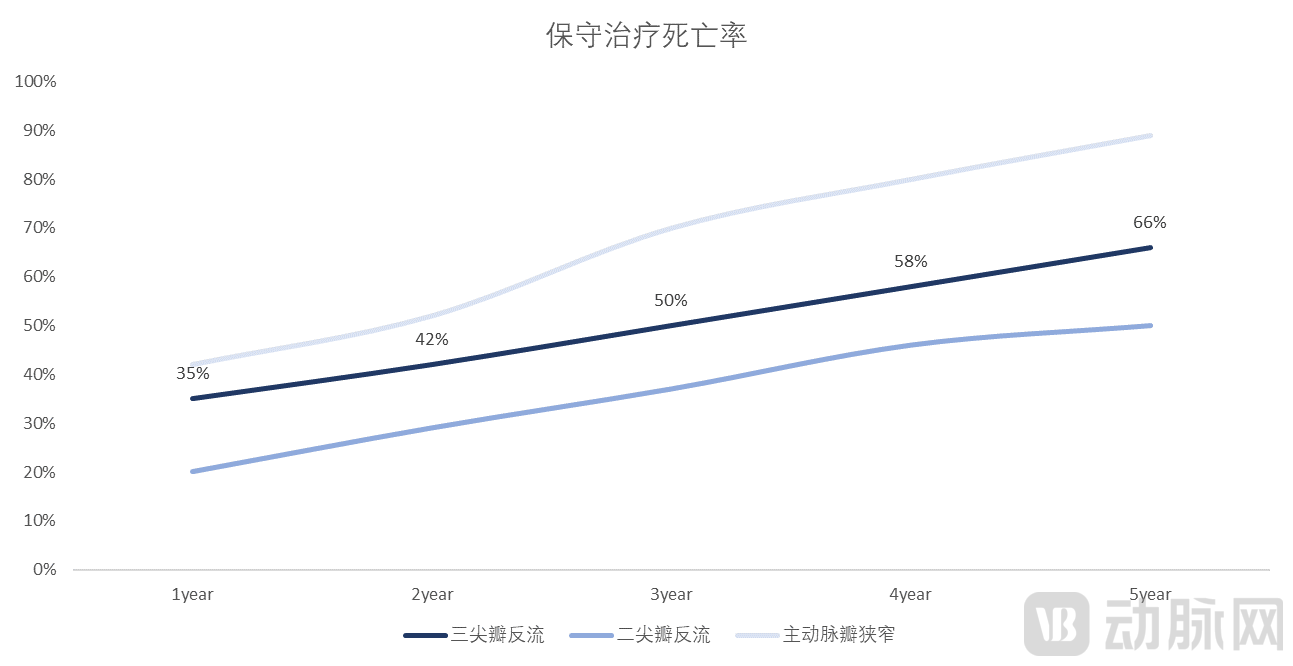
Figure 9: Extremely High Mortality Rate with Conservative Management of Tricuspid Regurgitation
Source: Excess Mortality Associated With Functional Tricuspid Regurgitation Complicating Heart Failure With Reduced Ejection Fraction, VCBeat
The surgical perioperative mortality rate in patients with tricuspid regurgitation (TR) is the highest among all valve surgeries.The perioperative mortality rate for isolated surgical tricuspid valve replacement is as high as 10.9%, and that for isolated surgical tricuspid valve repair is 8.1%. These figures are several times higher than the perioperative mortality rates for isolated surgical mitral valve repair (1.4%–2.6%), mitral valve replacement (3.8%), and aortic valve replacement (2.2%). Therefore, there is an urgent need to develop safer and more effective therapeutic approaches for tricuspid regurgitation.
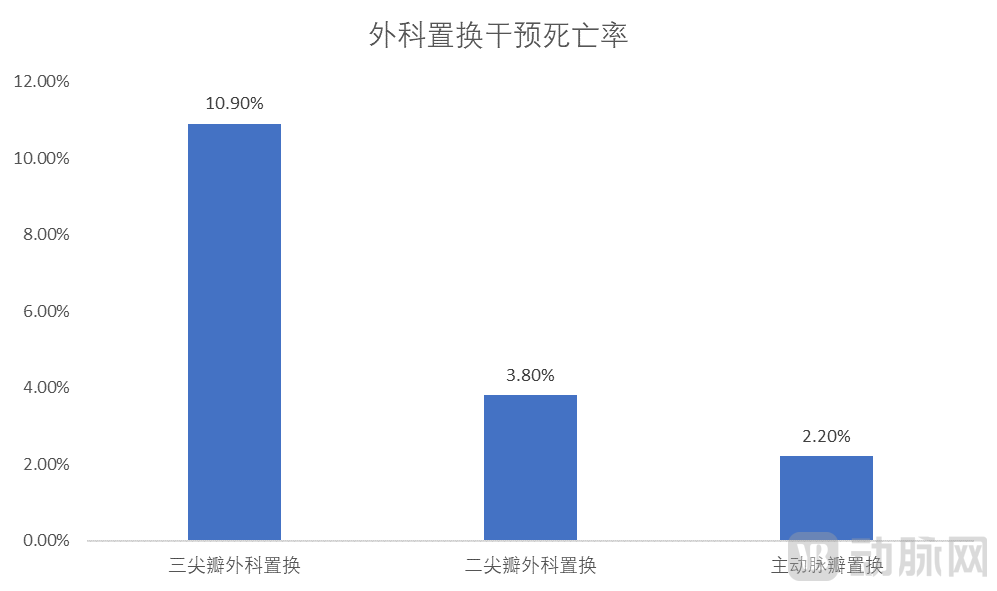
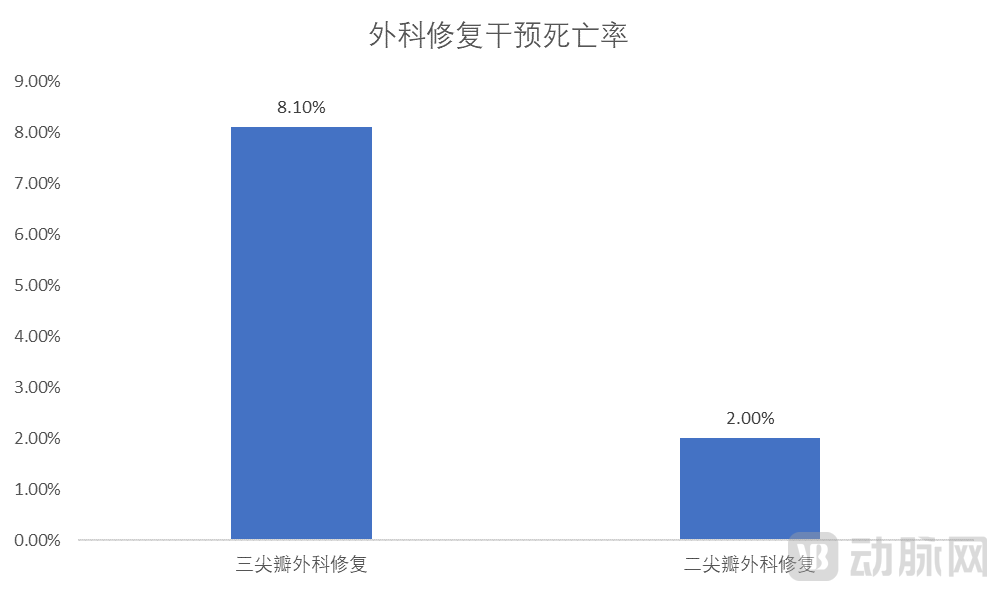
Figure 10: Mortality Rate of Surgical Intervention for Tricuspid Regurgitation Is Several Times Higher Than That for Other Valvular Heart Diseases
Source: Contemporary Trends in the Use and Outcomes of Surgical Treatment of Tricuspid Regurgitation, VCBeat
In addition to the clinical pain points of a large number of TR patients and low treatment rates, the clinical status of TR patients is extremely poor.A study based on echocardiographic data from 134,000 hospital outpatients in China showed that patients with functional tricuspid regurgitation (TR) accounted for 91.41%. The most common causes include prior left-sided valvular surgery, pulmonary hypertension, atrial fibrillation, and pacemaker implantation.
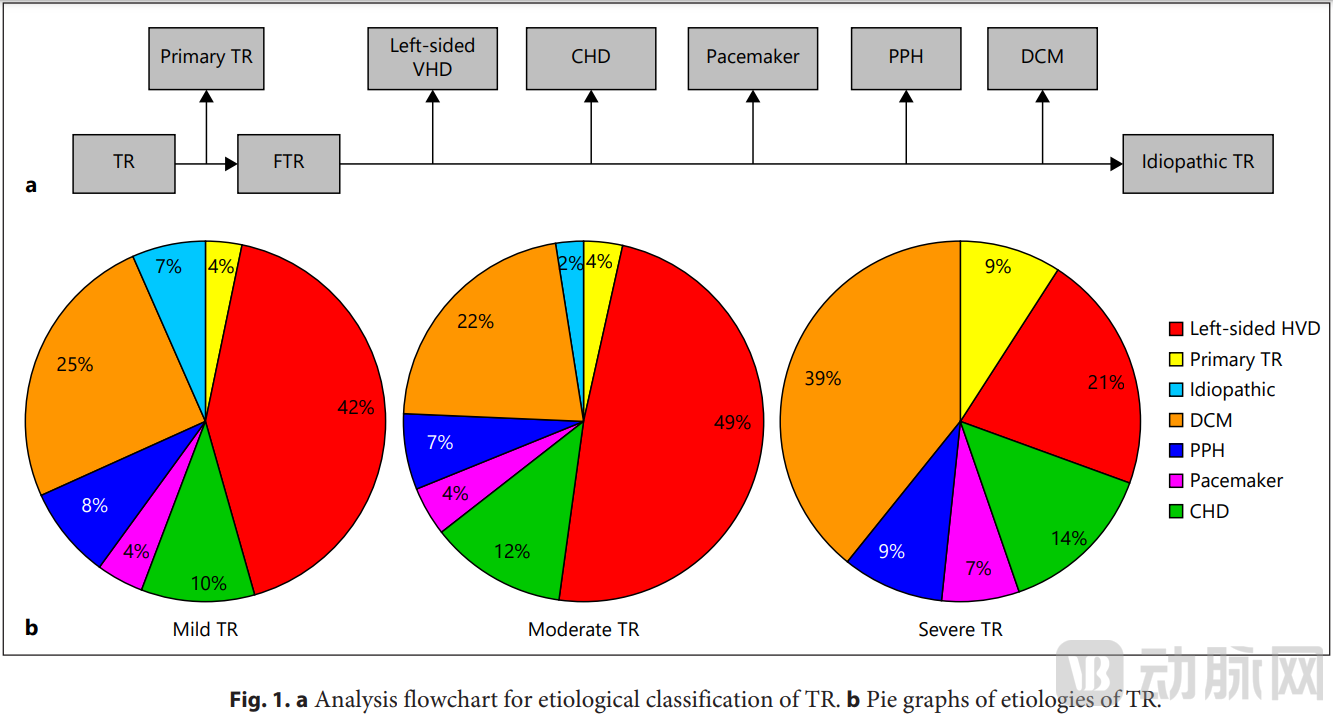
Figure 11: Echocardiographic Data from China Show the Etiology of Tricuspid Regurgitation
Source: Analyses for prevalence and outcome of tricuspid regurgitation in China: an echocardiography study of 134,874 patients, VCBeat
1.2 Strong Unmet Need: Limited Efficacy of Existing Treatments, Interventional Therapy Revitalizes Hope
Currently, therapeutic options for tricuspid regurgitation (TR) are limited. Surgical tricuspid valve repair or replacement has not demonstrated significant benefits, and pharmacological therapy yields suboptimal outcomes. Left-sided valve surgery combined with tricuspid valve repair may improve prognosis in patients with TR, underscoring the necessity of timely intervention for TR. Recent studies have shown that transcatheter tricuspid valve interventions are associated with better survival rates and lower rates of heart failure-related readmissions compared to conservative medical therapy alone, providing preliminary evidence of the efficacy of interventional treatment.
