The $10B RSV Race After 67 Years: Who’s Leading the Global Charge?

Trinomab
Developer of Natural Fully Human Monoclonal Antibody New Drugs
In May 2023, the previously empty RSV vaccine landscape saw the successive approvals of vaccines from GSK and Pfizer, reigniting the competition for this billion-dollar market.
Why Say “Again”?
RSV, first isolated as early as 1956—shouldn’t there already be a mature and available preventive vaccine?
In fact, the R&D path for RSV infection prevention has not been smooth.
In 1956, U.S. researcher J. A. Morris and colleagues isolated a virus from chimpanzees exhibiting respiratory disease. Subsequently, in 1957, virologist Robert M. Chanock isolated the same virus from the respiratory tract of pediatric patients with severe respiratory distress; this pathogen was later named Respiratory Syncytial Virus (RSV). Research on the prevention and treatment of RSV commenced shortly thereafter.
Generally, the primary methods for preventing infectious diseases are vaccines for active immunization and specific immunoglobulins (or monoclonal antibody drugs) for passive immunization. The initial RSV preventive products developed were live-attenuated or inactivated vaccines, which represented a mature technology at the time. However, the first RSV vaccine to enter clinical trials globally—Pfizer’s formalin-inactivated RSV vaccine (FI-RSV)—failed to deliver the expected efficacy. Moreover, it caused enhanced respiratory disease (ERD), leading to exacerbated illness upon RSV infection among vaccinated individuals and resulting in the deaths of pediatric trial participants. Consequently, the FDA urgently halted clinical trials of RSV vaccines in the United States, and RSV vaccine development entered a “dormant period.”
To expedite the resumption of vaccine research, scientists began investigating the causes of ERD. Studies suggest that RSV vaccines may activate Th2-CD4+ T cells, subsequently leading to cytokine-mediated pneumonia. This research has reignited interest in RSV vaccine development, with major pharmaceutical companies such as AstraZeneca/Sanofi, Merck & Co., Johnson & Johnson, GSK, Novavax, and Enanta all entering the field.
However, the market has underestimated the risks associated with the RSV prevention sector. Novavax’s repeated major setbacks in this field once pushed the company to the brink of bankruptcy. Its post-F protein recombinant nanoparticle vaccine (ResVax) was once hailed as “the most promising RSV vaccine,” and its significant success in Phase II clinical trials drove the company’s market capitalization up to $2.2 billion. However, this momentum did not carry through to the completion of Phase III trials. In September 2016, the company announced that its Phase III clinical trial involving 11,856 adults aged 60 and older had failed to meet either the primary or secondary endpoints. As a result, the company’s market value plummeted by 80% to less than $300 million, triggering partial layoffs. On February 28, 2019, Novavax again announced that the study of this vaccine in pregnant women had failed to meet the primary endpoint, concluding four years of research without achieving satisfactory results.
Prior to 2013, RSV vaccines were all designed and developed against the post-fusion F protein (Post-F). In 2013, structural biologists Jason McLellan, Tongqing Zhou, and others optimized and engineered the F protein.1, a stable prefusion F protein (Pre-F) was obtained, and a new neutralizing antibody epitope, Ø, was discovered. The study revealed that the Pre-F-specific antigenic epitope Ø elicits neutralizing antibodies with the highest potency, exhibiting neutralizing activity dozens of times greater than that of antibodies targeting other epitopes. This finding may explain the reasons for previous vaccine failures. This achievement was recognized as one of the Top 10 Scientific Advances of 2013. Since then, RSV vaccine development strategies and types have rapidly expanded.
GSK’s candidate vaccine GSK3003891A, which uses the pre-F protein as an antigen, was discontinued shortly after entering Phase II clinical trials. Due to risks of preterm birth and miscarriage observed in the Phase II trials, the company also announced last year that it had halted its research on maternal RSV vaccine candidates. In late March this year, Janssen Pharmaceuticals, a subsidiary of Johnson & Johnson, announced its decision to withdraw from the adult RSV vaccine program, terminating its ongoing Phase III EVERGREEN study and ending its adenovirus-vector-based RSV vaccine pipeline, which had been in development since 2014.
The good news is that in May this year, two RSV vaccines (pre-F protein) from GSK and Pfizer were successively approved, finally giving the green light for RSV prevention in individuals aged 60 and above.
