Antibody-Drug Conjugates (ADCs): A Focused Review on Tumor Therapy Innovation and Pipeline Highlights
Editor’s Note: This article is from the Shanghai Biomedical Fund, authored by Liu Yanjie. VCBeat has obtained authorization to republish it.
In recent times, there has been an overwhelming amount of news in the pharmaceutical industry regarding Antibody-Drug Conjugates (ADCs).ADCs, by virtue of their advantages in enhancing tumor targeting and mitigating toxic side effects, garnering sustained acclaim and attention within the industry, but itsAmid rapid development, it also faces certain challenges—how to overcome tumor heterogeneity and drug resistance? Why are antibody-drug conjugates (ADCs) so favored by investors?This article will explore this topic with you.
Table of Contents
I. Basic Concepts of ADCs
II. The Development History of ADCs
III. Representative ADC Drugs
IV. Market Size and Forecast
V. Key Transactions and Financing
VI. Challenges Facing ADCs
VII. Fund Perspectives
Abstract
Antibody-Drug Conjugates (ADCs) are an emerging class of targeted therapeutics that leverage monoclonal antibodies conjugated to cytotoxic agents to specifically deliver drugs to tumor cells.This article reviews the structural design of antibody-drug conjugates (ADCs), the development of toxins and linkers, targeting mechanisms, clinical applications, market sales, and financing transactions, with a focus on elucidating the advantages and existing challenges of ADCs in cancer therapy.Currently, antibody-drug conjugates (ADCs) are primarily used in the treatment of hematologic malignancies and certain solid tumors, achieving significant breakthroughs in several indications. However, challenges such as antigenic mutations, tumor heterogeneity, plasma instability, and drug resistance continue to pose substantial obstacles to the broader application of ADCs in oncology.Looking ahead, the rational design of novel linkers and carriers, the development of multi-target antibodies, and the combined use of antibody-drug conjugates (ADCs) with other therapeutic modalities may further enhance the efficacy and selectivity of cancer treatment.
Keywords:ADC, Tumor-Targeted Therapy, Enhertu, Monoclonal Antibody, Drug Resistance
I. Basic Concepts of ADC
Antibody-Drug Conjugate (ADC) is a novel anti-tumor therapeutic strategy., it links a highly targeted monoclonal antibody (mAb) to a small-molecule drug with potent cytotoxicity (payload) via a degradable or non-degradable linker, forming a composite molecule.AThe principle of DC leverages the high affinity and specificity of antibodies to precisely deliver drugs to antigens that are overexpressed or specifically expressed on the surface of tumor cells., and then release the drug through endocytosis or hydrolysis of linkers, exerting cytotoxic effects intracellularly, thereby achieving selective killing of tumor cells while reducing damage to normal tissues.
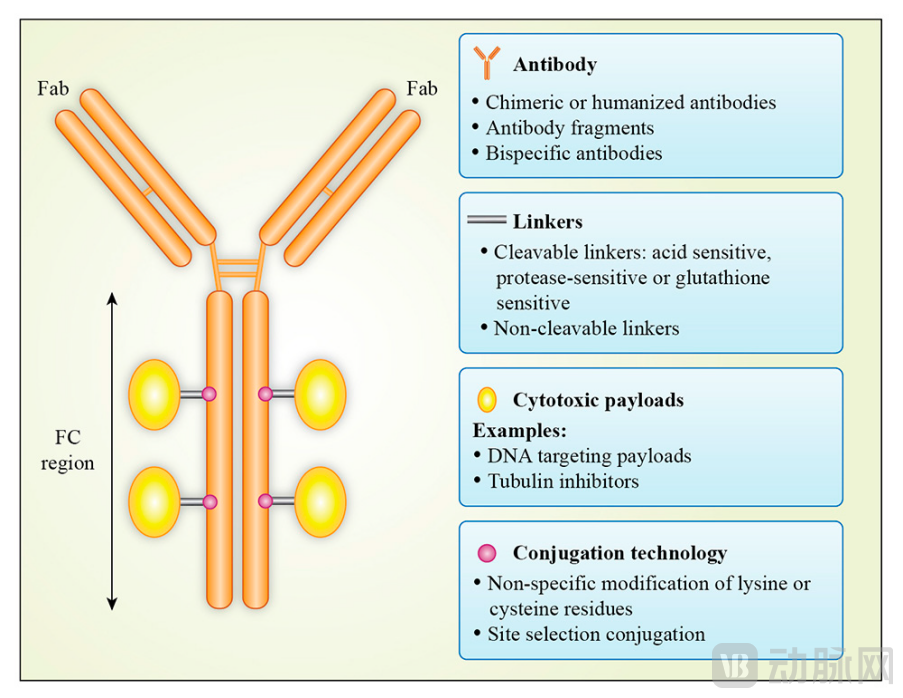
Figure 1. Basic Structure of ADCs
ADC is an innovative drug that combines antibody technology with small-molecule drug technology, offering the following advantages:
• High Efficiency:ADCs can leverage highly potent small-molecule drugs, such as microtubule inhibitors, topoisomerase inhibitors, and DNA-damaging agents, to exert strong cytotoxic effects on tumor cells. These agents are generally unsuitable for standalone use due to the severe side effects they would cause in normal cells.
• Targeted:ADCs can leverage the high specificity of antibodies to deliver drugs directly to antigens expressed or specifically expressed on tumor cells, without affecting normal cells, thereby enhancing the therapeutic index and safety of the drug.
• Flexible:ADCs can select different antibodies, linkers, and payloads based on tumor types and targets to achieve personalized and precise treatment.
II. Development History of ADCs
The development of ADCs can be divided into three generations:
• First-generation ADCs:Primarily utilizes non-cleavable linkers and murine or chimeric antibodies, resulting in lower efficacy and activity, and a higher propensity to induce immune responses and off-target toxicity.Currently, only one first-generation ADC is on the market: gemtuzumab ozogamicin (Mylotarg);It was the first approved ADC drug (2000) for the treatment of acute myeloid leukemia (AML).However, due to severe toxic reactions, Mylotarg was withdrawn from the market in 2010.Notably, the product demonstrated clinical benefits in AML after its withdrawal from the market, following adjustments to its dosing and regimen.Therefore, in 2017, the U.S. FDA re-approved the product for marketing to treat newly diagnosed CD33-positive acute myeloid leukemia (AML).
• Second-generation ADCs:It primarily utilizes cleavable linkers, humanized or fully human antibodies, and more potent small-molecule toxins,Improved tumor cell targeting and cytotoxicity.Among the currently marketed ADC products, representative drugs utilizing second-generation technology include brentuximab vedotin (Adcetris), indicated for the treatment of Hodgkin lymphoma (HL) and systemic anaplastic large cell lymphoma (sALCL); ado-trastuzumab emtansine (Kadcyla), indicated for the treatment of HER2-positive breast cancer; inotuzumab ozogamicin (Besponsa), indicated for the treatment of relapsed or refractory B-cell acute lymphoblastic leukemia (r/r B-ALL); and enfortumab vedotin (Padcev), indicated for the treatment of advanced bladder cancer. TheseSecond-generation ADCs have demonstrated favorable clinical efficacy and safety, yet certain issues remain.such as off-target toxicity, unconjugated antibodies, and poor blood stability.
• Third-generation ADCs:The primary use of site-specific conjugation technology, along with more stable, sensitive, and diverse linkers and payloads, has resulted in a stronger bystander effect and a wider therapeutic window.To achieve more homogeneous, safer, and more effective ADCs. Several third-generation ADCs have already been approved for marketing, such as trastuzumab deruxtecan (Enhertu),Indicated for the treatment of HER2-positive breast cancer, gastric cancer, and non-small cell lung cancer (NSCLC);Sacituzumab govitecan (Trodelvy), indicated for the treatment of triple-negative breast cancer; loncastuximab tesirine (Zynlonta), indicated for the treatment of relapsed or refractory diffuse large B-cell lymphoma (r/rDLBCL), among others.
