Yizao Medical Submits IPO Prospectus: Revolutionizing Esophageal Cancer Screening with a 3-Minute Painless Sampling Device Validated in 17,498-Participant National Study
Esophageal Cancer: A Frequently Overlooked High-Incidence Malignancy
Data from the National Cancer Center show that in 2016, there were 252,500 new cases of esophageal cancer in China, accounting for 6.21% of all malignant tumors. According to the Guidelines for Screening, Early Diagnosis, and Early Treatment of Esophageal Cancer in China, the number of new esophageal cancer cases in China reached 324,000 in 2020, representing 53.70% of the global total, while the number of deaths was 301,000, accounting for 55.35% of the global total.
Esophageal cancer carries a poor prognosis; over 80% of patients are diagnosed at an intermediate or advanced stage, with a 5-year survival rate below 30% and significantly impaired quality of life.
The path to breaking this impasse is already paved—patients with early-stage esophageal cancer who receive treatment can achieve a 5-year survival rate of up to 95%.
Early screening, early diagnosis, and early treatment are crucial for improving survival rates in esophageal cancer. Since the vast majority of patients in the early stages are asymptomatic, implementing early screening among asymptomatic high-risk populations is an essential strategy for the prevention and control of esophageal cancer.
Yizao Medical, in collaboration with its R&D team, has launched a novel esophageal cell collector that enables painless, non-invasive esophageal sampling in just three minutes. Integrated with an AI-powered early screening risk assessment model, this device facilitates early detection of esophageal cancer.
March 15, “Machine Learning-Based Computational Cytology for Screening Esophageal Squamous Cell Carcinoma and Adenocarcinoma of the Esophagogastric Junction: A Nationwide, Multi-Cohort, Prospective Study”Published in The Lancet Gastroenterology & Hepatology, a leading international journal in gastroenterology, introducing the latest breakthroughs in early screening and diagnosis through the integration of novel esophageal collection devices with AI and machine learning.
VCBeat interviewed Dr. Gao Ye, the first author of the paper and a key contributor to the project’s development, to discuss a novel approach for early screening of esophageal cancer.
Esophageal cancer primarily comprises two histological types: squamous cell carcinoma and adenocarcinoma. Esophageal adenocarcinoma and cardia cancer are collectively referred to as gastroesophageal junction adenocarcinoma. In China, both esophageal squamous cell carcinoma and gastroesophageal junction adenocarcinoma exhibit high incidence rates. Current screening methods are limited to invasive endoscopy, with no alternative screening modalities available, making it difficult to cover the hundreds of millions of individuals in the target population and hindering the advancement of early diagnosis and treatment efforts.
Unlike other cancers that can be detected through stool and blood tests, the diagnosis of esophageal cancer requires complete cellular sampling of the esophagus and gastroesophageal junction, followed by morphological diagnosis. The primary challenge to address is how to achieve high-density collection of cellular samples along the entire length of the esophagus.
The R&D team has turned its attention to the balloon cytology screening method from the last century. Balloon cytology was once widely implemented in high-incidence regions of esophageal cancer in China. The procedure involves inserting a balloon-like device into the subject’s esophagus, inflating it, and then withdrawing it. Due to significant discomfort during sample collection, poor patient tolerance, low cellular yield, and a consequent false-negative rate of nearly 50%, this technique has been largely discontinued.
The R&D team optimized and improved the collector material by employing sponge-like polymer materials and refining pore density parameters, enabling the collection of over 6 million cells per patient per procedure.