Meanwhile, passive immunization strategies—specifically antibody therapeutics—have also undergone several generations of technological advancement. In 1998, Synagis (palivizumab), the world’s first monoclonal antibody for RSV prevention developed by AbbVie/Sobi, was launched. This drug is indicated only for high-risk infants and young children, such as premature infants with a gestational age of ≤35 weeks, and pediatric patients with bronchopulmonary dysplasia or congenital heart disease, covering merely approximately 2% of the infant population in need of protection. Despite its short half-life, which necessitates 3–5 injections during a typical RSV season (five months), the drug still generated annual sales of approximately $1 billion at that time.
In November 2022, Beyfortus (nirsevimab), an antibody therapy co-developed by AstraZeneca and Sanofi, was approved in the European Union, becoming the world’s first long-acting RSV preventive measure for the infant population. A single intramuscular injection of Beyfortus provides sustained protection throughout the entire RSV season.
In addition to vaccines and antibody-based drugs, the industry is also actively developing small-molecule inhibitors, interferons, and other forms of RSV prophylaxis, making concerted efforts to overcome this “R&D black hole.”
RSV is the primary pathogen causing lower respiratory tract infections in infants and young children worldwide, with an infection rate of up to 90% among children under the age of two. It is estimated that2, globally, approximately 33.1 million children under the age of 5 develop severe acute lower respiratory tract infections due to RSV infection each year, resulting in hospitalization of 3.2 million children and 118,000 deaths.
In addition to children, older adults and individuals with chronic lung diseases are also at high risk of developing severe illness or even death following RSV infection. According to data from the U.S. Centers for Disease Control and Prevention (CDC), RSV causes approximately 60,000–120,000 hospitalizations among adults aged 65 and older each year, resulting in 6,000–10,000 deaths. It is estimated that 5.5% of adults aged 65 or older worldwide contract RSV annually, with a higher case fatality rate observed in this elderly population. The CDC recommends that society pay close attention to this issue.
For decades, RSV infection has led to hospitalizations, severe illness, and deaths, posing a serious threat to life and imposing a substantial burden on healthcare expenditures. Therefore, a safe and effective preventive measure against RSV has become particularly critical and urgent.
According to research data from Frost & Sullivan, the global market for RSV drugs (including both therapeutic and prophylactic agents) was approximately USD 1.9 billion in 2022. With novel prophylactic agents offering superior efficacy, longer duration of protection, and broader patient coverage entering the market in the coming years, the global RSV prophylaxis market is expected to continue its growth trajectory. It is projected to reach USD 12.8 billion by 2032, representing a compound annual growth rate (CAGR) of 20.8%.
In the field of RSV passive immunization agents, according to research data from Frost & Sullivan, the current market size for RSV monoclonal antibodies in North America and Europe is approximately $1 billion. With the development of the RSV monoclonal antibody pipeline, the market size is projected to expand to approximately $3.8 billion by 2030. In China, an RSV monoclonal antibody for prophylaxis is expected to be approved for marketing in 2024, with the potential to capture a market worth approximately RMB 700 million. This market is further projected to grow to approximately RMB 4.6 billion by 2030.
This positive market growth data has attracted numerous innovative pharmaceutical companies worldwide. As of today, there are nearly 70 RSV prevention candidates in the global clinical development pipeline. Overseas multinational pharmaceutical giants have made rapid progress in their RSV pipelines, with most having already obtained Phase III clinical trial data. There are also many domestic players in China; those with faster progress include Trinomab and Advaccine, while other companies such as Aim Vaccine, CSPC Pharmaceutical Group, Zhifei Biological Products, Jiachen Xihei, Biokangtai, BlueQuail Biosciences/Watson Biopharma, and Clover Biopharmaceuticals are also striving to catch up.
Currently, disease prevention is primarily achieved through two approaches: “active immunization” and “passive immunization.” Common preventive measures include vaccines, antibody drugs, specific immunoglobulins, small-molecule inhibitors, and interferons.
In principle, active immunity is acquired when the body is exposed to "non-self" antigens through natural infection or vaccination. It represents protective capacity generated by the body’s own immune system and is characterized by being acquired, specific, and variable. Passive immunity, on the other hand, occurs when the body passively receives antibodies, sensitized lymphocytes, or their products, thereby acquiring specific immune competence. It is characterized by a rapid onset of effect and a relatively short half-life.
In other words, active immunity relies on the body’s own immune system to generate a response, and its efficacy is influenced by the functional capacity of the immune system. In contrast, passive immunity is less affected by the immune system; its efficacy is primarily determined by passively administered substances such as antibodies. The longer the half-life of these substances, the more prolonged the immune protection.
In terms of specific target populations, ideal active immunity is typically elicited only in individuals with intact immune systems. For infants and young children whose immune systems are still developing or are weak, as well as for special populations with relative immune deficiencies, the direct administration of antibodies or similar substances to confer immunity represents a more effective and safer option.