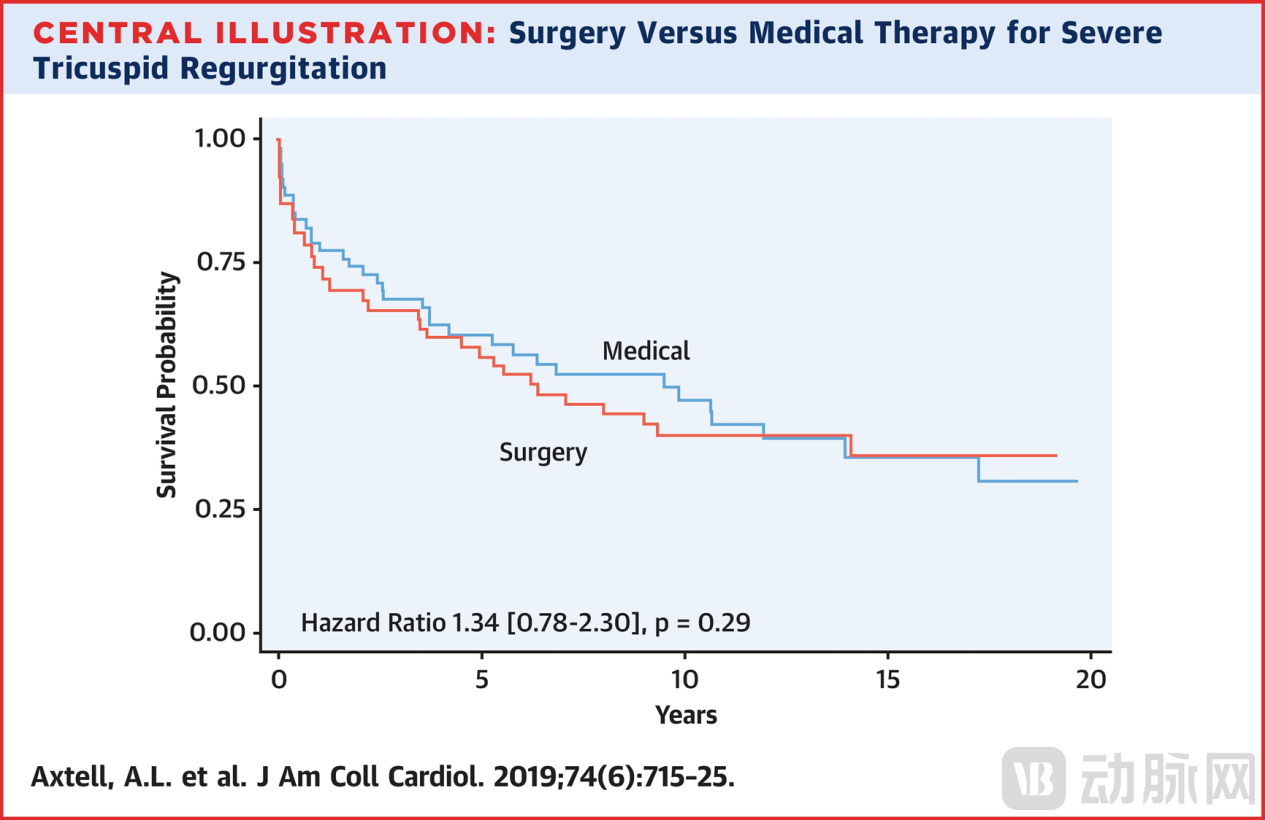
Figure 14: Surgical versus Medical Management of Severe Tricuspid Regurgitation
Source: Surgery Does Not Improve Survival in Patients With Isolated Severe Tricuspid Regurgitation, VCBeat
Transcatheter Tricuspid Valve Intervention (TTVI) is rapidly advancing.Driven by a large yet undertreated patient population and early reports demonstrating the safety and efficacy of transcatheter tricuspid valve interventions, devices for the treatment of tricuspid regurgitation (TR) have undergone rapid development.
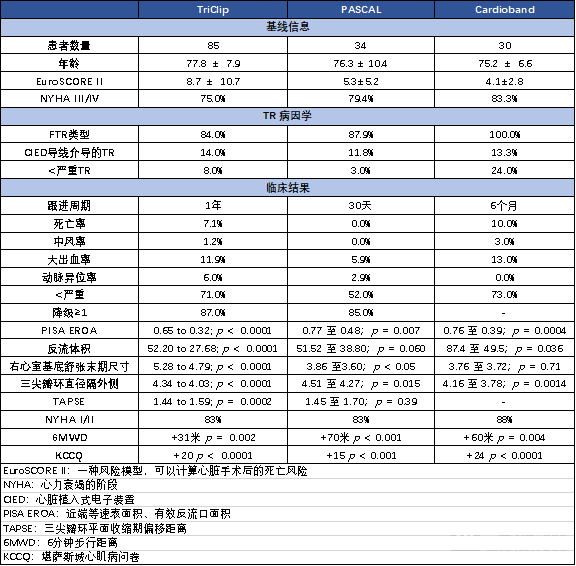
Figure 15: Summary of Available Clinical Data for Transcatheter Tricuspid Valve Repair Devices (Selected)
Source: New therapeutic approach for tricuspid regurgitation: Transcatheter tricuspid valve replacement or repair, VCBeat
1.3 Significant Market Potential: The Transcatheter Tricuspid Valve Market Is Poised for Rapid Growth
In terms of surgical volume,According to Frost & Sullivan’s forecasts, the global volume of transcatheter tricuspid valve interventions will grow from 340 cases in 2021 to 450,000 cases by 2030; meanwhile, the volume of transcatheter mitral valve interventions in China is expected to surge starting in 2023, rising from 600 cases to 200,000 cases in 2023.
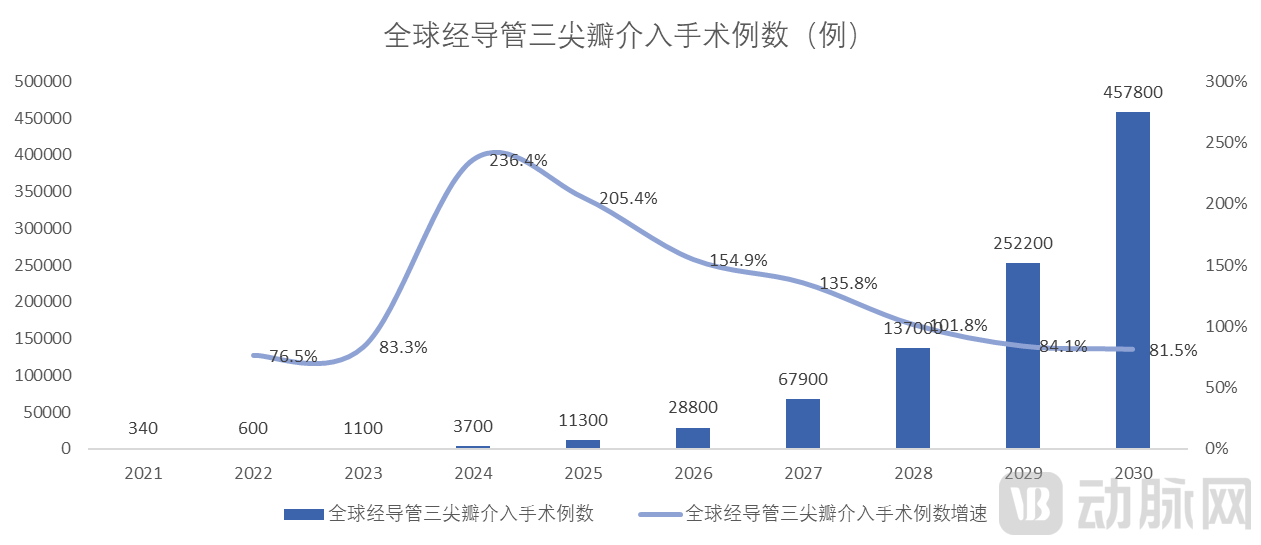
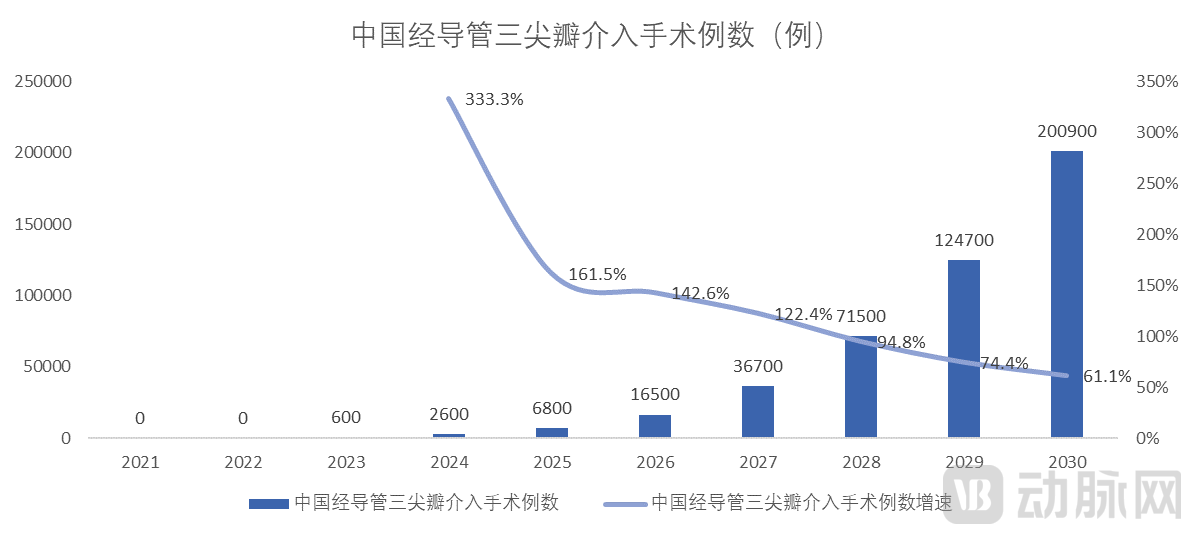
Figure 16: Global and China Tricuspid Valve Intervention Procedure Volumes
Source: Frost & Sullivan, VCBeat
In terms of market size,From 2021 to 2030, the global market size of transcatheter tricuspid valve devices is projected to grow from USD 10 million to USD 11.28 billion, with a CAGR of 118.35%. In China, the overall market for transcatheter tricuspid valve devices is expected to expand from RMB 90 million in 2023 to RMB 20.31 billion by 2030, achieving a CAGR of 118.44%. This indicates that the growth rate of China’s transcatheter tricuspid valve device market is largely consistent with the global trend, with both markets experiencing rapid expansion.
