Clinical Value-Driven New Drug Development: Insights from Real-World Practice
On June 29, 2023, at the VB-Link Future Medical Achievement Transformation and Cooperation Conference held at the InterContinental Hotel in Yujiapu, Binhai New Area, Tianjin, the Executive Director of the Office of the Drug Clinical Trial Research Center at the Cancer Hospital, Chinese Academy of Medical Sciences—Tang YuPublished"New Drug Development Guided by Clinical Value"keynote address.
Director Tang Yu introducedHealthcare InstitutionsIts importance in clinical research and new drug development: Clinical practice serves as both the starting point and the endpoint of new drug development. Clinicians who face patients are not only the ones who raise the needs but also the practitioners who verify the efficacy of new drugs. Tang Yu mentioned that in recent years, around“Clinical Value-Oriented New Drug Development”It has sparked extensive discussion in the medical field. The biopharmaceutical industry possesses unique characteristics and should prioritize itsSocial Attributes and the Mission to Advance Human HealthClinical value orientation is the foundation of pharmaceutical innovation; the performance and acceptance of new drugs depend on whether they meet clinical value needs. Tang Yu also mentioned the needs that oncologists pay attention to, such asSurvival Extension, Precision Therapy, and Health Management for Long-Term Survivorsetc. In clinical design and research, it is necessary toClosely Integrate R&D and Clinical Sides, engage in in-depth communication and discussion while maintaining an open mind. Meanwhile, clinical trials should, to the extent possible,Delivering Optimal Therapies for Broad Applications, ensuring that research findings reflect the true value of the drug. Combination therapy should consider the rationality of biological mechanisms to achieve better clinical outcomes.

Transcript of the Speech
It is a great pleasure to have the opportunity to share with you our insights gained from work. By way of brief introduction, the Cancer Hospital of the Chinese Academy of Medical Sciences serves as the National Clinical Research Center for Oncology, the National Quality Control Center for Standardized Diagnosis and Treatment of Cancer, and the site of the National Drug Clinical Research Center certified by the China Food and Drug Administration. It is a national flagship specialized cancer hospital that integrates medical care, education, research, and prevention, conducting comprehensive basic research and clinical diagnosis and treatment related to oncology. We conduct a substantial number of clinical trials on novel anti-cancer drugs and new medical devices each year, playing an integral role throughout the entire new drug development pipeline.The clinical setting is the starting point, where we raise the needs; of course, we are also the endpoint., conducting clinical trials in hospitals to verify whether products developed by various companies can benefit all of humanity.
In recent years, there has been vigorous discussion surrounding the concept of clinical value-oriented new drug development. What exactly constitutes clinical value, and how should we conduct new drug development guided by this principle? These are the questions I have been tasked with addressing today.
The biopharmaceutical industry itself has many unique characteristics. Professor Guan Jian discussed numerous ethical issues in the medical field. We have indeed observed that, compared with other products, while the biopharmaceutical industry possesses the attributes of general commodities, we place significant emphasis on itsSocial Attributes, I believe that every hospital and everyone engaged in the biomedical industry (whether in investment or R&D) harbors in their heart"Improving Human Health, Transforming Human Destiny"...dream. The biopharmaceutical industry is subject to stringent regulation because the launch of every product and technology is closely tied to human life. While companies naturally consider profitability when introducing products, within a broader framework, all industry practitioners must give due consideration to how to advance the health and well-being of humanity as a whole and promote social welfare.
In such a special circumstance, we observe that “clinical value-oriented” is the cornerstone of pharmaceutical innovation. Whether a product ultimately performs well and gains acceptance among physicians and patients hinges on its ability to deliver clinical value. Conversely, if a drug aligns well with our clinical needs—such as the star ADC (antibody-drug conjugate) in oncology last year, DS-8201 for breast cancer treatment—it demonstrates strong clinical value by significantly addressing unmet medical needs.