III. Representative ADC Drug: Enhertu (Uherde)
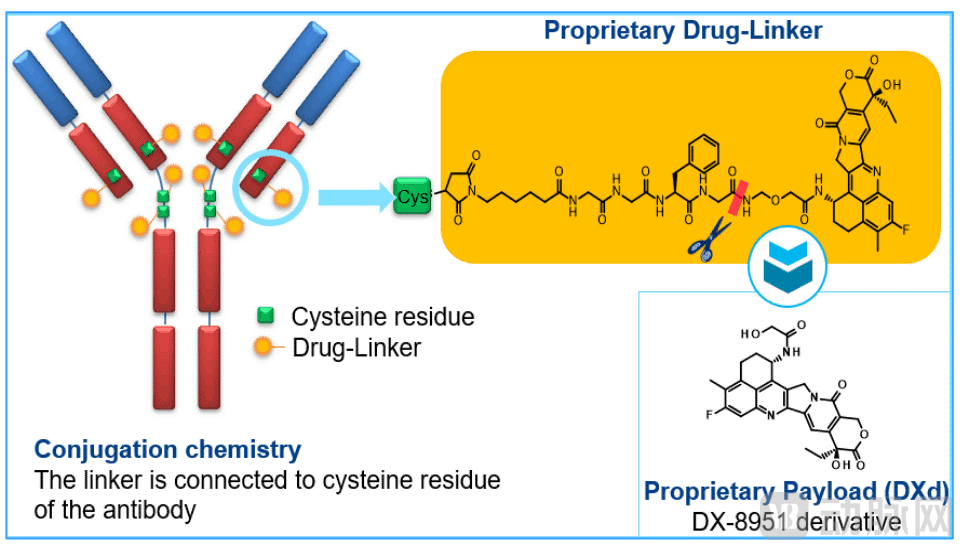
Figure 2 Structure of Enhertu
Enhertu, also known asDS-8201 (generic name: trastuzumab deruxtecan),Trastuzumab deruxtecan is a novel HER2-targeted antibody-drug conjugate (ADC).It mainly consists of trastuzumab (a HER2-targeted monoclonal antibody) and deruxtecan (an irinotecan-based chemotherapeutic agent). Enhertu was originally developed by Japan’s DaiichiOriginally developed by Daiichi Sankyo, this ADC product secured a collaboration agreement with AstraZeneca in 2019 for joint development and commercialization, featuring an upfront payment of $1.35 billion and a total transaction value of $6.9 billion. The reason this ADC has garnered significant attention from both AstraZeneca and the industry lies in its following distinctive features:
Ⅰ. It has a high drug-to-antibody ratio (DAR). Enhertu can conjugate 7–8 chemotherapy drugs to a single antibody molecule, which is 2–4 times higher than that of previously approved ADCs. This provides a solid foundation for its anticancer efficacy.
II. A linker with stability and susceptibility to specific cleavage. The linker of Enhertu not only demonstrates excellent stability in the bloodstream but also can be specifically cleaved by cathepsins within tumor cells, thereby ensuring the release of the chemotherapeutic agent in cancer cells.
III. Cytotoxic agents with a unique mechanism of action. The cytotoxic payload used in Enhertu is an innovative DNA topoisomerase I inhibitor (DXd), which exhibits tenfold greater potency than the commonly used chemotherapy drug irinotecan, thereby enabling comparable efficacy at lower doses.
IV. Possesses a potent bystander effect. The GGFG linker of Enhertu can be specifically cleaved by lysosomal proteases that are highly expressed in tumors, and the released Dxd toxin exhibits strong cell membrane permeability. Consequently, after DXd kills the cancer cells that have internalized the ADC, it can penetrate the cell membranes of neighboring cancer cells, thereby killing other cancer cells adjacent to the targeted cells and producing a “bystander effect.”