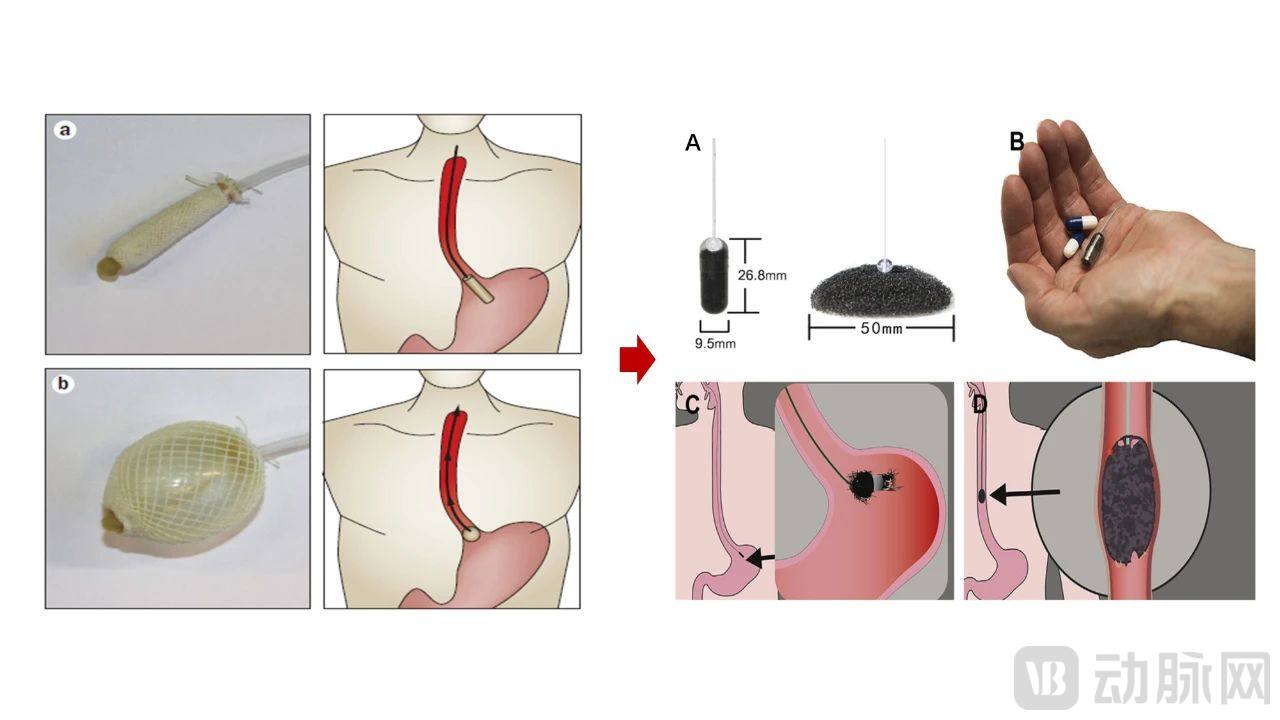
Traditional Esophageal Balloon Cytology Screening (Left) vs. Novel Cell Collector (Right)
Photo provided by the interviewee
Preparing slides from 6 million cells yields anywhere from 50 to 100 slides. Where can one find cytopathologists, who are already in short supply? Moreover, the goal of early screening for esophageal cancer is large-scale implementation. Manual diagnosis, characterized by low efficiency, insufficient experience, and high subjectivity, makes it difficult to achieve efficient operation.
The R&D team came up with the idea of AI-assisted diagnosis.
There are numerous precedents for the application of AI-assisted cytological diagnosis in endoscopy and oncology. Drawing on the example of AI-assisted diagnosis in cervical cancer cytology screening, the R&D team has incorporated whole-slide image digitization and AI-assisted diagnosis into their screening model.
At this point, the challenges of early screening for esophageal cancer have not been readily resolved—machine learning requires large volumes of precisely annotated images and accurate diagnostic pathways. This brings us to a fundamental question: What are the pathological criteria for exfoliated esophageal cells?
Cytomorphological diagnosis of esophageal cancer is not a routine practice, and experienced physicians are exceedingly rare. The R&D team invited cytopathologists with extensive diagnostic experience to develop an improved cytological grading system for the esophagus and gastric cardia. This system was formulated by referencing the esophageal balloon cytology diagnostic criteria from the last century and integrating the latest Bethesda System for cervical cytology classification.
In the machine learning process for screening models, each sample annotation requires confirmation by three cytopathologists. Dr. Takano stated, “From the very beginning of training, we have made every effort to ensure the accuracy of cytology image annotations, thereby ensuring the validity of the machine learning data and laying a solid foundation for accurate cell recognition in subsequent stages.”
This nationwide study enrolled 17,498 participants and, by integrating sample data with machine learning techniques, developed and validated a risk assessment model for screening esophageal and gastroesophageal junction cancers. The model achieved a sensitivity of 94.5% and a specificity of 91.9%.
Following initial screening, 90.3% of individuals in the population can be classified into the low-risk group and do not require endoscopic examination. Limited endoscopic resources can be efficiently allocated to the identified high-risk individuals, while the population benefits from a more accessible, convenient, painless, and non-invasive large-scale screening solution.
The world's first spherical cell sponge for early screening of esophageal cancer comes from Cyted, a UK-based company (CytospongeTM), primarily applicable for screening the precancerous condition of esophageal adenocarcinoma—Barrett’s esophagus. Its diagnostic logic lies in identifying and screening for disease markers within the sample, specifically Trefoil Factor 3 (TFF3) in goblet cells.