In recent years, the U.S. Food and Drug Administration (FDA) and China’s National Medical Products Administration (NMPA) have issued a series of policies encouraging us to focus on the more urgent challenges facing healthcare. From a regulatory perspective, these incentive policies aim to facilitate progress and development in particularly difficult fields, while minimizing both R&D costs and subsequent commercialization expenses. The NMPA’s 2021 release of the “Guiding Principles for Clinical Development of Antineoplastic Drugs with a Focus on Clinical Value” sparked significant controversy within the industry. However, from our perspective as physicians, the principles outlined in this document merely reiterate well-established concepts. Its strong resonance within the industry has prompted deep reflection among many professionals. This may also serve as a reminder that we should return to our fundamental mission and reconsider the proper direction for drug development.
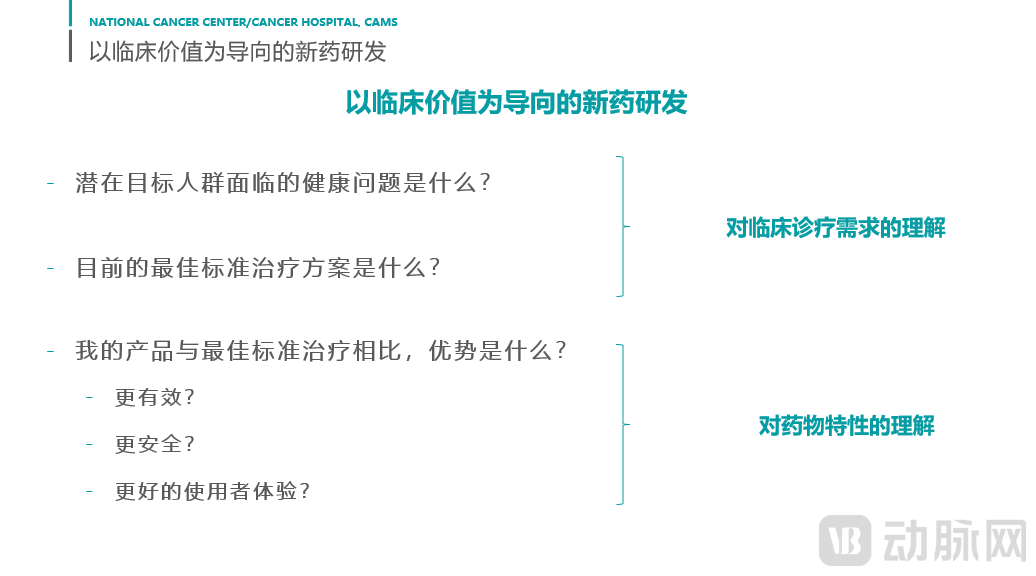
From a clinical value perspective, the first question we need to consider:What Is Clinical Value. Over the years, we have discussed this issue at many conferences: is it the pursuit of longevity or the pursuit of quality of life? This should be the authentic aspiration of every individual’s life. Even the emperors and high-ranking officials in ancient China sought immortality and eternal youth. In essence, what weThe goal is to live longer, with greater dignity and higher quality of life., which remains the paramount objective in clinical practice. When applied to new drug development or specific issues, we continuously question ourselves throughout the implementation of every idea and product: What health problems can this product truly address? What is the current best solution for these health issues? What are its advantages and limitations, and what improvements are needed? What specific advantages does this product offer compared to current standard treatments? From a scientific perspective, such advantages may include greater efficacy, prolonged survival, better glycemic control, or improved vision; alternatively, the efficacy may be comparable but with a superior safety profile; or, with similar efficacy and safety, it may provide a better patient experience—for instance, reducing dosing frequency from once monthly to once every three months, or transitioning from continuous medication to a one-time administration that resolves all issues. From a commercial standpoint, advantages may include lower costs and easier storage and transportation, among others, butDifferentiated Advantages"Always the foundation for standing firm in this market."