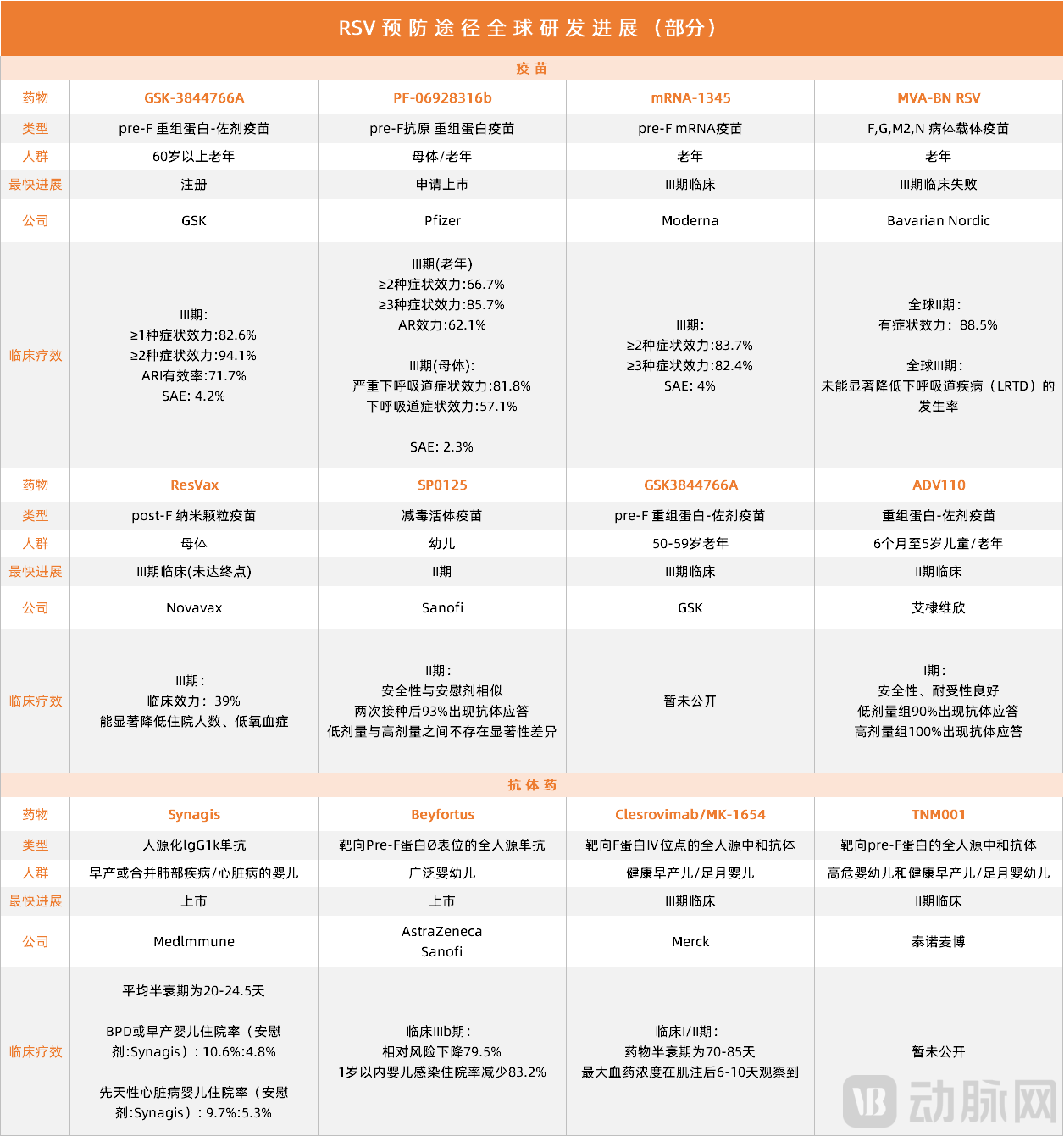
Global Pipeline Progress of RSV Prevention (Vaccines + Antibody Drugs) Under Development or on the Market (Partial)
(Data source: publicly available data from the entire internet)
In light of immunological principles and the global pipeline landscape, we are pleased to observe that, after more than 60 years of arduous exploration, the global RSV prevention pipeline has largely identified appropriate R&D strategies and continues to pursue innovative avenues.
Currently, global pipelines under development or already on the market demonstrate clearly differentiated strategic layouts in terms of technological processes, target populations for immunization, and modes of immunity. Notably, the most advanced pipelines primarily target the elderly, pregnant women, and infants; vaccine candidates based on active immunization mainly cover the former two groups, while antibody drugs utilizing passive immunization predominantly target the infant population.