Following this logic, Cyted has developed a semi-automated diagnostic system leveraging AI machine learning models. Under this diagnostic workflow, two sections are cut from the paraffin-embedded block of the cytology sample: one is subjected to hematoxylin and eosin (H&E) staining for sample quality control (i.e., to assess the presence of glandular epithelial cell clusters from the gastroesophageal junction), while the other undergoes TFF3 immunohistochemical staining for diagnostic purposes (i.e., to detect positively stained cells).
In contrast, China’s novel cell collectors and screening risk assessment models follow a diagnostic pathway that is entirely different from that of Cyted. Squamous cell carcinoma accounts for 90% of esophageal cancer cases in China. Unlike Barrett’s esophagus, which is a precancerous lesion associated with adenocarcinoma of the gastroesophageal junction, squamous cell carcinoma lacks a well-defined precancerous state, and there are currently no universally accepted biomarkers or highly mutated genes to aid in diagnosis. This indicates that the biomarker-based diagnostic approach is not viable.Therefore, the R&D team selected cytological diagnosis, which involves larger sample sizes and a higher degree of difficulty.
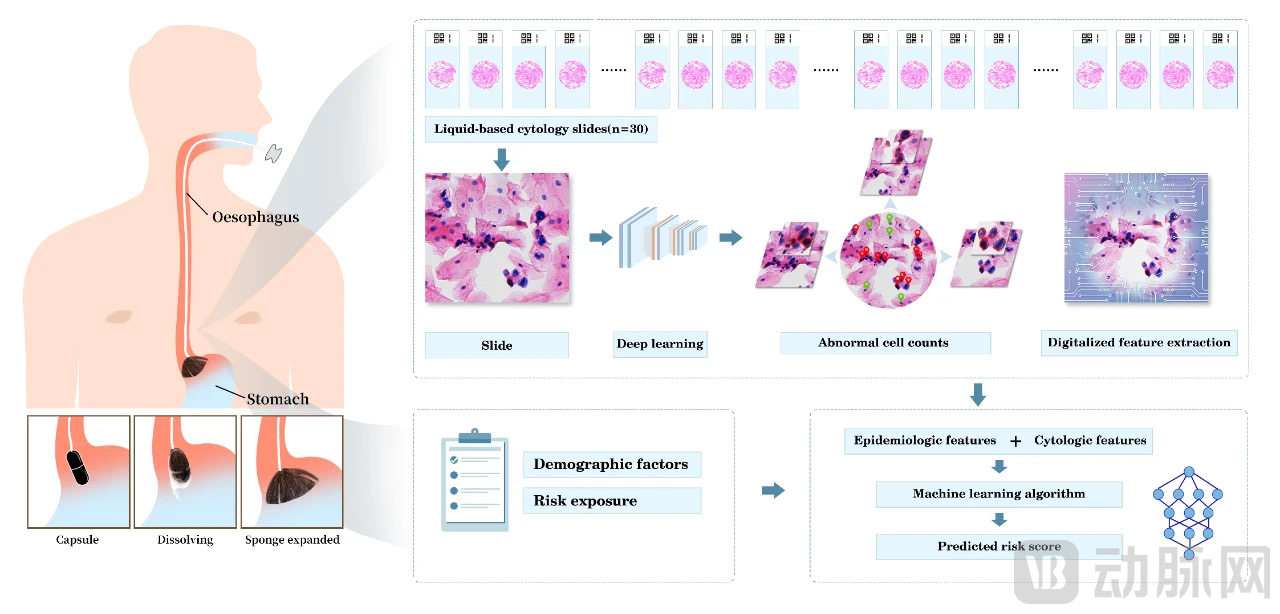
Novel Cell Collector Model (Left) and Multimodal Feature Extraction with Risk Assessment Model Construction (Right)
Photo provided by the interviewee
Adenocarcinoma of the gastroesophageal junction has a well-defined site of origin. However, squamous cell carcinoma and its precancerous lesions may occur at any location along the entire length of the esophagus. This necessitatesThe collector must capture cells without any blind spots.Dr. Takano stated, “The average width of the esophagus is 2 cm. Given individual variations and the dynamic processes of esophageal contraction and relaxation, reduced conformity between the collector and the esophageal wall may lead to incomplete sampling, thereby potentially resulting in missed diagnoses of squamous cell carcinoma.”
The R&D team increased the collector width from 3 cm to 5 cm, enabling it to seamlessly conform to the full length and width of the esophagus. Material improvements were also made: the capsule shell was changed from gelatin to glutinous rice, reducing the dissolution time from 7 minutes to 2 minutes while enhancing softness. This optimization improved the sampling experience and eliminated the need for pharyngeal anesthesia during the procedure.