In December 2019, Enhertu received its initial FDA approval for second-line and subsequent treatment of HER2-positive breast cancer; in January 2021, Enhertu gained further FDA approval for second-line treatment of HER2-positive gastric cancer and gastroesophageal junction adenocarcinoma; in February 2023, Youhede (Enhertu) was approved by China’s NMPA for second-line and subsequent treatment of HER2-positive breast cancer.To date, the product has been approved for four indications, including breast cancer, gastric cancer, and non-small cell lung cancer.In 2022, Enhertu’s global sales reached $1.234 billion,Daiichi Sankyo expects its 2023 sales to reach $2.4 billion.
The key clinical trial results for Enhertu can be summarized as follows:
• DESTINY-Breast01
This is the pivotal trial of Enhertu for the treatment of HER2-positive metastatic breast cancer. The results showed that the overall response rate (ORR) with Enhertu was 61%, significantly superior to the 16% observed with chemotherapy agents. The median progression-free survival (PFS) was 16.2 months in the Enhertu group, compared to only 6.8 months in the chemotherapy group.
• DESTINY-Breast02
The trial is indicated for HER2-positive metastatic breast cancer, primarily comparing the therapeutic efficacy of Enhertu versus T-DM1 (ado-trastuzumab emtansine). The objective response rate was 79% in the Enhertu group and 34% in the T-DM1 group. The median progression-free survival was 25.1 months in the Enhertu group and 7.2 months in the T-DM1 group.
• DESTINY-Breast03
This trial evaluated the combination of Enhertu and chemotherapy for the treatment of metastatic breast cancer. The results demonstrated that the combination therapy further improved the response rate, with a median progression-free survival of 28.8 months.
• DESTINY-Breast04
This is a randomized, open-label, multicenter Phase III clinical trial indicated for patients with early-stage invasive breast cancer who were pathologically diagnosed as HER2-positive after surgery. The treatment group received Enhertu, while the control group received standard adjuvant chemotherapy. The primary endpoint was invasive breast cancer–free survival (iBDFS). A total of 524 patients were enrolled, with a median follow-up duration of more than 2 years. The results showed that the 2-year iBDFS in the Enhertu group was significantly higher than that in the control group. In the overall population, Enhertu reduced the risk of disease progression or death by 50% compared with TPC.
In the HER2-negative cohort, DS-8201 reduced the risk of disease progression or death by 54% compared with TPC, with median PFS of 8.5 months and 1.9 months, respectively; the risk of death was reduced by 52% in the DS-8201 group versus the TPC group, with median OS of 18.2 months and 8.3 months, respectively. Notably, this patient population has traditionally been defined as having triple-negative breast cancer. DESTINY-Breast04 is the first phase III clinical trial to yield positive results in patients with HER2-low expression, and this milestone breakthrough also provides clinical data supporting the bystander effect mechanism of Enhertu.
• DESTINY-Gastric01
This study evaluated Enhertu versus chemotherapy in patients with HER2-positive advanced gastric cancer. Among 187 patients with HER2-positive gastric or gastroesophageal junction adenocarcinoma who experienced disease progression after receiving at least two prior therapies (including trastuzumab), 125 received Enhertu and 62 received chemotherapy. The objective response rate (ORR) was 51% in the Enhertu group compared with 14% in the physician’s-choice chemotherapy group. Overall survival (OS) was four months longer in the Enhertu group than in the chemotherapy group (12.5 vs. 8.4 months).
• DESTINY-Lung01
This study aimed to evaluate the efficacy and safety of Enhertu in patients with non-small cell lung cancer (NSCLC) who overexpress HER2 or harbor HER2 mutations and have failed standard therapy. The results showed that Enhertu achieved an objective response rate (ORR) of 54.9%, a median progression-free survival (mPFS) of 8.2 months, and a median overall survival (mOS) of 17.8 months. Based on the DESTINY-Lung01 trial, the FDA approved Enhertu for the treatment of HER2-positive non-small cell lung cancer.
• Safety
In the completed clinical trials of Enhertu, the primary adverse reactions were interstitial lung disease and neutropenia. Most adverse reactions were manageable and rarely led to trial discontinuation.