Both vaccines that have successfully obtained marketing approval are recombinant protein vaccines using the pre-F protein as the antigen. GSK’s vaccine, GSK3844766A, developed for adults aged 60 and older, was successfully approved by the FDA with a 12:0 vote in favor of efficacy and a 10:2 vote in favor of safety. Clinical trials for this vaccine in adults aged 50–59 are also underway, with plans to expand the indicated population this year. Pfizer’s vaccine is currently approved only for the prevention of RSV in individuals aged 60 and older. Its clinical trials targeting maternal populations have yielded positive top-line data, based on which the U.S. FDA has accepted the priority review application for this pipeline and set the PDUFA date for August this year. This means the vaccine is expected to be approved before next year’s RSV season, enabling infants to have protection against RSV infection from their “first breath.”
Among the vaccine candidates in development, Moderna’s mRNA vaccine is advancing most rapidly and has entered global Phase III clinical trials. Recently, the Danish company Bavarian Nordic announced the failure of its RSV vaccine candidate, MVA-BN RSV. In the Phase III VANIR study, MVA-BN RSV failed to significantly reduce the incidence of lower respiratory tract disease (LRTD), leading the company to discontinue the vaccine program. MVA-BN RSV is a viral vector-based RSV vaccine that utilizes modified vaccinia virus Ankara (MVA) technology to express five antigens: F, G (subtypes A and B), M2, and N. Notably, prior to the announcement of MVA-BN RSV’s failure, RSV vaccines from Johnson & Johnson, GSK, and Vaxart had also encountered setbacks using the viral vector platform.
On the other hand, infant vaccines led by Sanofi’s SP0125 pipeline are also under continuous exploration. Designed for intranasal administration, this vaccine has already demonstrated positive antibody responses and a favorable safety profile in current clinical studies, and is expected to enter Phase III clinical trials in the first half of 2024.
Currently, there are two passive immunization agents on the market: Synagis, a humanized IgG1κ monoclonal antibody from MedImmune, and Beyfortus (nirsevimab), a monoclonal antibody jointly developed by AstraZeneca and Sanofi. Synagis is indicated only for infants born prematurely or with congenital conditions; due to its short half-life, it requires administration approximately every 20 days, totaling about 6–8 injections throughout the RSV season.
Beyfortus was developed to address the pain points associated with antibody therapies, such as economic cost, population coverage, and injection frequency. In the Phase IIb clinical trial involving all infants and the Phase III MELODY trial, Beyfortus significantly reduced the incidence of medically attended lower respiratory tract infections caused by RSV within 150 days post-administration compared to the single-dose placebo group, demonstrating a 79.5% reduction in relative risk. The safety profile observed in these trials was similar to that of the placebo group. Furthermore, in the MEDLEY trial, Beyfortus demonstrated safety and tolerability comparable to Synagis. Beyfortus is currently the world’s first single-dose passive immunization agent for RSV approved for all infants, and it remains the only one currently approved and marketed.
Merck’s humanized neutralizing antibody Clesrovimab, currently in Phase III clinical trials, is highly anticipated. This drug is expected to further expand the indicated population for RSV passive immunization to include healthy preterm infants. Existing clinical studies have confirmed that the drug has a half-life of up to 85 days and reaches peak plasma concentration within as little as 6 days after intramuscular injection.
Currently, the antibody drug pipeline with the most rapid progress in China is being advanced by Trinomab. Its independently developed fully human neutralizing antibody injection, TNM001, is undergoing Phase II clinical trials in healthy preterm and full-term infants. This drug has the potential to become the first RSV antibody medication for infants and young children in China. Additionally, two other RSV preventive drugs in China are on the verge of entering clinical trials: Raybiopharm’s RB0026 injection and Akebia Therapeutics’ AK0610 injection.
Overall, based on the fundamental principles of active and passive immunity, existing marketed and investigational RSV preventive products form a distinct complementary landscape when categorized by target population. Currently, the competitive dynamics between active and passive immunity in the RSV sector are characterized more by internal competition within each modality than by direct rivalry between them. Companies engaged in active immunity R&D are more numerous, and their primary focus will be to rapidly advance their pipelines to capture market share across various regions. Meanwhile, companies in the passive immunity space must not only develop safe, long-acting antibodies but also achieve breakthroughs across multiple dimensions—including prematurity, congenital conditions, and age—to expand indications and encompass a larger infant and young child population.