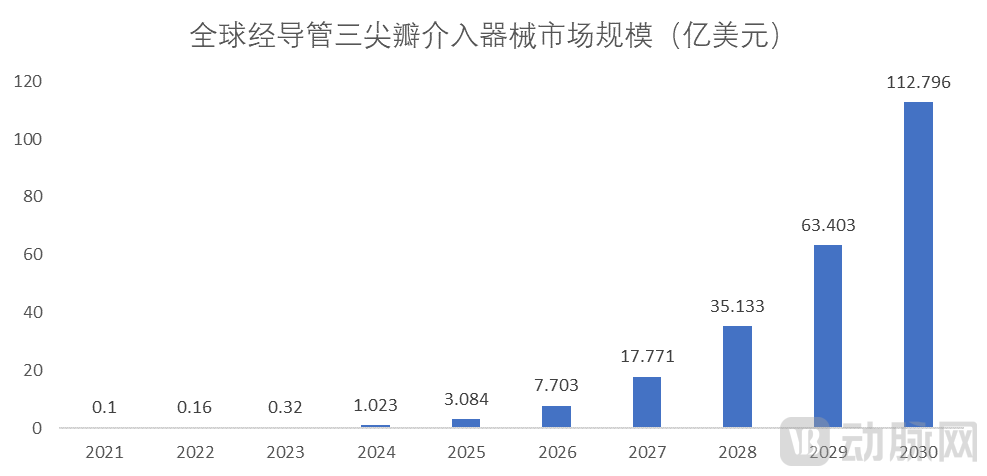
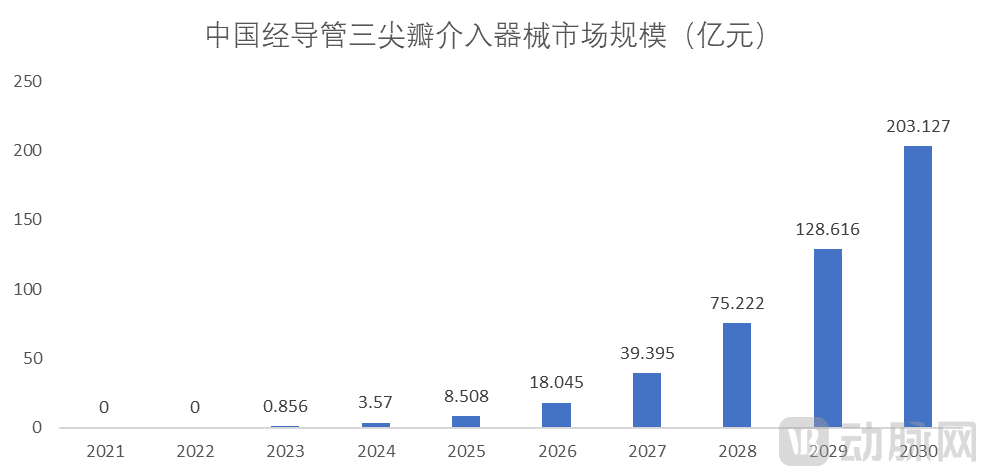
Figure 17: Market Size of Tricuspid Valve Interventional Devices Globally and in China
Source: Frost & Sullivan, VCBeat.
1.4 Major Challenge: Tricuspid Valve Anatomy and Patient Characteristics Increase Interventional Difficulty
The tricuspid valve and mitral valve differ significantly in two major aspects: anatomical structure and patient disease status, thereby posing greater challenges for transcatheter tricuspid valve interventions. First, the tricuspid valve has a more complex and fragile structure than the mitral valve. Second, tricuspid regurgitation (TR) is typically more severe. While the normal tricuspid annulus area can reach up to 9 cm², it further enlarges in cases of functional TR. Third, the complex adjacent structures of the tricuspid valve carry a potential risk of injury. Fourth, the anatomical characteristics and location of the tricuspid valve increase imaging difficulties, resulting in suboptimal image quality. Fifth, patients with secondary TR often receive intervention only at late stages, presenting with poorer overall physical condition compared to those with mitral regurgitation (MR). Furthermore, the lack of available treatment options complicates perioperative management and patient recovery.
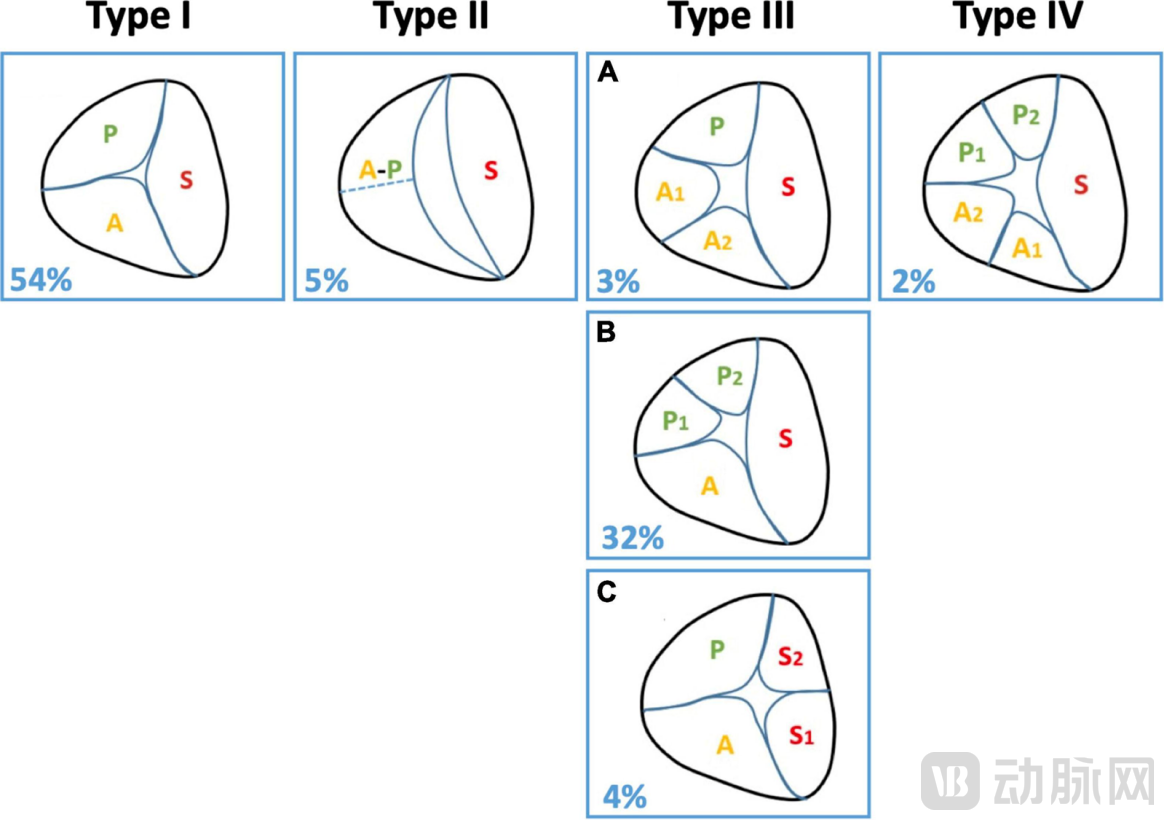
Figure 18: Marked Heterogeneity in Tricuspid Valve Leaflet Height
Source: Right ventricular function in transcatheter mitral and tricuspid valve edge-to-edge repair, VCBeat
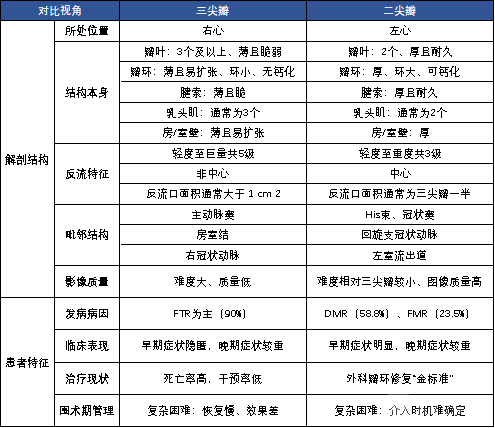
Figure 20: Comparison of Anatomical Structures of the Mitral and Tricuspid Valves and Patient Disease Conditions
Source: Challenges and future perspectives of transcatheter tricuspid valve interventions: adopt old strategies or adapt to new opportunities? et al., VCBeat
Part II: Interventional Strategies for the Tricuspid Valve: Revitalizing Patients Through Intervention, with Repair and Replacement Each Playing a Key Role
2.1 Revisiting the “Three Gates” Analytical Framework Model
We employ the “Triple Barrier” analytical framework to comprehensively and meticulously demonstrate how transcatheter tricuspid valve interventions have overcome these three major hurdles. This is achieved by comparing surgical versus transcatheter approaches, transcatheter repair versus transcatheter replacement, and the respective sub-pathways within repair and replacement strategies.The First Barrier: Comparison between Surgical and Transcatheter Procedures. Unlike mitral valve disease, for which surgical annuloplasty represents the “gold standard,” the exceedingly high mortality rate associated with surgical tricuspid valve intervention has resulted in very low treatment rates. Clinical guidelines typically recommend addressing the tricuspid valve concurrently during left-sided valve surgery. The 2021 ESC/EACTS Guidelines marked the first recommendation for transcatheter tricuspid valve therapies, emphasizing the necessity of early intervention.The Second Barrier: Comparison between Transcatheter Repair and Transcatheter Replacement. First, from the perspective of patient etiology and disease progression, we outline a personalized approach to pathway selection based on distinct patient characteristics. Furthermore, drawing on existing clinical evidence, we provide a detailed comparison of the features of transcatheter tricuspid valve repair versus replacement across three dimensions: pre-procedural, intra-procedural, and post-procedural considerations.The Third Barrier: Pathway Selection within Transcatheter Repair and Replacement. First, based on technical approaches, we categorize transcatheter repair into leaflet edge-to-edge repair and annuloplasty, and transcatheter replacement into orthotopic and heterotopic implantation. Subsequently, we present a comprehensive overview of representative products for each sub-pathway of repair and replacement, evaluated across three dimensions: product characteristics, clinical evidence, and limitations.