IV. Market Size and Forecast
According to Frost & Sullivan’s analysis, the global market size of ADCs grew rapidly from $1.6 billion in 2017 to nearly $7 billion in 2022.USD, with a compound annual growth rate (CAGR) of 33.2%, and is projected to maintain rapid growth at a rate of 31.2% from 2021 to 2030. In the Chinese market,Following the National Medical Products Administration’s approval of the first ADC drug, Kadcyla, the domestic ADC drug market began to grow in 2020.It is expected to grow at a compound annual growth rate (CAGR) of 79.4% from 2021, reaching RMB 68.9 billion by 2030.
Nature Reviews published “The Oncology Market for Antibody-Drug Conjugates” in 2022, predicting that the market size for the 14 ADC drugs then on the market would exceed $16.4 billion by 2026. The main drivers of future market growth include: 1) expansion of indications for existing drugs; 2) extended treatment durations due to prolonged survival; and 3) continued approval and launch of new ADC drugs.Among them, Enhertu has been approved for multiple indications in breast cancer and gastric cancer, and with its prolonged usage duration, it is projected to become the best-selling ADC drug with $6.2 billion in sales.Padcev Approved for the Treatment of Urothelial Carcinoma, with Potential for Indication Expansion to Earlier Stages Affecting Larger Patient Populations in the FutureGlobal sales are expected to reach $3.5 billion in 2026, ranking second.
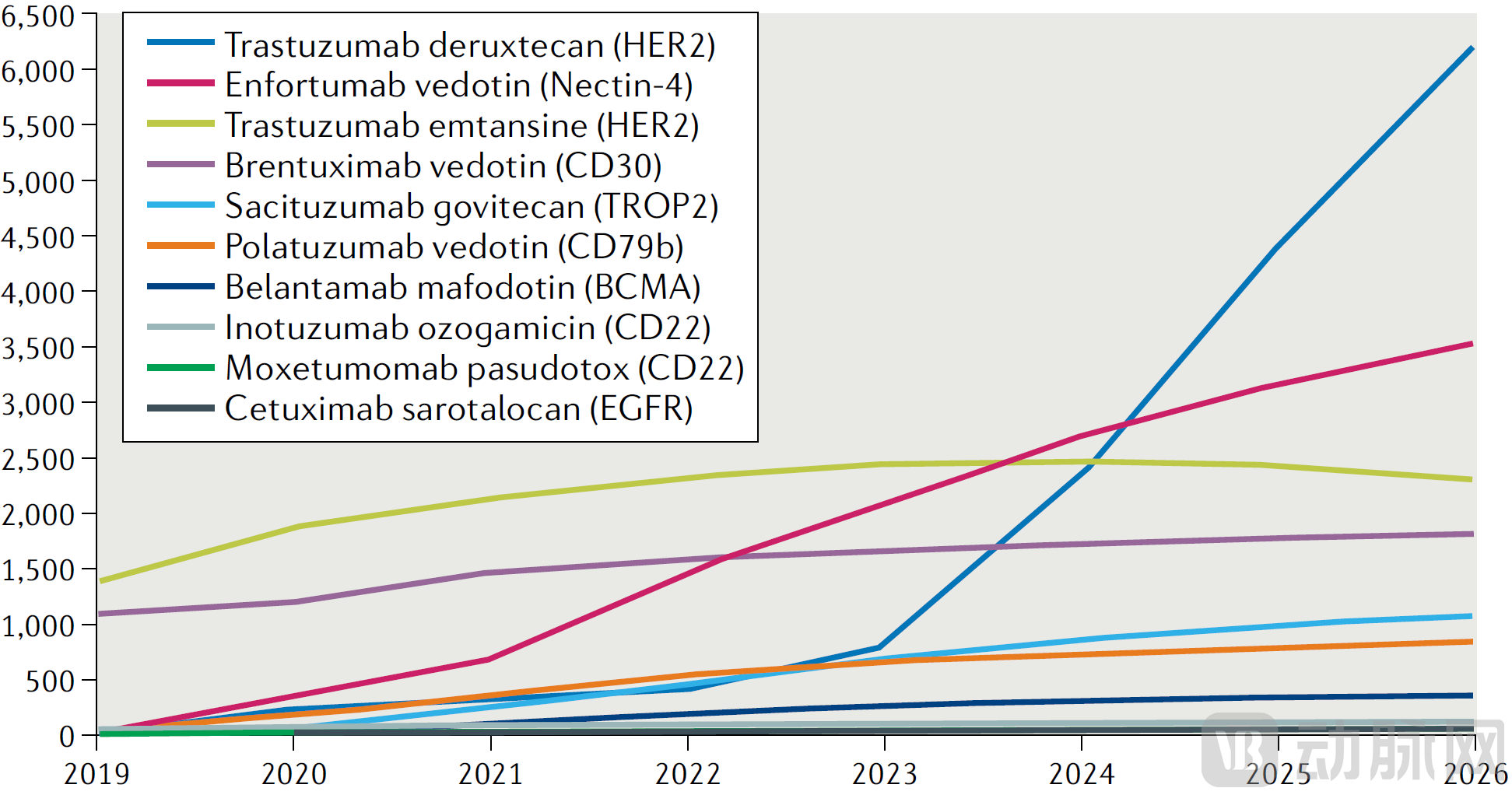
Figure 3. Market Size Forecast for ADCs Published in Nature Reviews
Currently, 15 ADC drugs have been approved for marketing worldwide, with indications covering lymphoma, leukemia, breast cancer, multiple myeloma, head and neck cancer, urothelial carcinoma, and other diseases.Among these, HER2 is the top-ranked target with three products; CD22 ranks second with two products. Additionally, ten other targets, including CD33, CD30, CD79B, and Nectin-4, each have one product. In terms of toxin selection, there are six products using MMAE/MMAF, two each using camptothecin, calicheamicin, and maytansine derivatives, and one using PBD.

Figure 4 Sales Statistics of ADC Drugs