In addition to its unique design targeting squamous cell carcinoma, the R&D team has also incorporated into the screening risk assessment modelInnovatively Incorporating Epidemiological Models“Epidemiological models are not uncommon in early screening protocols for gastrointestinal tract cancers, but purely epidemiology-based approaches have shown suboptimal efficacy. In 2021, we observed a low positive predictive value; however, after integrating epidemiological analysis, the predictive value improved,” said Dr. Gao Ye.
The incorporation of epidemiological data constitutes multimodal information integration, enabling the inclusion of patient risk factors and exposure history in the analysis, thereby enhancing diagnostic performance. Multimodal prediction models that integrate cytopathological and epidemiological features canPersonalized, Quantitativeto predict the risk of esophageal cancer in examinees.The aforementioned process does not require diagnostic interpretation by cytopathologists, thereby further reducing human subjectivity and facilitating the promotion of screening in large target populations.
Following the publication of these research findings in a Lancet specialty journal, Dr. Sandord Dawsey, a senior investigator at the U.S. National Institutes of Health (NIH), published a commentary in the same issue, highly praising this method as a “breakthrough in esophageal cancer screening.”
The improvement in positive predictive value brought by epidemiological models is actually related to the significant regional differences in the incidence of esophageal cancer in China.
According to the Guidelines for Esophageal Cancer Screening, Early Diagnosis, and Early Treatment in China, high-incidence areas of esophageal cancer in China are mainly concentrated in regions near the Taihang Mountains (Henan, Hebei, Shanxi, Taian in Shandong, Jining in Shandong, and Heze in Shandong), as well as Anhui, northern Jiangsu, Nanchong in Sichuan, Yanting in Sichuan, Shantou in Guangdong, and southern Fujian.
In addition to large-scale screening in high-risk areas, individuals at high risk for esophageal cancer should also maintain a certain frequency of screening. The Guidelines consider individuals aged ≥40 years in non-high-risk areas who have a family history of esophageal cancer or possess high-risk factors for esophageal cancer (such as smoking, heavy alcohol consumption, squamous cell carcinoma of the head and neck or respiratory tract, preference for hot and pickled foods, and poor oral hygiene) as the high-risk population.
The vast high-risk regions and high-risk populations create immense potential for product innovation, while also laying the foundation forThe Ultimate Goal of Esophageal Cancer Early Screening Models—Population AccessibilitySo, how can individuals with early screening needs complete sampling as soon as possible and obtain results at the fastest speed?
Similar to conventional medical testing pathways, early screening for esophageal cancer initially prioritized hospitals in closest proximity to the disease burden. During the trial period from January 2021 to June 2022, pilot programs in high-incidence regions for esophageal cancer covered 39 hospitals and five communities, including several county-level hospitals.
The research team believes that, within the framework of county-level medical consortia, promoting new methods for early esophageal cancer screening may offer a superior solution. By establishing a collaborative model led by hospitals and jointly built with township health centers and community health stations, early screening can be effectively decentralized to the grassroots level. This approach enables large-scale screening while ensuring rapid referral for subsequent endoscopic diagnosis and disease treatment.
In response, Yi Zao Medical has launched two solutions for its early screening product for esophageal cancer.Teams with pathological testing capabilities can independently operate a complete system encompassing sample collection, slide preparation, pathological examination, and result delivery. For medical institutions with limited resources, only sample collection needs to be performed, requiring merely a small, dedicated sampling area and staff trained in sample collection. After samples are collected, they can be shipped via logistics to partner pathology laboratories, and test results can be directly accessed through official WeChat accounts or websites.
Another pathway: Early screening for esophageal cancer is making its way into health checkup centers and convenient screening sites.
Meinian Onehealth has introduced Yizao Medical’s esophageal cancer early screening product and has currently launched pilot programs for the “Innovative Project for Precise Early Screening of Esophageal Cancer” in Qingdao and Jinan, Shandong Province. In Yantai, Shandong, individuals can access the screening channel directly through the “Yantai Travel” APP and complete sample collection at the JD Health Operations Center.
Currently, Yizao Medical’s early esophageal cancer screening system has achieved large-scale production, encompassing the entire workflow from novel cell collection devices at the front end and laboratory sample processing quality control systems to risk assessment reporting platforms. The company plans to promote its solutions across medical institutions at all levels, health examination centers, and government-led regional screening programs, with the aim of establishing a population-based screening network. Ultimately, this initiative seeks to increase public participation rates in early screening and support China’s efforts in esophageal cancer prevention and control.