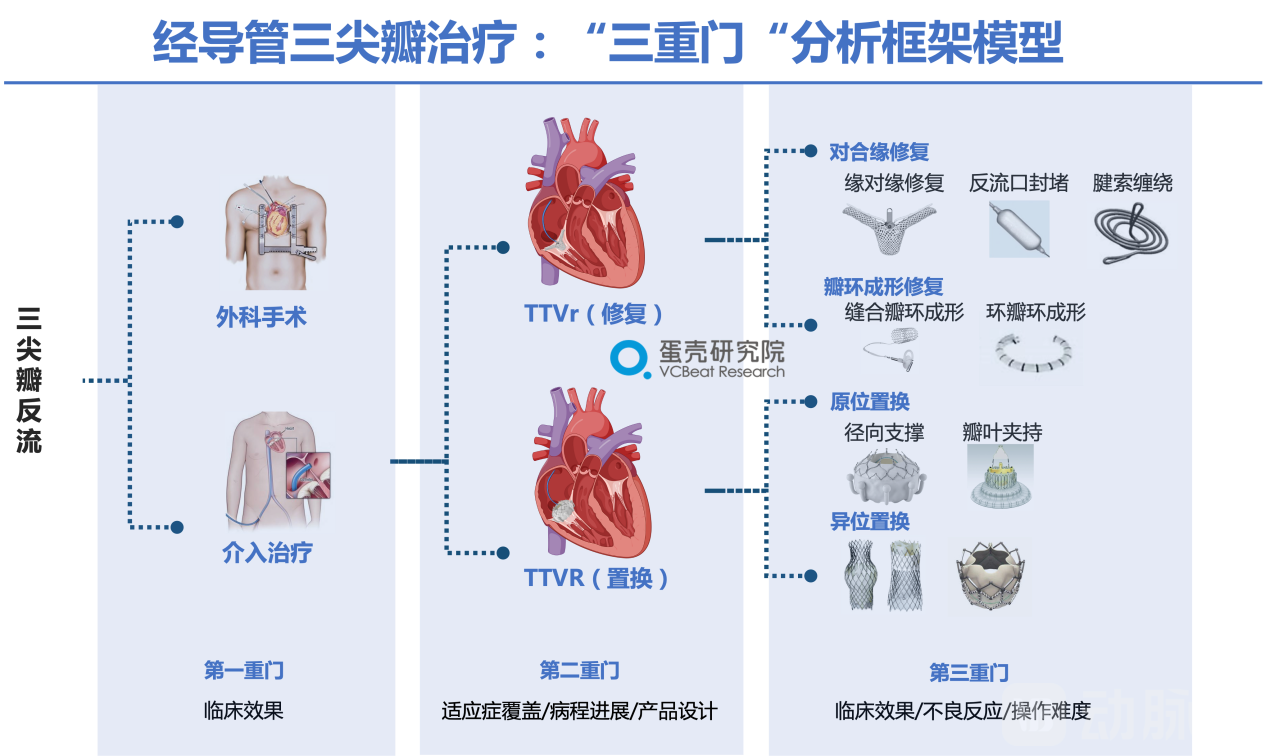
Figure 21: The “Triple Gate” Framework Model for Transcatheter Tricuspid Valve Therapy
Source: Public literature; compiled by VCBeat.
2.2 Surgery & Intervention: Limited Role for Surgical Intervention, Expanding Opportunities for Interventional Procedures
Tricuspid Valve Surgery Lacks a “Gold Standard,” While Interventional Therapy Offers New Opportunities.Unlike in the field of mitral regurgitation (MR), where surgical intervention has become the "gold standard" for treatment, clinical practice and authoritative guidelines for tricuspid regurgitation (TR) have relied almost exclusively on conservative medical management for moderate-to-severe or more severe cases. Due to the lack of targeted pharmacotherapies, high-dose diuretics are typically administered. However, the clinical efficacy of diuretic management is often limited. Furthermore, although surgical techniques for tricuspid valve repair or replacement are included in authoritative clinical guidelines, they are associated with lower treatment rates and higher mortality compared to other valvular heart diseases. Consequently, there is currently no established gold standard for either surgical or medical treatment of tricuspid regurgitation. Early positive clinical outcomes from interventional therapies have brought new opportunities to the treatment of TR.
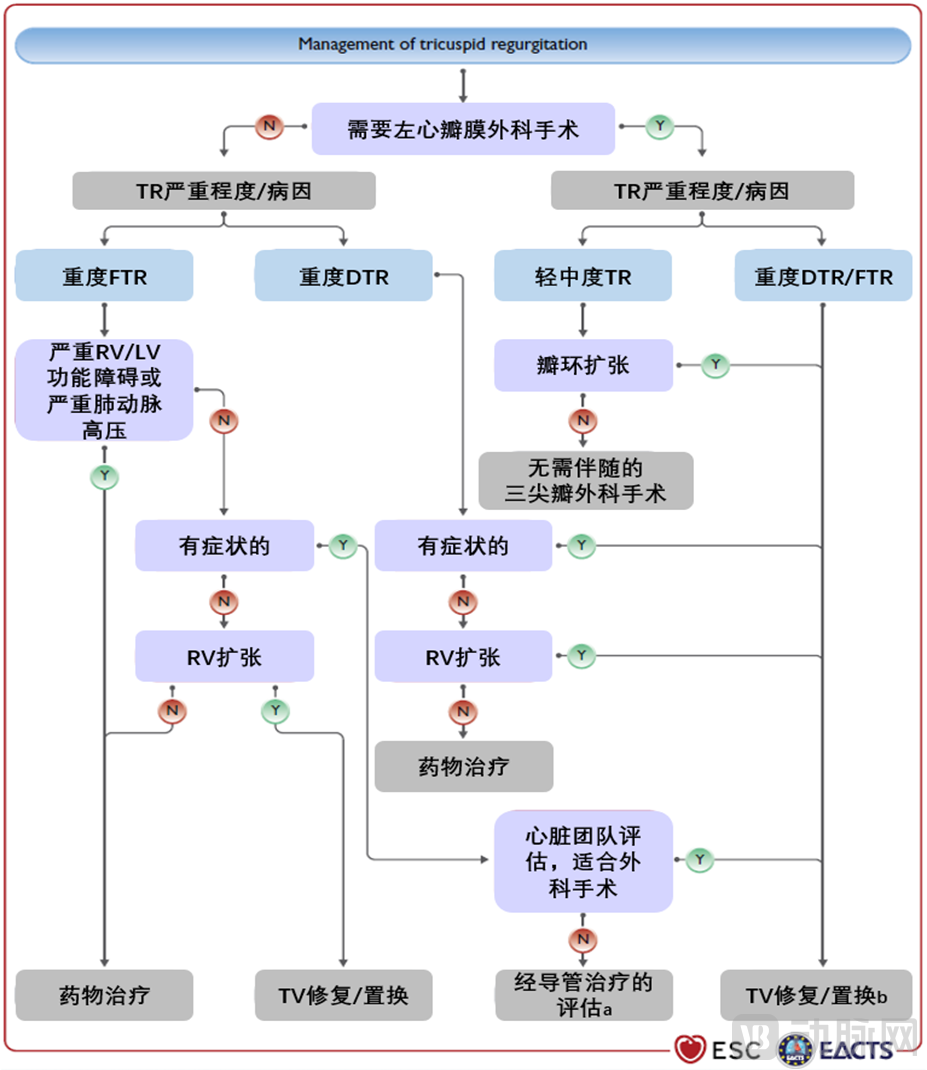
Figure 22: Schematic Diagram of Pathway Selection in TR Clinical Guidelines
Note: LV = left ventricle; RV = right ventricle; TA = tricuspid annulus; TR = tricuspid regurgitation; FTR = functional tricuspid regurgitation; DTR = degenerative tricuspid regurgitation; TV = tricuspid valve. A. The heart team with experience in treating tricuspid valve disease evaluates the anatomical suitability for transcatheter therapy, including the location of regurgitation, coaptation gap, leaflet tethering, and potential interference from pacing leads. B. Valve replacement is performed when repair is not feasible.
Source: “2021 ESC/EACTS Guidelines for the management of valvular heart disease”, VCBeat
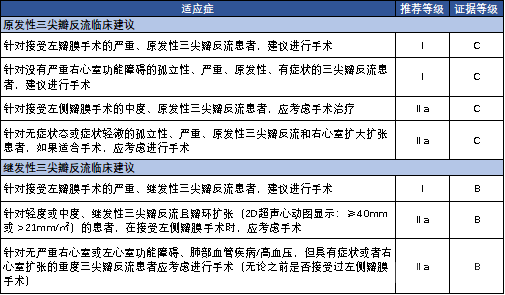
Figure 23: Guideline Recommendations for Surgical Management of Tricuspid Regurgitation
Source: “2021 ESC/EACTS Guidelines for the management of valvular heart disease”, VCBeat
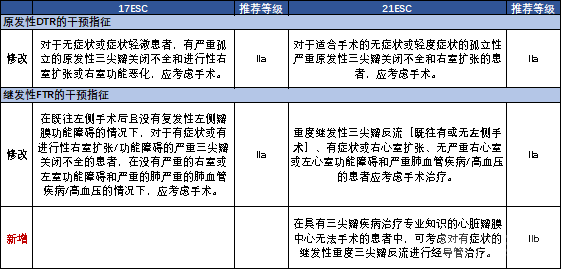
Figure 24: Comparison of Clinical Practice Guidelines for Tricuspid Regurgitation
Source: 2021 ESC/EACTS Guidelines for the Management of Valvular Heart Disease, VCBeat
2.3 Interventional Panorama: Interventional Repair & Interventional Replacement
2.3.1 Panoramic Roadmap for Transcatheter Tricuspid Valve Intervention
In recent years, transcatheter tricuspid valve intervention (TTVI) has become one of the research hotspots in the field of cardiovascular disease and has made rapid progress. In terms of technical approaches, TTVI products can be divided into two major categories: transcatheter tricuspid valve repair and transcatheter tricuspid valve replacement. Interventional repair products can be further classified intoLeaflet Coaptation Edge Repair, Annuloplastytwo categories, with interventional replacement products further divided intoIn situ replacementandHeterotopic Transplantationtwo categories (as shown in the figure below). In the technical application of TTVI, there are many products that directly adopt mitral valve treatment and draw on surgical experience. For example, TriClip, PASCAL, DragonFly-T based on edge-to-edge repair, and EVOQUE, NaviGate for valve replacement are all improvements and reuse derived from mitral valve products. Transcatheter annuloplasty mainly draws on surgical annuloplasty, thereby improving the safety of the procedure. It is worth noting thatTwo TTVI products with independent Chinese intellectual property rights, Lux-Valve and K-Clip, have entered the first tier of tricuspid valve product development, with their innovative product designs and clinical research progress attracting global attention.
