Tianjin Medical University General Hospital Neurosurgery Introduces Innovative PPDO-Based Craniobasal Repair Material
How difficult is it to repair a 1 cm defect?
If it were on a piece of paper, one strip of adhesive tape would be sufficient to secure a firm repair.
If the hole is on a piece of clothing, even a dexterous child can sew it up with a needle and thread.
However, if this 1-cm defect is located in the area of thinned bone at the anterior cranial fossa floor exposed via the transsphenoidal approach, repair is extremely challenging. Inadequate repair may lead to postoperative cerebrospinal fluid leakage, and even a forceful sneeze could place the patient at serious risk.
1How to Better Repair a Hole
With the continuous advancement of imaging diagnostic technologies, the detection rates of intracranial tumors such as pituitary adenomas, anterior cranial fossa meningiomas, and craniopharyngiomas have been increasing year by year. While this enables early detection and treatment for patients, it also presents new challenges in clinical practice.
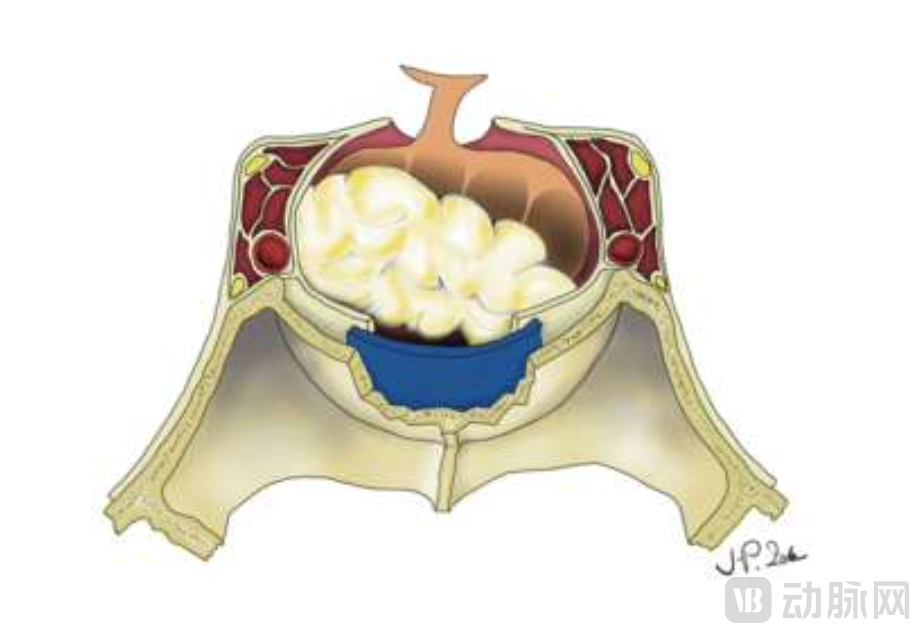
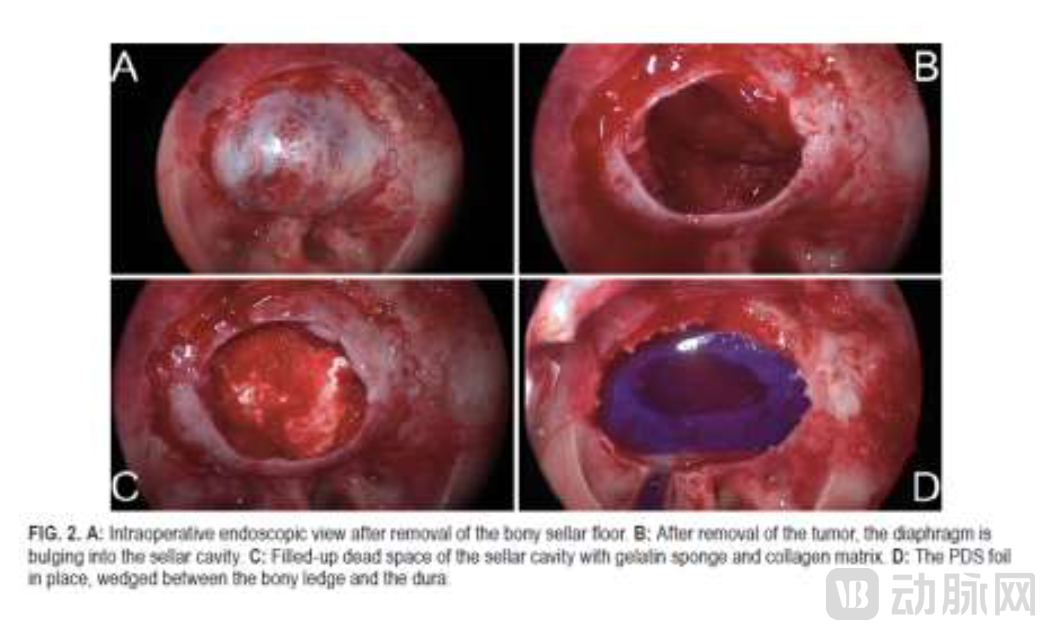
Among current surgical approaches, apart from the open craniotomy procedures traditionally perceived as requiring skull opening, the endoscopic transnasal approach is the alternative. In the endoscopic transnasal procedure, the sphenoid sinus is first accessed via the nasal cavity, followed by opening the anterior cranial base bone through the sphenoid sinus cavity to resect the lesion, and finally completing the skull base repair and reconstruction. In this final step, the most reliable method is to use rigid support materials for skull base reconstruction to repair the drilled bony defect.