These three questions—the first two essentially reflect an understanding of current clinical needs. To obtain answers to these two questions, it is necessary toGet closer to physicians and frontline healthcare workers to understand what is currently happening in clinical practice.. Big data can reveal the overall picture, but it often fails to capture microscopic details. The underlying causes behind the phenomena identified by big data may require direct engagement with frontline staff and end users to foster stronger connections and deeper understanding. Regarding the subsequent issues, thisProduct AdvantagesWhat it is requires a deeper understanding.Drug Characteristics、Characteristics of the Technology, only with a deeper understanding can you better identify the differences between this product and current standard treatments, which will also help you better assess the product’s value. Answering these questions requires continuous and in-depth communication between R&D and clinical teams, emphasizing the need for ongoing dialogue starting from the early stages of development.
As oncologists, we will discuss the greatest clinical need in the field of oncology: the primary need isSurvival. Although the five-year survival rate for cancer in China has currently reached approximately 40% and is projected to rise to around 45% in five years, cancer remains a major threat to human health. In recent years, driven by the trend of immunotherapy, both survival rates and treatment efficacy for cancer have been continuously improving. However, even with such significant advances, for the common types of cancer listed here in China, where first-line treatments are predominantly immunotherapy or immunotherapy combined with chemotherapy, the median progression-free survival (PFS) is only about 7–9 months. Including current targeted therapies, the median PFS for most diseases treated with targeted therapy is approximately 12 months. We can hardly be satisfied with these data, as cancer patients have higher unmet needs. This was evident at the VB-Link conference, where many companies presented solutions; if better therapies, whether immunotherapeutic agents or targeted drugs, could be developed...Significantly Prolonging Survival Time in First-Line Patients, or inIdentifying Better Treatment Options for Drug-Resistant Populations, the product and medication will certainly be well received by patients and physicians.
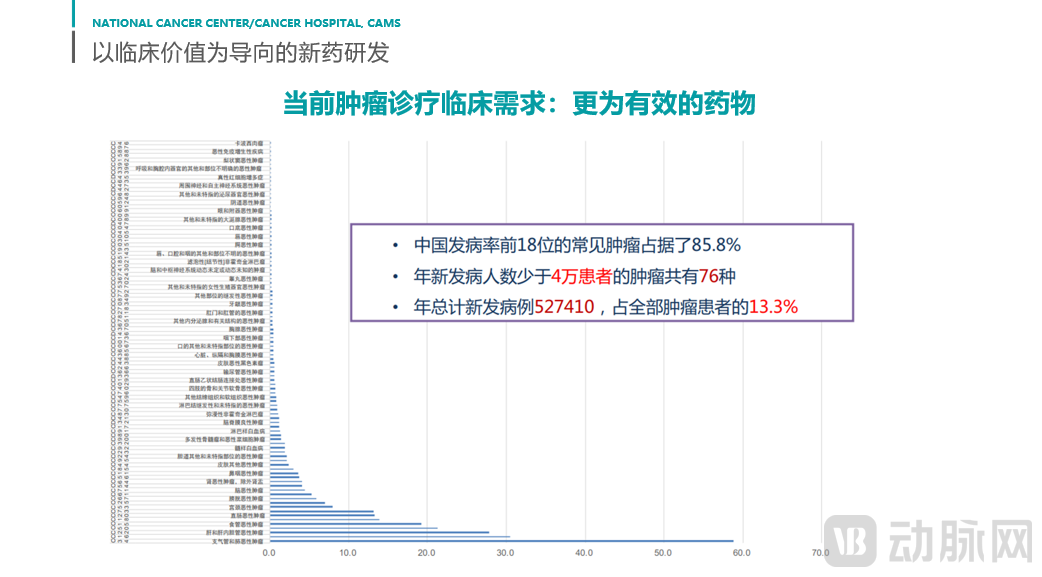
These are merely common cancer types, or those that have seen significant breakthroughs in treatment in recent years. If we turn our attention to the broader spectrum of rare tumors, the challenges in improving survival outcomes become even more pronounced. In China, the top 18 most common cancers account for approximately 85.8% of all cases. According to European and U.S. standards, a disease is considered rare if its annual incidence is less than 5–6 per 100,000 people. Given China’s large population base, we have adopted a lower threshold of 2.5 per 100,000. Even by this definition, there are still 76 types of rare tumors, which collectively account for 13.2% of all cancer patients—a proportion that is far from negligible. So, what is the current state of treatment for these patients? For more than half of them, clinical guidelines explicitly state that there is no standard of care. In fact, even conventional chemotherapy lacks standardized regimens for many of these rare tumors, and existing treatment options areBased on physicians' experience or by drawing on treatment regimens for other malignancies。
While diseases such as lung cancer and breast cancer have made significant strides in therapeutic areas including immunotherapy and targeted therapy, the vast majority of rare tumors lack any evidence supporting the use of immunotherapy or targeted therapy, with chemotherapy remaining the first-line treatment. However, this does not mean that our novel therapies offer no benefit to these patients; in fact, our statistical results reveal that one-third of patients with these rare conditions actuallyPresence of Actionable TargetsTherefore, mechanistically, targeted therapy is expected to be effective in these patients. Similarly, PD-L1 expression in half of the patients approaches the “PD-L1 > 1” threshold observed in lung cancer, suggesting that immunotherapy should also be effective for this subgroup. However, due to the heterogeneity of these patients and their relatively small numbers compared with major cancer types, current research remains significantly limited. Identifying effective pharmacological agents in clinical practice is an urgent unmet need for these patients.