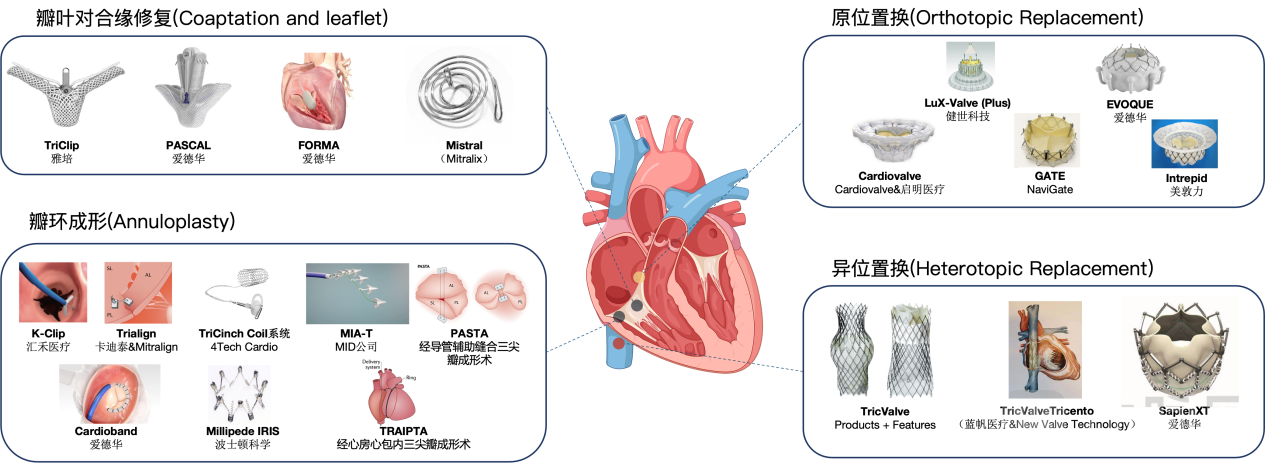
Figure 25: Panoramic Pathway Diagram of Transcatheter Tricuspid Valve Intervention
Source: Public literature, compiled by VCBeat.
2.3.2 Global R&D Progress in Transcatheter Tricuspid Valve Interventional Products
Currently, only four transcatheter tricuspid valve intervention devices have received CE certification globally, with no products yet approved for market launch by the U.S. FDA or China’s NMPA.Based on R&D experience in mitral valve repair, three CE-certified products are transcatheter tricuspid valve repair devices, includingEdge-to-Edge Repair (T-TEER) PathwayAbbott's TriClip, Edwards' PASCAL,Annuloplasty ApproachEdward's Cardioband, and anotherHeterotopic Transplantation PathwayGermany’s PF TricValve. Similar to the mitral valve, T-TEER is currently the most widely used TTVr technology globally, with the safety, availability, and ease of use of TriClip and PASCAL supported by evidence from several clinical studies. Regarding global product approvals, progress in tricuspid valve replacement devices has been relatively slow, with no approved products currently available for the orthotopic replacement approach. Among existing product pipelines, those that have entered confirmatory clinical trials include China’s LuX-Valve (Plus), independently developed by Jianshi Technology, and Edwards’ EVOQUE.
There are still multiple investigational products for repair and replacement pathways globally, with Chinese innovations emerging prominently.According to incomplete statistics from VCBeat, there are a total of 43 interventional repair and replacement products under development globally, with 24 for interventional repair and 21 for interventional replacement.Apposition Edge Technique in Interventional Repair Pathway TechnologyNeoBlazar (Duanyou Medical) has entered the pivotal clinical trial stage. Additionally, six products have entered the feasibility study stage of clinical trials, and six products are in the preclinical stage. Interventional repair pathway technologyMid-Annuloplasty TechniqueThe product that has entered the pivotal clinical trial phase is K-Clip (Huihe Medical), which has currently completed the pivotal clinical trial and entered the follow-up stage. In addition, a total of five products have entered the feasibility clinical study phase, and two products are in the preclinical stage.
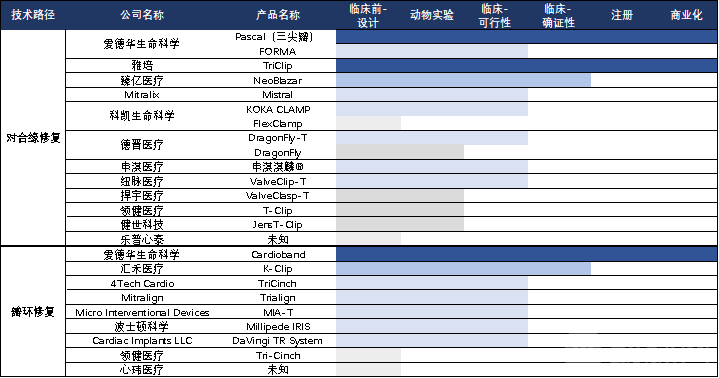
Figure 26: Domestic and International Market Launches and Pipelines of Tricuspid Valve Interventional Repair Devices
Source: Public information, compiled by VCBeat.
In Situ Replacement Technology in Interventional Replacement Pathways, LuX-Valve (Jenscare Scientific) is about to be commercialized; two products have entered confirmatory clinical trials, namely LuX-Valve Plus (Jenscare Scientific) and EVOQUE (Edwards); additionally, nine products have entered the feasibility clinical study stage; six products are in the preclinical stage. Among transcatheter replacement technologiesHeterotopic Transplantation Technique, with two products entering the feasibility clinical study phase: SpienXT (Edwards) and Tricento (New Valve & Blue Sail Medical).
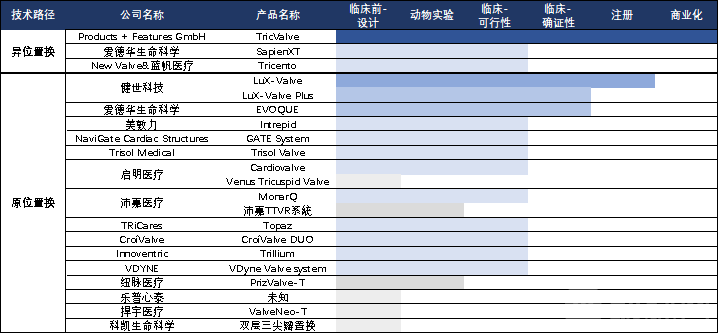
Figure 27: Domestic and International Market Launches and R&D Pipelines of Tricuspid Valve Interventional Replacement Devices
Source: Public information, compiled by VCBeat.
2.3.3 Personalized Approach Selection for Transcatheter Tricuspid Valve Intervention
Although the application of TTVI technology has developed relatively late and accumulated experience is still insufficient, a certain consensus has been formed on selecting different repair or replacement devices according to the causes and progression of tricuspid regurgitation. This report, based on existing clinical evidence and practical experience of products, fromPerspectives on Patient Etiology and Disease Progression, we analyze and discuss the selection of personalized pathways, aiming to clarify the advantages and disadvantages of various products and explore the "optimal solution" for their application. Furthermore, based on existing clinical evidence, weThree Major Perspectives: Preoperative (Patient Selection for Indicated Cases), Intraoperative (Implant Anchoring and Delivery System Operation), and Postoperative (Short- and Long-Term Efficacy, Perioperative Management), providing a detailed comparison of the characteristics of transcatheter tricuspid valve repair and transcatheter tricuspid valve replacement.
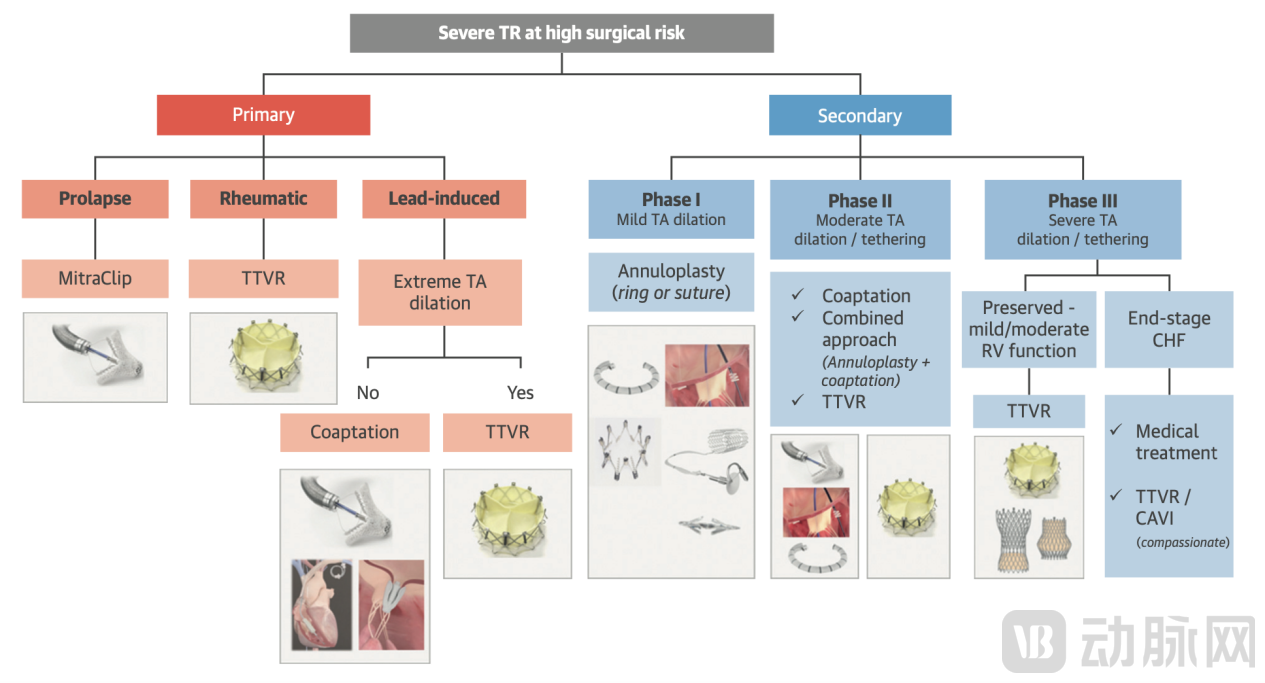
Figure 28: Personalized Selection of Transcatheter Tricuspid Valve Interventions
Source: JACC, VCBeat Research
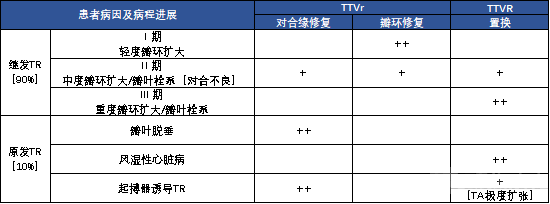
Figure 29: Theoretical Optimal Solutions for Tricuspid Valve Disease by Etiology and Disease Course: TTVr and TTVR
Source: Relevant literature, VCBeat (++ indicates preferred, + indicates optional)
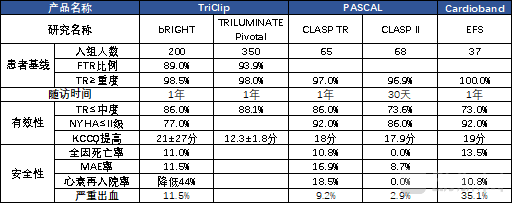
Figure 30: Clinical Progress of CE-Certified Products in 2022 Demonstrates the Efficacy of Interventional Repair for Severe Tricuspid Regurgitation
Source: Relevant literature, compiled by VCBeat
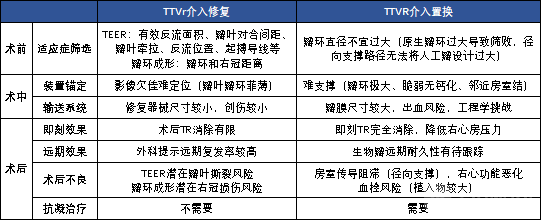
Figure 31: Transcatheter Tricuspid Valve Repair and Replacement
Source: Public literature, VCBeat.