The Innovation and Translation Branch of Neurosurgery [ITMNS] under the China Health Care Association for the Elderly, together with the Beijing Ensi Institute of Translational Medicine, introduced a cranial base reconstruction and repair material. Through discussions with clinical translation expert Dong Miao, Professor Yue Shuyuan, Chief Physician of the Department of Neurosurgery at Tianjin Medical University General Hospital, and Associate Professor Wang Dong, Deputy Chief Physician, they shared their insights in a highly accessible manner. Professor Yue stated that the fundamental requirements for cranial base reconstruction are, in fact, easy to understand:
1. Cerebrospinal Fluid Leak Prevention Function
2. Mechanical Support Function of the Skull Base for Overlying Tissues
Currently, the commonly used methods are relatively standardized, typically involving filling with solid materials or sealing with membranous soft tissue materials. Commonly used materials include solid fillers (autologous fat, gelatin, hydrogels, cellulose), membranous patches (autologous fascia, SIS dura mater), and rigid support materials (autologous cartilage, autologous bone), with progressively increasing hardness and toughness.
However, widespread use does not imply that these materials are flawless. Existing materials still exhibit numerous limitations in clinical practice. For instance, soft biological membranes provide insufficient mechanical support and are unsuitable for large-area skull base defects. Hard materials, typically derived from autologous cartilage, are associated with difficult harvest procedures, poor uniformity, and inadequate mechanical stability. Meanwhile, solid graft fillers lack preformed shapes, resulting in prolonged packing times and increased surgical complexity.
Demand for a novel material is spreading among neurosurgical clinicians.
2Different Questions, Same Answer
When we discuss the demand for a certain new material, the answer does not necessarily lie in a brand-new, undeveloped polymer. Reprocessing existing materials can often be a more cost-effective solution.
A marketed product from Ethicon, USA, has captured the attention of Professor Yue Shuyuan, Chief Physician of the Department of Neurosurgery at Tianjin Medical University General Hospital. As an FDA-approved soft tissue and cartilage support material for rhinoplasty, the Ethicon product is composed of polydioxanone (PPDO). It is not only hydrophobic but also exhibits an appropriate degradation profile, losing mechanical strength within two months in rats and undergoing complete degradation within six months.
Director Yue quickly recognized the advantages of PPDO material in the field of skull base repair. As a novel synthetic hydrophobic polyester polymer capable of in vivo degradation, PPDO exhibits superior biocompatibility compared to currently commonly used polyesters and can be thermally processed, facilitating its dissolution and fabrication into custom-designed shapes.

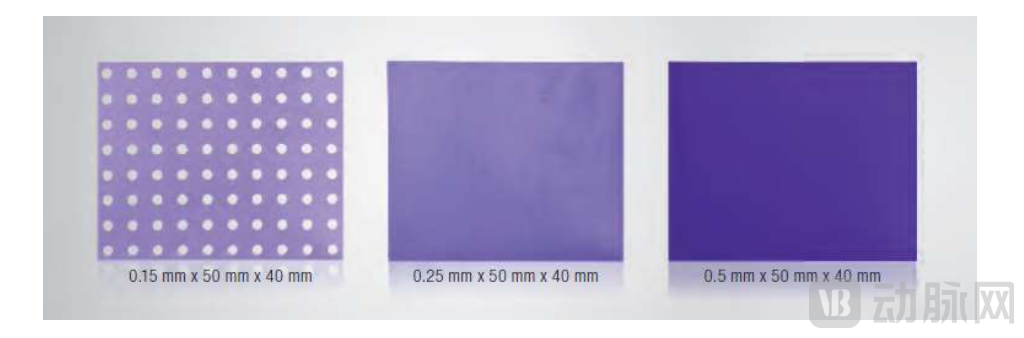
This characteristic makes sheet-like PPDO material particularly suitable for skull base reconstruction as a dural substitute, offering advantages in storage and transportation, ease of processing, and convenient intraoperative handling.
As an alternative to traditional skull base support materials, PPDO offers greater hardness and uniformity than cartilage, thereby providing stronger structural support. This enhanced support allows for larger surgical exposure areas using a drilling burr (up to 35×30 mm), enabling a wider range of device options. Additionally, preoperative shaping of the membrane can reduce operative time and lower the risk of intraoperative cerebrospinal fluid leakage and associated complications.
Building on this foundation, Director Yue also introduced improvements by testing two designs featuring perforations and protrusions, which facilitate intraoperative grasping and real-time position adjustment, thereby further enhancing convenience.
3A Doctor's Wish
With the widespread adoption and advancement of endoscopic techniques and equipment, the number of endoscopic nasal surgeries and transsphenoidal endoscopic procedures has been increasing year by year. According to Professor Wang’s estimates, currently, 2 out of every 10 skull base tumor resection surgeries are performed via the transnasal approach. If the scope of bone removal via the nasal route can be further expanded and skull base reconstruction becomes more precise and reliable, the proportion of transnasal surgeries will increase even further.
When asked about their future plans, both doctors expressed a strong desire to see this material widely disseminated, for very simple reasons.
"Truly excellent to use."
“If the wound is large, only this type of trimmable rigid support offers greater reliability.”
“With this rigid support, cerebrospinal fluid leakage is virtually eliminated.”
"Prepare in advance to significantly simplify intraoperative procedures."
“See, it can be stored in a sealed bag at room temperature.”
Each sentence squarely addresses the myriad of small yet critical challenges that neurosurgeons encounter during operations. Clinical issues must ultimately be resolved by clinicians.