AmputationTo date, a total of five ADC drugs have been approved for marketing in China:Including Roche's trastuzumab emtansine, Takeda's brentuximab vedotin, Pfizer's inotuzumab ozogamicin, RemeGen's disitamab vedotin, and sacituzumab govitecan, which was licensed by Everest Medicines (this product has been returned by Everest Medicines to Gilead).Among them, disitamab vedotin is the only commercially available domestically produced ADC drug.Its sales revenue in 2021 was $13 million, with projected sales of $70 million for 2022. In addition to RemeGen, other Chinese pharmaceutical companies with ADC drug candidates in their pipelines include Hengrui Medicine, Kelun-Biotech, Zhejiang Medicine, Lepu Biopharma, and CSPC Pharmaceutical Group.
During the 2022 National Reimbursement Drug List (NRDL) negotiations, four antibody-drug conjugate (ADC) drugs were involved, including RemeGen’s disitamab vedotin, which was already on the list, and three products from multinational pharmaceutical companies that were not on the list. Ultimately, Roche’s trastuzumab, Takeda’s brentuximab vedotin, and RemeGen’s disitamab vedotin were successfully included in the NRDL.
V. Key Transactions and Financing
Recent public financing and transaction news indicate that the ADC sector remains highly active.In the past two to three years, several ADC-focused startups, including Zymeworks, Kelun-Biotech, and Duality Biologics, have successively secured financing rounds worth hundreds of millions of yuan. These funds will drive the late-stage clinical trials and commercialization of their product pipelines.Meanwhile, pharmaceutical giants such as Pfizer and Merck & Co. have also chosen to acquire core technology platforms in the ADC field through multi-billion-dollar mergers, acquisitions, and licensing collaborations.It is evident that ample financing support from the capital markets, coupled with the strategic deployments and layouts of industry-leading enterprises, has jointly driven the sustained and rapid development of this emerging therapeutic field. On the arduous path of new drug research and development,ADCs are garnering sustained industry acclaim and attention for their advantages in enhancing tumor targeting and mitigating toxic side effects.