2.4 Interventional Repair
Transcatheter tricuspid valve intervention primarily includes leaflet edge-to-edge repair (Coaptation) and annuloplasty. Leaflet edge-to-edge repairThe primary mechanisms for enhancing leaflet coaptation and reducing tricuspid regurgitation include edge-to-edge repair (T-TEER), regurgitant orifice occlusion, and chordal wrapping. T-TEER is currently the most widely adopted repair technique, with two CE-certified products available: TriClip (Abbott) and PASCAL (Edwards). The representative product for regurgitant orifice occlusion is FORMA (Edwards), which reduces regurgitation by placing a spacer at the regurgitant orifice. However, due to suboptimal long-term outcomes, the development of this product has been discontinued. Chordal wrapping is an emerging technical approach that aims to improve coaptation by capturing the tricuspid valve chordae tendineae; the representative product in this category is Mistral.(Mitralix). The product is easy to operate, is not limited by regurgitant orifice size, and requires only preoperative ultrasound imaging of the chordae tendineae; however, its long-term efficacy remains to be validated.
Transcatheter Tricuspid AnnuloplastyThis is an interventional procedure derived from surgical techniques, primarily comprising ring annuloplasty and suture annuloplasty. Representative products for ring annuloplasty include Cardioband (Edwards), Millipede IRIS (Boston Scientific), and TRAIPTA. There are numerous products under suture annuloplasty, mainly including: K-Clip (Huihe Medical), Trialign (Mitralign & Cardiotek), TriCinch (4Tech Cardio), Percutaneous Annular Suture Tricuspid Annuloplasty (PASTA), and Minimally Invasive Annuloplasty Technology (MIA) (Micro Interventional Devices). These products are primarily indicated for early-stage secondary tricuspid regurgitation; in terms of recurrence rates, ring annuloplasty demonstrates superiority over suture annuloplasty. For mid-stage secondary tricuspid regurgitation, standalone efficacy is suboptimal, and combination therapy with T-TEER may be employed. Additionally, due to the proximity of the tricuspid annulus to the His bundle and the right coronary artery ostium, post-implantation complications such as myocardial infarction, right coronary artery perforation, conduction block, and severe hemorrhage may occur.
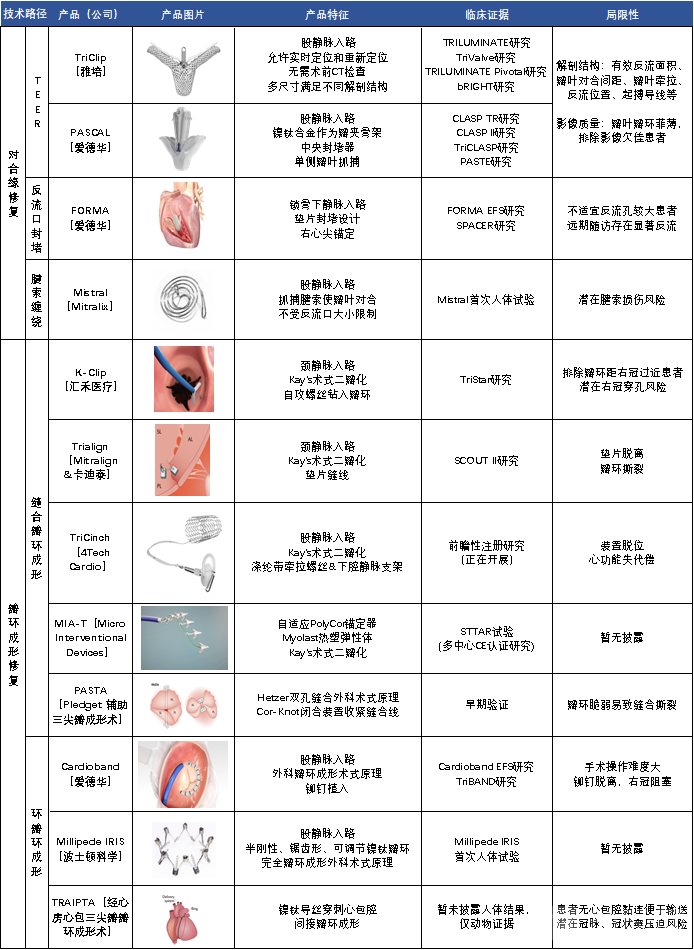
Figure 32: Overview of Features of Interventional Repair Products
Sources: Public literature, official product websites, VCBeat.
2.5 Interventional Replacement
Based on design principles, transcatheter tricuspid valve replacement products can be categorized into orthotopic replacement and heterotopic replacement. Orthotopic replacement involves positioning the prosthetic valve at the anatomical site of the native tricuspid valve to substitute its function, eliminate systolic regurgitation, reduce right atrial pressure and right ventricular preload, thereby alleviating systemic venous congestion and reversing right ventricular remodeling. Representative products include EVOQUE (Edwards), GATE (NaviGate), LuX-Valve (Plus) (Jenscare Scientific), Cardiovalve (Cardiovalve & Venus Medtech), and Intrepid (Medtronic). These products demonstrate superior efficacy compared to repair-based devices in scenarios such as excessively large effective regurgitant orifice area and coaptation gaps, significant annular dilation, severe leaflet tethering, non-central or anterior-septal commissural regurgitation, direct compression of the septal leaflet by pacemaker leads, leaflet calcification or iatrogenic injury, and tricuspid stenosis.Heterotopic TransplantationThis involves implanting artificial valves into the superior and/or inferior vena cava to reduce venous regurgitation and alleviate systemic congestion; however, it may not facilitate right ventricular reverse remodeling and functional recovery. As such, it is primarily used as a palliative adjunct to transcatheter tricuspid valve repair (TTVr) or orthotopic transcatheter tricuspid valve replacement (TTVR). Representative products include TricValve (P + F GmbH), Tricento (Lifetech Scientific & New Valve Technology), and Sapien XT (Edwards).
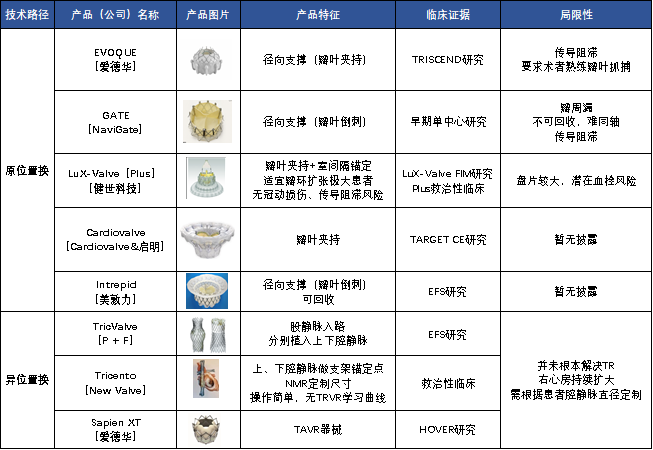
Figure 45: Overview of Product Characteristics for Interventional Replacement Devices
Sources: Public literature, official product websites, VCBeat.
Part III: Advances in Transcatheter Tricuspid Valve Interventions: Chinese Innovations Shine Globally as Diverse Approaches Compete
In 2022, significant clinical research advancements were made in global interventional tricuspid valve devices, providing further evidence to support interventional tricuspid valve therapy. Three CE-certified interventional repair products, drawing on experience from mitral valve interventions, are Abbott’s TriClip, Edwards’ PASCAL, and Cardioband. Encouragingly, China’s original tricuspid valve devices, LuX-Valve (Jenscare Scientific) and K-Clip (Huihe Medical), were showcased at PCR London Valves 2022, demonstrating the strength of Chinese innovation to the world. Meanwhile, tricuspid valve replacement, represented by LuX-Valve, has surged ahead, outpacing mitral valve developments and highlighting the leading “China speed” on the global stage. With various technological approaches competing globally, clinical results presented at major academic conferences such as PCR London Valves, ESC, ACC, and EuroPCR, as well as published in journals like JACC in 2022, have further confirmed the efficacy and safety of interventional tricuspid valve devices for treating tricuspid regurgitation (TR). In addition, multiple tricuspid valve products worldwide have achieved significant clinical progress. These include NeoBlazar (Duanyou Medical), DragonFly-T (Dejin Medical), and koka clamp (Koke Life Science) via the T-TEER approach, as well as EVOQUE (Edwards), Cardiovalve (Cardiovalve & Qiming Medical), and MonarQ (Peijia Medical & inQB8) via the orthotopic replacement approach, all of which have reported clinical advancements.
3.1 CE-Certified Products Originating from the Mitral Valve: Clinical Evidence Further Strengthened
Three CE-certified products for the treatment of tricuspid regurgitation are transcatheter tricuspid repair devices developed based on experience with mitral valve repair, among which the most widely adopted technique internationally is edge-to-edge repair (T-TEER). In 2022, presentations at major global academic conferences provided additional clinical evidence supporting the safety and efficacy of these three approved products.These include Abbott’s TriClip and Edwards Lifesciences’ PASCAL, both of which follow the transcatheter edge-to-edge repair (T-TEER) pathway and received CE marking in 2020, as well as Edwards Lifesciences’ Cardioband, which follows the annuloplasty pathway and received CE marking in 2018. The TriClip™ is a device specifically designed for T-TEER; its delivery system features a shorter guide catheter with enhanced maneuverability. The latest-generation TriClip G4 system offers four different clip sizes and an independently controllable gripper drive mode to optimize leaflet grasping. The PASCAL system has also undergone a series of developments. The newly released PASCAL Ace clip is smaller in size and has a narrower spacer compared to the first-generation PASCAL clip. Furthermore, the PASCAL Precision delivery system, which received CE marking in August 2022, improves upon the original PASCAL delivery system with enhanced performance in terms of delivery and positioning.
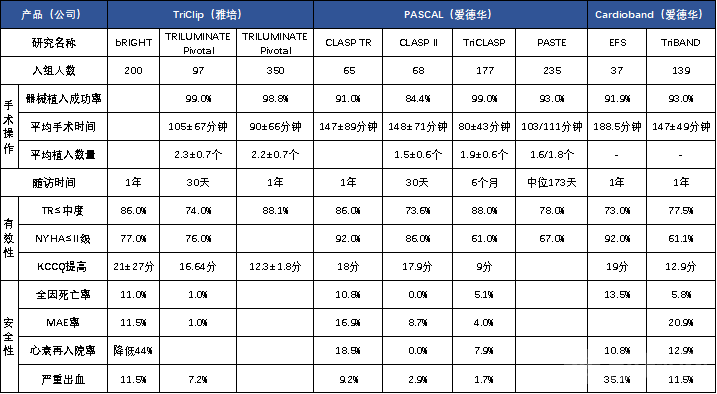
Figure 54: Summary of 2022 Research Progress on CE-Certified Products
Source: Relevant literature, compiled by VCBeat.