Having discussed the issue of survival, the second question—Precision Medicine. In the 1990s, precision medicine was a novel term; today, it has become a consensus across oncology treatment, as seen with novel targeted therapies and immunotherapies. We frequently observe that regulatory agencies recommend early exploration of biomarkers to help identify the patient populations most likely to benefit from these drugs. However, this endeavor is not easy and requires betterLeveraging Artificial Intelligence and Big Data, to conduct more comprehensive and superior analyses for cancer patients. To achieve more precise diagnosis, it is essential to identify the right tools for precision diagnostics, whether they are reagents or emerging technologies. These tools must help cancer patients find treatment regimens better suited to their individual needs. The therapeutic model in which a single drug is suitable for 100 cancer patients will certainly not be common in the future.
Thirdly, an aspect that often receives little attention is that the five-year survival rate for cancer patients in our country has reached 40%, which means that there will be a growing number ofLong-Term Survivors of Cancer, for cancer patients with long-term survival, he needs to consider not only living longer but also how to live with better quality and well-being. For cancer patients whose condition has become chronic,Drug Safetyissues, and these patients inLong-term Health Managementissues, among others, will also become very prominent. For instance, in the case of patients with early-stage breast cancer, the survival rates in China are now on par with those in Europe and the United States, with a five-year survival rate exceeding 90%. This means that there is little difference between the life expectancy of these patients and that of their age-matched peers. In Europe and the United States, the leading cause of death among such early-stage breast cancer patients is not cancer, but cardiovascular events.。For patients, managing cardiovascular issues and mitigating complications arising from long-term treatment are persistent concerns shared by both healthcare providers and patients. Currently, we lack effective therapeutic interventions for many of these conditions, such as chemotherapy-induced peripheral neuropathy and radiation dermatitis. In clinical practice, although physicians may prescribe certain medications symbolically, we are aware that their benefits are largely placebo effects. The introduction of a truly efficacious drug would provide substantial benefit to patients.
The needs I just listed are very broad requirements that exist in the field of oncology. I believe that in any disease area, if you engage in in-depth discussions with frontline physicians, you will discover many unmet clinical needs that may not be captured through statistical data alone. Returning to the point mentioned earlier, understanding clinical needs indeed requiresR&DandClinical SideThe integration must be exceptionally tight, initiated early, and carried out in depth. From the clinical perspective, we aim to provide timely feedback on issues encountered in practice to technical teams and maintain prompt communication. On the R&D side, I have always believed that scientists need to dispel a common misconception. Scientists sometimes fixate on an idea; they may anchor their clinical research to a specific problem identified three or five years earlier and proceed with clinical development. Even after development, they often remain steadfast in the belief that their product can perfectly resolve that clinical issue. However, time can change everything. Three to five years later, the problem they initially studied may no longer be the most critical one in clinical practice, and the solution they launch may not be the optimal approach to addressing current clinical needs. How, then, can we effectively bridge these two sides?"Communicate and discuss more, and maintain an open mind.", is the best solution to this problem.