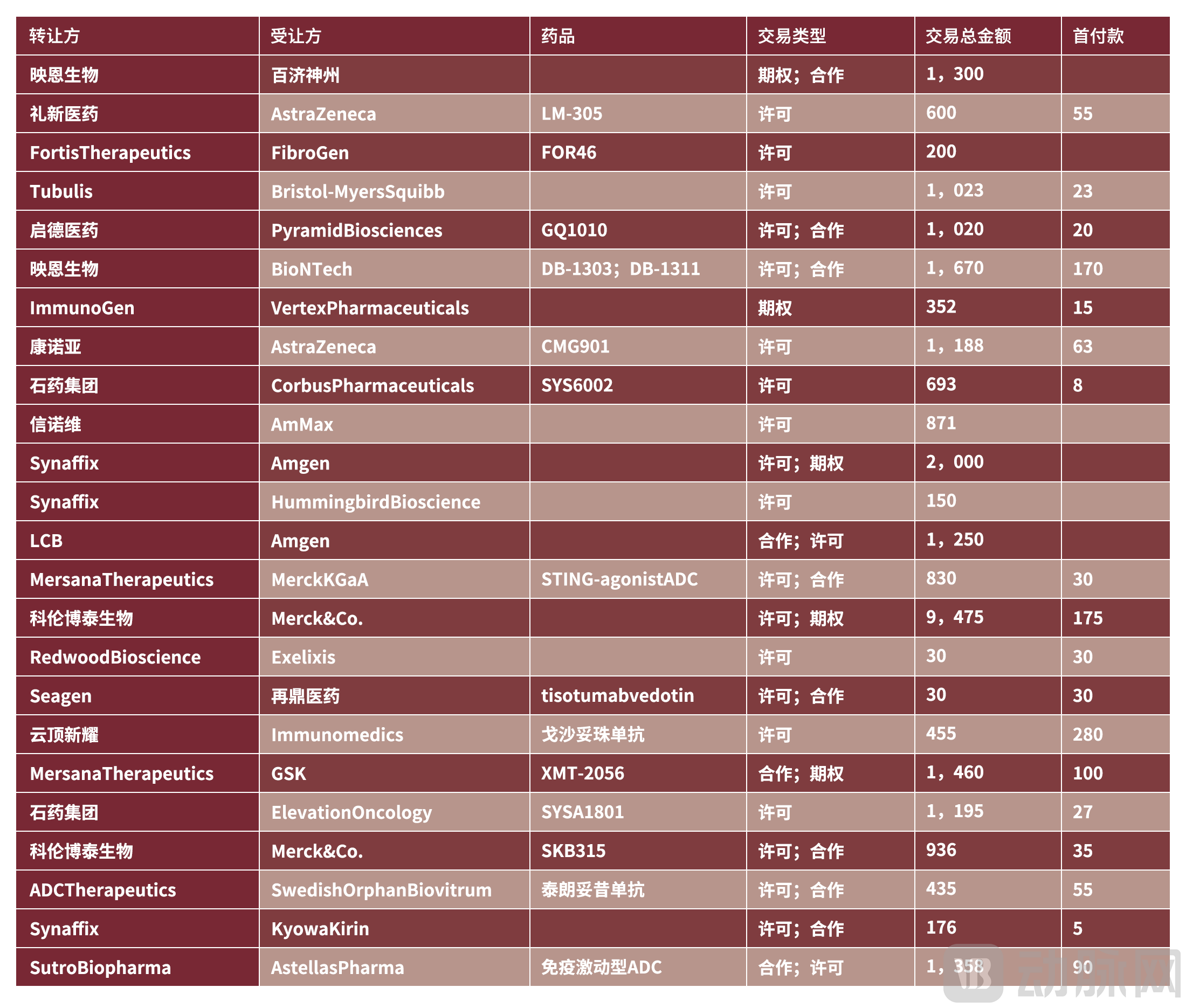
Figure 5. Recent ADC-Related Transactions(Amount: million USD | Source: PharmaCube)

Figure 6. ADC-related financing events year-to-date (Source: PharmCube)
VI. Challenges Facing ADCs
We also note that while antibody-drug conjugates (ADCs) have been developing rapidly in recent years, they face certain challenges, primarily including the following aspects:
Target Selection
Ideal targets should be highly specifically expressed on the surface of tumor cells, with low or no expression in normal cells.However, most current ADC targets are also expressed to some extent in normal tissues, which limits the maximum tolerated dose of the drug and reduces its efficacy. For example, CD30, the target of Brentuximab vedotin, is also expressed in certain normal tissues, leading to side effects such as peripheral neuropathy. Identifying highly specific tumor targets has become one of the key research focuses in current ADC development.