3.2 Chinese Innovations Shine Globally, Leading Progress in Tricuspid Valve Replacement
China’s Original Tricuspid Valve Devices, LuX-Valve and K-Clip, Make Debut at PCR London Valves 2022, Showcasing the Strength of Chinese Innovation to the World.In October 2022, the first-generation trans-right-atrial product of the LuX-Valve orthotopic replacement system (Jenscare Scientific) completed its one-year follow-up for the confirmatory clinical trial and submitted data to regulatory authorities. Commercialization is anticipated in 2023, with the potential to become the world’s first marketed orthotopic tricuspid valve replacement product.Encouragingly, the 2021 ESC/EACTS Guidelines cited the results of the first-in-human trial of the LuX-Valve, marking international recognition for this Chinese-origin transcatheter valve replacement product.In September 2022, the national multicenter confirmatory clinical trial TRAVLE II for the second-generation transjugular Lux-Valve Plus, led by Academician Ge Junbo, was officially launched. Enrollment is currently more than halfway complete (46 cases), with full enrollment expected to be finished and the comprehensive follow-up phase to begin in early 2023. From May to October 2022, the K-Clip annuloplasty system (Huihe Medical) completed its confirmatory clinical trial and has entered the follow-up phase, with commercial application expected in the near future.
Tricuspid Valve Replacement Surges Ahead, Outpacing Mitral Valve Progress; China’s Speed Leads the World Due to the Higher Risk of Left Ventricular Outflow Tract Obstruction in Mitral Valve Procedures.ReviewLVOT Obstruction Following Mitral Valve ReplacementQuestion: Although the world’s first human transcatheter mitral valve replacement (TMVR) procedure, involving the implantation of the CardiAQ valve (the predecessor to Evoque), was performed as early as 2012, most valve programs were terminated due to high mortality rates in early clinical trials. To date, only one device, the transapical Tendyne system (Abbott), has received CE marking, which it obtained in 2020. AlthoughTricuspid valve replacement also carries the risk of atrioventricular block.risks. However, unlike products such as EVOQUE (Edwards) and Intrepid (Medtronic), which are directly adapted from mitral valve devices, LuX-Valve was specifically designed for the anatomical characteristics of the tricuspid valve to mitigate this risk. Developed independently by Professor Lu Fanglin’s team at Changhai Hospital in collaboration with Jenscare Scientific, LuX-Valve employs a unique “non-radial force” design concept. It secures the valve through septal anchoring and anterior leaflet capture, thereby reducing the incidence of atrioventricular conduction block. In 2023, the Chinese-originated LuX-Valve (Jenscare Scientific) is poised to become the world’s first commercially available transcatheter tricuspid valve replacement device.Comparing the clinical enrollment progress of mitral and tricuspid valve procedures in China,We have observed that, due to the high risk of left ventricular outflow tract obstruction (LVOTO) associated with mitral valve replacement, patient enrollment for the two most advanced domestic mitral valve replacement products (Mitrafix and Mi-thos) has been slow. Out of safety considerations, strict patient screening is required; for instance, since the first human implantation of Mi-thos in 2019, only 13 cases have been reported in feasibility and registrational clinical studies. In contrast, on a global scale, the tricuspid valve LuX-Valve has completed over 250 implantations (with 159 patients enrolled in the confirmatory clinical trial from October 2020 to August 2021), and the LuX-Valve Plus has achieved more than 100 global implantations.
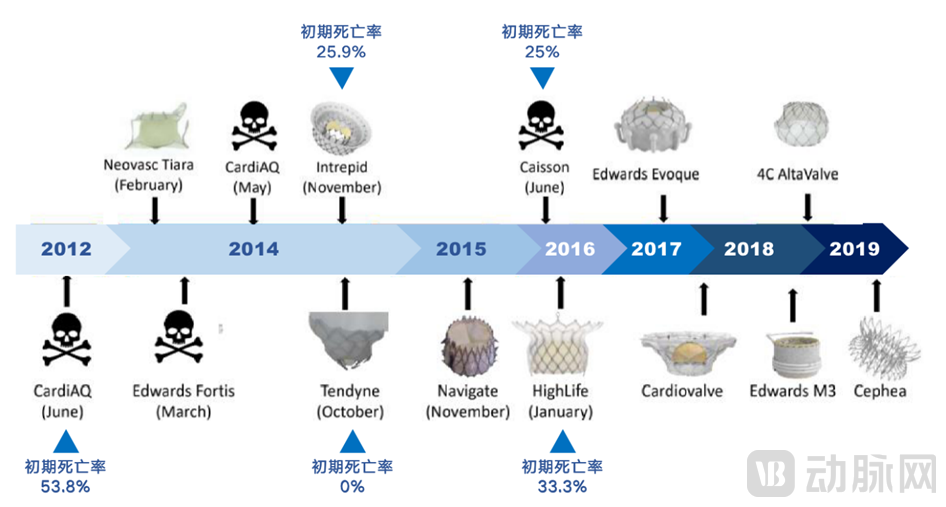
Figure 65: The R&D of Transcatheter Mitral Valve Replacement Products Is Extremely Challenging
Source: Public information, VCBeat.
3.3 Global Products Intensify Competition
In 2022, multiple tricuspid valve products achieved significant clinical advancements globally.In addition to the research progress reported at various academic conferences for CE-certified devices such as TriClip (Abbott), PASCAL (Edwards), and Cardioband (Edwards), as well as the imminent commercialization of China’s original innovations LuX-Valve (Jenscare Scientific) and K-Clip (Huihe Medical), clinical advances have also been reported for products following the T-TEER pathway, including NeoBlazar (Duanyou Medical), DragonFly-T (Dejin Medical), and koka clamp (Kokai Life Sciences), and those pursuing the orthotopic replacement pathway, such as EVOQUE (Edwards), Cardiovalve (Cardiovalve & Qiming Medical), and MonarQ (Peijia Medical & inQB8).
Part 4: The Future of Transcatheter Tricuspid Valve Intervention: Experience and Trend Outlook
The preceding sections have elaborated in detail on the necessity of transcatheter tricuspid valve intervention, the comprehensive technical pathways, and clinical progress in 2022. Although challenges remain in transcatheter tricuspid valve therapy, existing evidence has accumulated substantial clinical experience and identified multiple dimensions worthy of discussion. We anticipate that transcatheter tricuspid valve therapy will become more standardized and mature in the future, thereby benefiting a broader patient population. In the following section, we will elaborate on the accumulation of experience and future trends in transcatheter tricuspid valve therapy from seven perspectives, including the heightened necessity of transfemoral venous access for patients with tricuspid regurgitation (TR), imaging assessment and perioperative management experience, discussions on optimal timing of intervention and therapeutic endpoints, the continued strengthening of clinical evidence, and an outlook on the evolving landscape of interventional therapy.
4.1 Transvenous Approach Is More Imperative for Patients with Tricuspid Regurgitation
Compared with mitral valve disease, patients with severe tricuspid regurgitation (TR) are in much poorer condition, making the transvenous approach more critically necessary for these patients.
In the mitral valve report, we have elaborated in detail on the advantages and disadvantages of the transapical versus transfemoral approaches, proposing that the transfemoral approach will become the ultimate choice. Existing studies indicate that while the technical success rates of the transapical and transfemoral approaches are similar, the transfemoral approach is associated with lower mortality, faster postoperative recovery, and shorter hospital stays. More importantly, patients with tricuspid regurgitation (TR) generally present in worse condition than those with mitral regurgitation (MR), often seeking medical attention only at advanced stages of the disease. Consequently, they frequently exhibit severe systemic clinical manifestations and poor overall physical status, rendering them unable to tolerate the trauma associated with hybrid surgical procedures. This leads to a higher incidence of postoperative complications, including incisional bleeding due to impaired coagulation mechanisms, postoperative infections resulting from severely compromised immune function, and pulmonary complications.
4.2 Imaging Assessment Experience in Tricuspid Valve Intervention
The efficacy of transcatheter tricuspid valve intervention is largely dependent on the image quality of echocardiography.The core challenge in imaging-based identification for tricuspid valve interventions lies in the suboptimal quality of transesophageal echocardiography (TEE) images. This is attributed to the tricuspid valve’s location in the far field, its leaflets being thinner and thus more difficult to visualize than those of the mitral valve, the highly heterogeneous anatomical structure with multiple leaflets, and frequent artifacts from metallic shadows caused by prior valve replacements or pacemaker leads, all of which complicate the localization of leaflets and the annulus.
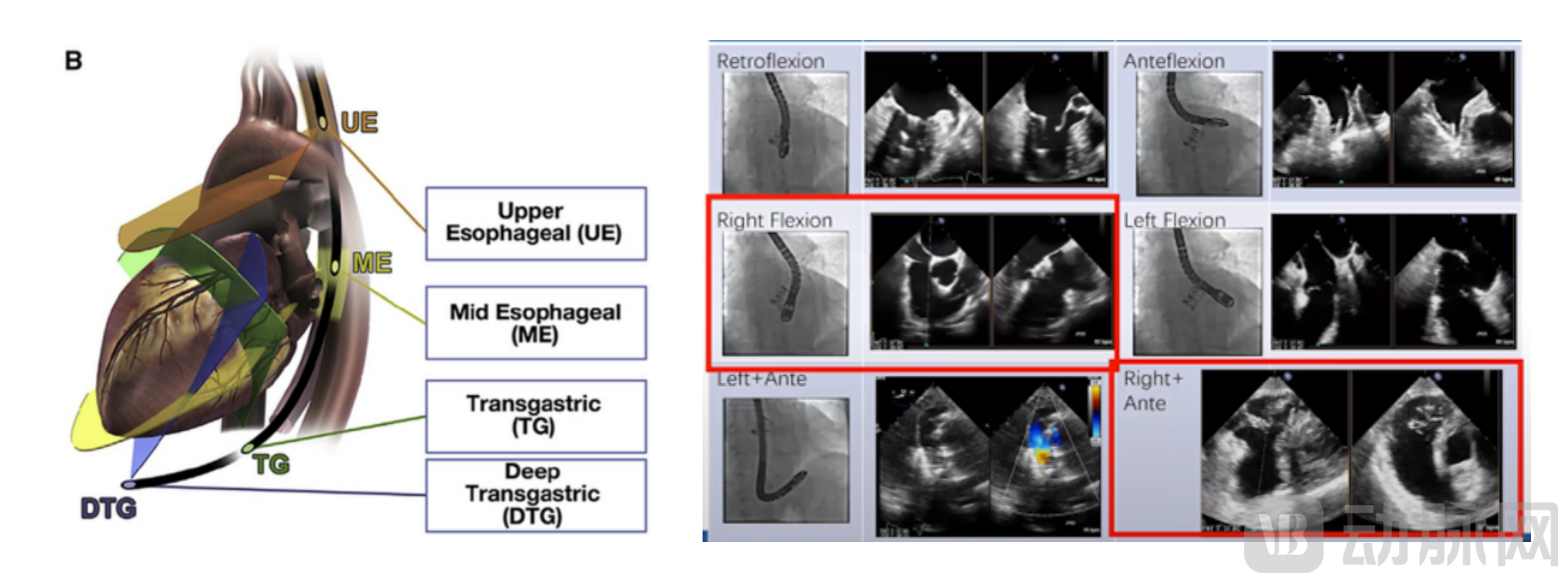
Figure 79: Key TEE Views and Critical Guiding Planes for Tricuspid Valve Identification
Sources: Guidelines for Performing a Comprehensive Transesophageal Echocardiographic Examination; Indications and Key Technical Considerations for Transcatheter Edge-to-Edge Tricuspid Valve Repair; VCBeat
4.3 Perioperative Management Experience in Tricuspid Valve Intervention
Given that patients with tricuspid regurgitation (TR) often present with complex clinical manifestations and severely compromised physical conditions, the importance of perioperative care for transcatheter tricuspid valve interventions is further highlighted. Scientifically guided nursing care facilitates postoperative recovery and improves quality of life.