The next question involves a real-world case in which a manufacturer of a certain antiemetic drug approached us to conduct a clinical study. Currently, most antiemetics are administered via injection, although some are available in oral formulations. The manufacturer in question has developed a transdermal patch, which offers greater convenience in administration. They proposed designing a trial to compare this antiemetic patch with standard antiemetics used in chemotherapy. In China, patients undergoing chemotherapy who are at moderate-to-high risk of emesis receive prophylactic antiemetic treatment prior to chemotherapy. In the proposed design, one randomized group would receive the transdermal antiemetic patch, while the other would receive conventional intravenous antiemetics.From a trial design perspective, this control setup is sound. However, we must consider the setting in which patients receive chemotherapy. Currently, the majority of chemotherapy infusions are administered in hospitals. Under routine practice, nurses administer intravenous antiemetics by injecting them into the infusion port (“Y-site”) after establishing venous access, followed immediately by the chemotherapy infusion. If the act of “injecting” the antiemetic is replaced by applying a patch to the patient’s arm, the patient’s actual experience remains unchanged, as they still require venous access for the chemotherapy infusion. Thus, the pain associated with needle insertion is not avoided, given that intravenous infusion is inevitably required afterward.While the concept of a transdermal antiemetic is appealing and aims to improve patient experience, it does not substantively enhance the patient’s experience within the actual clinical workflow. Consequently, we advised the manufacturer that although the transdermal antiemetic offers no benefit to patients when used in hospital settings, it may be better suited for home care. The product would demonstrate substantial advantages if used in conjunction with oral chemotherapy agents, or if administered after same-day completion of chemotherapy infusion (in which case the antiemetic serves a therapeutic rather than prophylactic purpose). This case illustrates that if you do not focus on understandingClinical Practical Application Scenarios, it may not be possible to identify the actual differentiated use cases for this product.
The second question: our product has been developed, and we need to conduct clinical validation. How should we design clinical studies guided by “clinical needs”? In fact, here we““Guided by Clinical Needs”Change to“"Subject Benefit"If so, this is a particularly straightforward issue. What we need to consider is whether, throughout the entire clinical trial process, you can ensure that patients receive the current best available treatment at every critical juncture of therapeutic decision-making. We typically focus on how to select the control group in confirmatory studies and what strategy should be adopted for the investigational treatment. Of course, there are many other questions, but the one we repeatedly ask ourselves during the entire design phase is: Are we truly providing patients with the best possible treatment? A major point of contention is the selection of the control group. In oncology, standard-of-care treatments theoretically serve as controls, but which specific standard therapy should be chosen? We may be inclined to select the weakest option, as it offers the highest probability of demonstrating success; however, does this truly reflect the drug’s maximum clinical value? I believe everyone has their own assessment of this matter.