Tumor Heterogeneity
Tumor cells within the same tumor type exhibit high heterogeneity, with varying dependencies on drug targets across different cells.This may lead to the emergence of tumor cells that are insensitive to the drug or the development of drug-resistant cells. Ado-trastuzumab demonstrates significant efficacy in treating HER2-positive breast cancer; however, tumors with weak HER2 positivity or HER2 negativity are insensitive to it and may potentially become the dominant cell clones post-treatment. Strategies to address this issue include developing bispecific antibodies targeting multiple antigenic epitopes or enhancing the bystander effect of antibody-drug conjugates (ADCs).
Selection of Linkers
Instability of the linker can lead to drug release outside the intended site, increasing toxic side effects.Gemtuzumab ozogamicin, the first ADC to reach the market, caused severe toxicity leading to locked-in syndrome due to linker instability.An ideal linker should be highly stable in the bloodstream and rapidly cleavable within tumor cells, thereby enabling effective release of toxin molecules at the tumor site to exert cytotoxic effects. A key highlight of Enhertu lies in its novel linker design, which significantly improves blood stability and broadens the therapeutic window.
Drug Resistance of Tumor Cells
The development of ADC resistance involves multiple mechanisms, specifically including:1) Tumor cells can evade drug-induced cytotoxicity by downregulating or completely losing the target antigen recognized by the antibody-drug conjugate (ADC); 2) Within the same tumor, there exist cell subpopulations that are highly dependent on and independent of ADCs, with the latter capable of selective survival and formation of resistant clones; 3) Tumor cells can activate resistance-related pathways, such as ATP-binding cassette (ABC) transporters, to efflux the cytotoxic payload from the ADC; 4) Tumor cells can activate alternative signaling pathways to bypass the primary pathway inhibited by the ADC; 5) Some tumor cells can reduce toxin release by altering lysosomal cleavage of the linker; 6) Tumor-associated macrophages and other cells in the microenvironment can internalize ADCs, thereby reducing drug concentration.
The Impact of the Tumor Microenvironment
The tumor microenvironment, such as tumor-associated macrophages, can also affect the delivery and efficacy of ADCs.Existing studies have found that tumor-associated macrophages can engulf antibodies via Fcγ receptors, thereby reducing the efficacy of antibody-drug conjugates (ADCs). Understanding the impact of the microenvironment on drug efficacy and adopting corresponding strategies are also current research hotspots.
VII. Fund Perspectives
ADC Therapy for Tumors Has Gradually Become One of the Key Approaches in Precision Oncology.Currently, 15 ADC drugs have been approved for marketing worldwide, applied in the treatment of lymphoma, leukemia, and various solid tumors. The representative drug Enhertu has demonstrated significant improvements in survival rates and response rates in multiple clinical trials.With continuous technological optimization, the efficacy and safety of next-generation antibody-drug conjugates (ADCs) are expected to further improve,Meanwhile, factors such as tumor heterogeneity and drug resistance have also posed new challenges to the development of antibody-drug conjugates (ADCs).Future trends in the field of antibody-drug conjugates (ADCs) include developing antibodies with more diverse targets and higher specificity, designing novel linkers to enhance stability, and combining ADCs with other therapeutics to improve efficacy and overcome drug resistance.We have reason to believe that, as more products gain regulatory approval for market launch, antibody-drug conjugates (ADCs) are poised to become a primary treatment option for certain hematologic malignancies and solid tumors.
Swipe up or down to view