The technical theories and market landscape are already clear, but in practical implementation, conducting relevant clinical trials for RSV prevention remains challenging, regardless of the immunization approach.
The primary reason is that such trials can be conducted only once a year, requiring clinical teams to complete the enrollment of all participants before the annual RSV epidemic season begins. Furthermore, as preventive pipeline products, their clinical guidelines mandate sample sizes exceeding 1,000 subjects, making patient recruitment significantly more challenging than for therapeutic trials. More importantly, RSV infection surveillance systems remain inadequate in many countries, rendering it difficult to obtain accurate data on local epidemic timing.
GSK and Pfizer’s two vaccines for the elderly were able to “cross the finish line” first, partly because recruitment in this target population is relatively easier and compliance is relatively higher.
Another adult population—pregnant women—benefits from a prevention mechanism in which maternal vaccination induces antibody production, with these antibodies then transferred to the fetus in utero. Thus, while vaccination constitutes active immunization for the mother, the fetus derives benefit through passive immunity. Theoretically, a single dose of this vaccine not only equips the mother with resistance against RSV infection but also ensures that the newborn possesses immediate RSV-specific immune protection at birth, making it a highly cost-effective and timely strategy for RSV prevention.
However, researchers have found that in specific clinical studies, the efficacy of passive fetal immunization primarily depends on the level of antibodies produced by the mother. Individual maternal variations directly impact preventive effectiveness, and adverse outcomes such as preterm birth may occur. More importantly, antibodies in the fetus are time-limited; only infants born during the RSV epidemic season can benefit from this therapy. Infants who miss the epidemic season will still face a high risk of infection when the next season arrives.
From this perspective, passive immunization remains the optimal choice for infants, a vulnerable population. However, the development of antibody-based drugs presents significant challenges. On one hand, it is necessary to develop long-acting antibodies capable of providing coverage throughout the entire RSV epidemic season (150+ days). On the other hand, various challenges arising from clinical trials must be overcome. In addition to the common difficulties in RSV prevention clinical trials mentioned earlier, it is particularly challenging to communicate trial risks to parents of infants in a neutral manner and to complete patient recruitment. Furthermore, for infants, factors such as physical constitution and body weight directly influence dosage and frequency of administration. How to achieve precise stratification of the study population and implement appropriate trial protocols serves as a test of a company’s clinical experience and capabilities.
Based on this analysis, the diversity of therapies emerging from the complementary landscape of active and passive immunization has enabled players in this sector to explore more boldly; however, significant challenges remain in the critical stage of clinical research. Over the past 60 years, scientists have laid the foundation in basic research and technical principles. Moving forward, accelerating clinical research may become a shared objective for companies to tackle collaboratively within this “harmonious and complementary” framework.
2023 is destined to be a breakthrough year for RSV prevention. Amidst the "triple pandemic" of influenza, COVID-19, and RSV, health regulatory agencies worldwide have begun to place greater emphasis on RSV prevention.
Currently, two RSV vaccines for the elderly from GSK and Pfizer, as well as an infant monoclonal antibody from AstraZeneca and Sanofi, have been launched in overseas markets, but there remains a void in the field of RSV prevention in China.
Whether for active immunization in adults or passive immunization beneficial to infants, accelerating the R&D and market launch of existing pipelines has become an inevitable trend for domestic innovative pharmaceutical companies. Optimistically speaking, Chinese pharmaceutical companies have demonstrated greater “acumen” in this field than before; currently, no small number of enterprises have RSV prevention candidates in their pipelines, and clinical studies are progressing smoothly. Given the current development trajectory, China’s RSV prevention products are not entirely out of step with global R&D progress, holding significant promise for future participation in international market competition.
In the post-pandemic era, public awareness of disease prevention in China has significantly increased, sending a positive signal for drug R&D and commercial promotion. Next, we will see how domestic innovative pharmaceutical companies capture this “multi-billion-dollar market.”
References:
1. Jason S. McLellan, Man Chen, Sherman Leung, Kevin W. Graepel, Xiulian Du, Yongping Yang, Tongqing Zhou, Ulrich Baxa, Etsuko Yasuda, Tim Beaumont, Azad Kumar, Kayvon Modjarrad, Zizheng Zheng, Min Zhao, Ningshao Xia, Peter D. Kwong, and BarneyS. Graham. Structure of RSV Fusion Glycoprotein Trimer Bound to a Prefusion-Specific Neutralizing Antibody.Science. 2013 May 31; 340(6136): 1113–1117. doi:10.1126/science.1234914.
2. Shi T, McAllister DA, O’Brien KL, Simoes EAF, Madhi SA, Gessner BD, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. 2017;390:946–58.