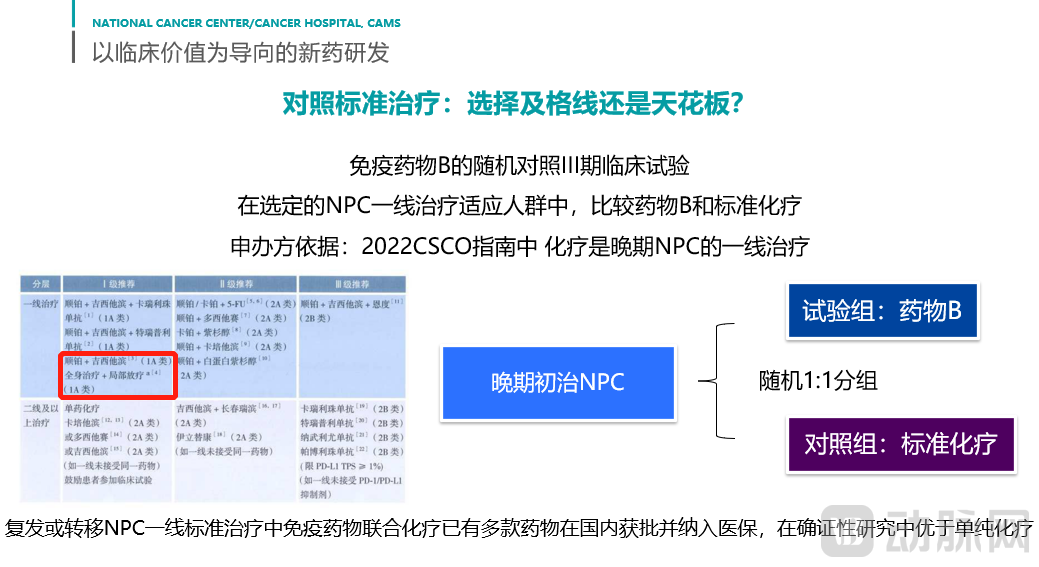
Let us consider an example involving an immunotherapy product targeted at nasopharyngeal carcinoma, a cancer type with high prevalence in China. The initial study design featured a 1:1 randomization, with one arm receiving the investigational drug and the other receiving standard chemotherapy. It is worth noting that in recent years, immunochemotherapy has firmly established itself as the first-line treatment for nasopharyngeal carcinoma. In the recently updated 2022 CSCO Guidelines, numerous immunotherapy regimens combined with chemotherapy have been included as first-line recommendations. Furthermore, from a health insurance perspective, these drugs have rapidly gained reimbursement approval, ensuring excellent accessibility. At that time, I raised a question: Given the current medical landscape, is it still appropriate to use chemotherapy alone as the standard of care? The manufacturer responded that their chemotherapy regimen remains within the scope of standard treatment, as referenced in the CSCO Guidelines (highlighted in red in the figure below).
In fact, if we adopt a more neutral perspective, it is clear that such a clinical trial design cannot be described as “clinical value-oriented.” While this approach may facilitate rapid market approval of a drug, it does not help the drug achieve its maximum value throughout its entire lifecycle. Stakeholders should reflect on this: when employing a therapy that is already becoming obsolete, how will you promote it in the future? How will you persuade physicians and patients to adopt this treatment regimen? These are critical considerations that must be taken into account.
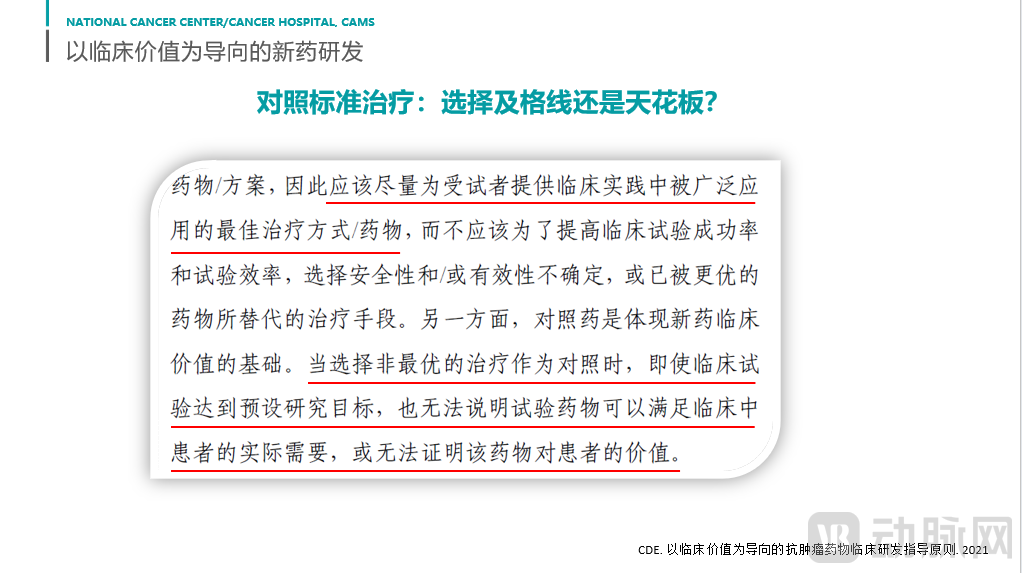
As we will see, the Center for Drug Evaluation (CDE) of the National Medical Products Administration officially released the "Guiding Principles for Clinical Development of Antitumor Drugs with a Focus on Clinical Value," which clearly states that every effort should be made to provide subjects with treatments available in clinical practice.The Widely Adopted Optimal Treatment Modality. I greatly appreciate this final statement: if the treatment regimen selected is not optimal, even if therapeutic goals are achieved, it fails to reflect the true value of the drug. Setting aside whether the Center for Drug Evaluation (CDE) will impose stricter standards for drug approval in the future, let us reconsider such a design and its execution. Despite the substantial costs incurred, this approach may not necessarily represent the best choice for the drug itself.