First, volume management must be maintained throughout the entire perioperative period."Due to the slow recovery of the right ventricle, postoperative management of cardiac function is the top priority. Close monitoring of cardiac and renal functions is required, including assessing whether preoperative volume overload has been alleviated, implementing hydration therapy to prevent acute kidney injury, and remaining vigilant for acute heart failure."Second, strengthen patient positioning management and wound care,Apply appropriate protective restraints to prevent common post-interventional complications, such as bleeding and hematoma at the puncture site.Third, closely monitor patients for major complications such as thrombosis, arrhythmias, infection, and thrombocytopenia. Fourth, maintain diuretic therapy for at least three months to allow for right ventricular remodeling.Instruct patients to closely monitor for symptoms such as chest tightness, shortness of breath, and edema, accurately record fluid intake and output, and weigh themselves daily. If body weight increases by more than 2 kg consecutively over 2–3 days, or if bilateral lower extremity edema develops, volume overload should be suspected, and prompt medical attention should be sought. Additionally, regarding organ functional changes and outcomes associated with tricuspid regurgitation (TR), AI-based venous imaging can be utilized to identify that, following the elimination of TR, patients exhibit increased cardiac output and decreased right atrial pressure and systemic venous pressure, thereby leading to morphological improvements in abdominal organs and veins.
4.4 Optimal Timing for Intervention in Tricuspid Regurgitation
The tricuspid valve has long been referred to as the “forgotten valve,” often overlooked due to its considerable tolerance and the insidious nature of early clinical manifestations in patients.Severe tricuspid regurgitation is closely associated with prognosis, and therefore early intervention is warranted.Unlike mitral valve surgery, which has a “gold standard,” tricuspid valve intervention is often performed too late, resulting in a 5-year recurrence rate of annuloplasty as high as 40% and a mortality rate as high as 10%. Therefore,Timely intervention is key to preventing irreversible right ventricular damage and organ failure.Studies have shown that the greater the severity of tricuspid regurgitation (TR), as indicated by the regurgitant volume TRV (ml) and the regurgitant fraction TRF (%), the higher the patient mortality rate.
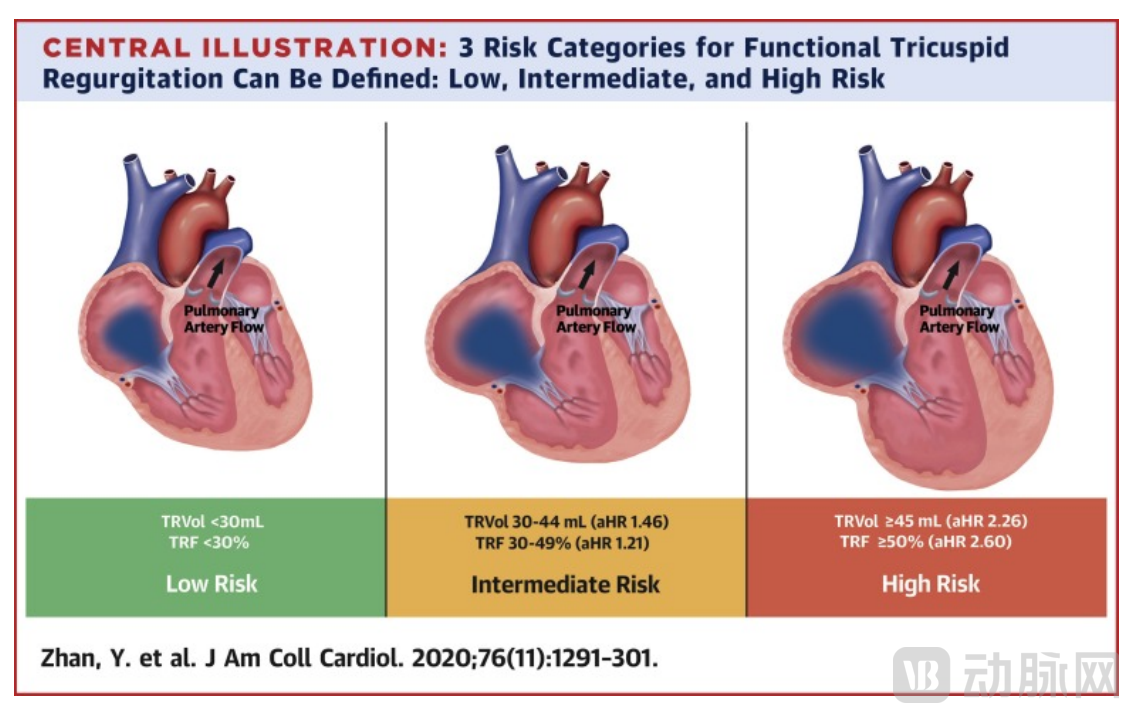
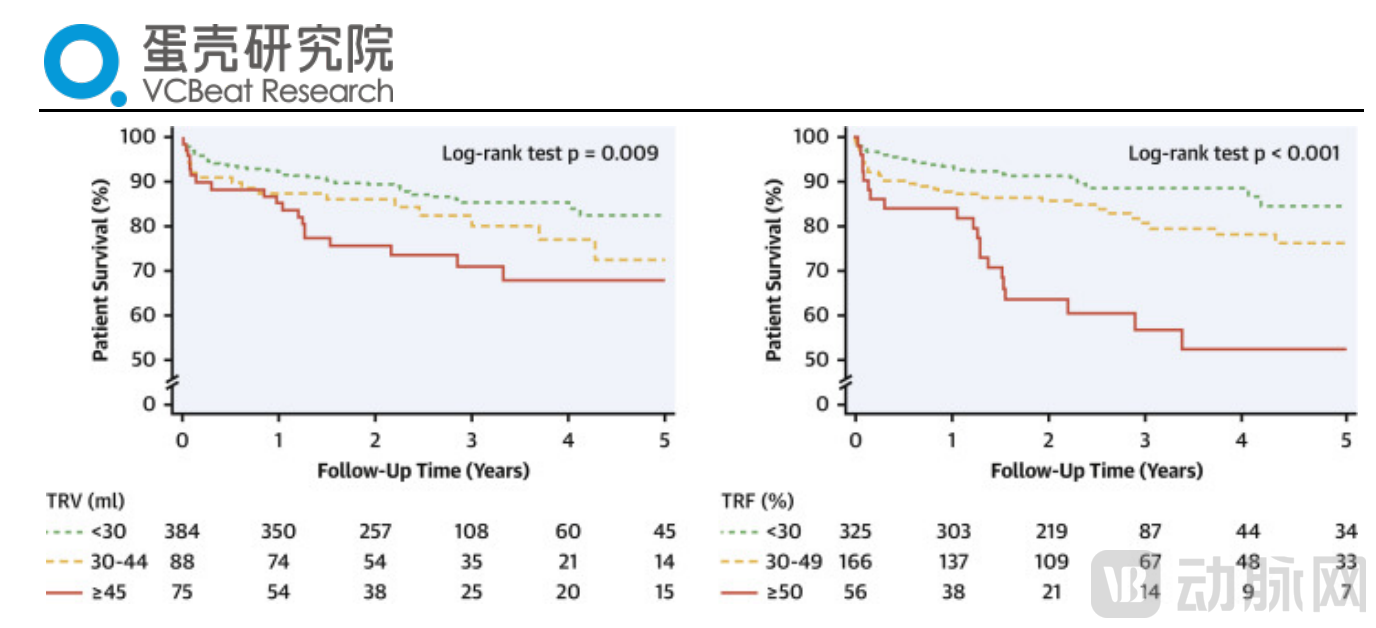
Figure 80: Evolution of TR and Corresponding Mortality Rates
Source: Natural History of Functional Tricuspid Regurgitation Quantified by Cardiovascular Magnetic Resonance, VCBeat
4.5 Discussion on Endpoints of Tricuspid Valve Interventional Therapy
The extent of reflux elimination should be assessed individually based on the patient’s anatomical structure and disease course characteristics.Valve replacement can achieve excellent immediate surgical outcomes; however, previous studies have indicated that tricuspid regurgitation (TR) should not be eliminated too completely. A significant reduction in TR leads to a sharp increase in antegrade flow across the tricuspid valve, markedly increased pulmonary blood flow, and a substantial rise in pulmonary artery pressure, which can result in severe heart failure and death. In patients with secondary TR complicated by right ventricular dysfunction, TR may serve as a compensatory mechanism. Immediate and complete correction of TR may prevent the right ventricle from adapting in time, potentially leading to acute right heart failure; therefore, candidates for valve replacement should not have severely impaired right ventricular function. Furthermore, the persistence of regurgitation even after open surgical repair of the tricuspid valve suggests that TR is not merely a pathological condition but also a protective and buffering mechanism for cardiac function. Although the degree of improvement following TR repair may appear less pronounced than that observed with mitral regurgitation (MR), any reduction in TR severity yields clinically significant benefits in terms of symptom relief and hard endpoints.
4.6 Clinical Evidence for Tricuspid Valve Interventions Continues to Strengthen
Published by PCR LV in 2022bRIGHT Real-World StudyOne-year follow-up results from the first 200 patients demonstrated sustained reduction in tricuspid regurgitation (TR) in 86% of cases, with a low adverse event rate (11.5%), further validating the findings of the TRILUMINATE trial. Evidence from the five-year follow-up of 500 patients is anticipated. With continuous improvements in devices, ultrasound imaging, and operator expertise, transcatheter edge-to-edge repair (T-TEER) holds promise for application in patients with larger coaptation gaps (GAP) and more severe baseline disease. However, the bRIGHT study has certain limitations, including the lack of data on key factors influencing post-procedural tricuspid stenosis and long-term prognosis, such as GAP width, number of implants, and changes in post-procedural transvalvular pressure gradients. It also did not report important indicators such as TR, which contributes to systemic congestion, nor did it provide evidence of benefit in heterogeneous patients with complex anatomical features in real-world settings. Therefore, further research is needed to determine which patient subgroups, stratified by tricuspid valve anatomy and other clinical baseline characteristics, will derive greater benefit from T-TEER, and to support the expansion of T-TEER indications beyond high-surgical-risk patients with severe TR.
4.7 Outlook on the Landscape of Tricuspid Valve Interventional Therapy
Multi-device combined "toolkit" provides a complete solution.Chapter 2 has already elaborated in detail that personalized pathway selection should be adopted for patients with different anatomical structures and disease course characteristics. Therefore, the future landscape of interventional therapy will feature the coexistence of multiple devices, working together to address tricuspid regurgitation.With the continuous accumulation of clinical evidence and operator experience in TEER, future expansion of indications and application potential are promising.As the first transcatheter edge-to-edge repair (TEER) procedure to initiate clinical studies and receive market approval in the field of tricuspid valve intervention, it has continued to accumulate substantial clinical evidence in recent years, supporting significant improvements in patients' quality of life.