Experimental therapies are more complex. If an experimental therapy advances to the confirmatory trial phase, we internally believe that such a therapy should be capable of outperforming the current standard of care; otherwise, researchers would not initiate such confirmatory studies, and ethics committees would not grant approval. Before evaluating a treatment regimen, we expect to review all available data so that we can at least conclude that the therapy is worthy of competing against the standard of care. This raises a question: How can the value of an experimental therapy be better demonstrated? Is it possible for this experimental therapy to surpass the standard of care in clinical practice? Here, we provide an example. A currently very common treatment approach in oncology is the so-called“add on”, specifically combining two drugs with three drugs. If the triple-drug regimen proves suboptimal, a fourth drug may be added; indeed, four-drug combination therapies have already received regulatory approval. As illustrated in this trial, patients with lung cancer who have failed first-line therapy—despite having previously responded well to dual immunotherapy combinations—may opt for an intensified approach by adding chemotherapy to the two immunotherapeutic agents, thereby employing a triple- or quadruple-drug combination strategy. This aggressive approach aims to achieve remarkable outcomes and may potentially yield superior efficacy. However, the challenge with combination therapy lies in:The toxicity of treatment has basically increased rather than decreased.Furthermore, when the underlying mechanisms are not well elucidated, combination therapy does not always yield a synergistic effect (i.e., “1+1>2”); in many cases, it fails to even achieve an additive effect (“1+1=2”). We recently encountered a case involving a specific cancer type for which two drugs had already been approved and marketed. We initiated a study on combination therapy using these two agents. While each drug demonstrated a favorable safety profile when administered as monotherapy, and the rationale for their combined use appeared sound, the combination unexpectedly resulted in toxicities that no one had anticipated. Biological mechanisms are highly complex; therefore, when designing combination regimens, it is essential to thoroughly evaluate whether the preclinical biological rationale is sound. Without a robust mechanistic basis, simply adding more agents may lead to only marginal improvements in efficacy, while significantly increasing adverse effects and patient burden/costs. From a clinical value perspective, such a medical strategy is not cost-effective. This is precisely why the Center for Drug Evaluation (CDE) specifically addresses “combination therapy” in its Guiding Principles for Clinical Development of Antineoplastic Drugs with a Focus on Clinical Value.
In summary, the principle of “clinical value orientation” should be deeply ingrained in the minds of all those engaged in new drug development or involved in the biopharmaceutical and healthcare industries. Our ultimate overarching goal is invariably to advance the health and well-being of humanity as a whole. In this process, how weConsideration of Clinical Needs, howExploring the Advantages of Drug and Technological Differentiation, integrate the principle of "clinical value orientation" throughout the R&D process. Throughout this process, we need to discuss this issue more effectively by fostering close collaboration between the R&D and clinical teams, ensuring real-time communication and continuous updating of information. In various trials, including the drug development process, better adherence to clinical value orientation means better"Patient needs and interests-oriented, thinking from the perspective of maximizing patient benefits."This question can help us find answers to many questions.