MRD Commercialization Faces Three Final 'Hard Bones' to Crack

Gene+
Tumor Gene Testing Service Provider
“An increasing number of patients are proactively calling to inquire about MRD,” a professional in the field of oncology genetic testing told VCBeat. In early 2023, his company began promoting MRD in hospitals. Within a few months, it had been implemented in nearly 30 top-tier tertiary Grade A hospitals across China.
MRD, or Minimal Residual Disease detection, was initially developed as a testing method for hematologic malignancies to help monitor the risk of recurrence in patients who had undergone curative treatment. Around 2015, some teams attempted to apply this logic of residual disease detection to monitor recurrence in early-stage cancer patients who had received curative surgery, thereby opening up new possibilities. Since 2020, major domestic tumor NGS companies have successively launched MRD products, competing for the postoperative tumor market.
However, during that period, MRD technology itself was not yet mature, clinical evidence was limited, and the overall pace of commercialization was slow. If MRD were only used to predict the risk of recurrence, its clinical value would undoubtedly struggle to meet market expectations. The greater potential for MRD lies in guiding decisions on treatment selection.
In recent times, domestic and international manufacturers have engaged in fierce competition, with MRD clinical research cohorts being launched in succession. An increasing number of clinical application scenarios for MRD have been validated through practice. Meanwhile, MRD has been progressively incorporated into clinical guidelines and expert consensus statements, thereby becoming integrated into the treatment workflows for cancer patients.
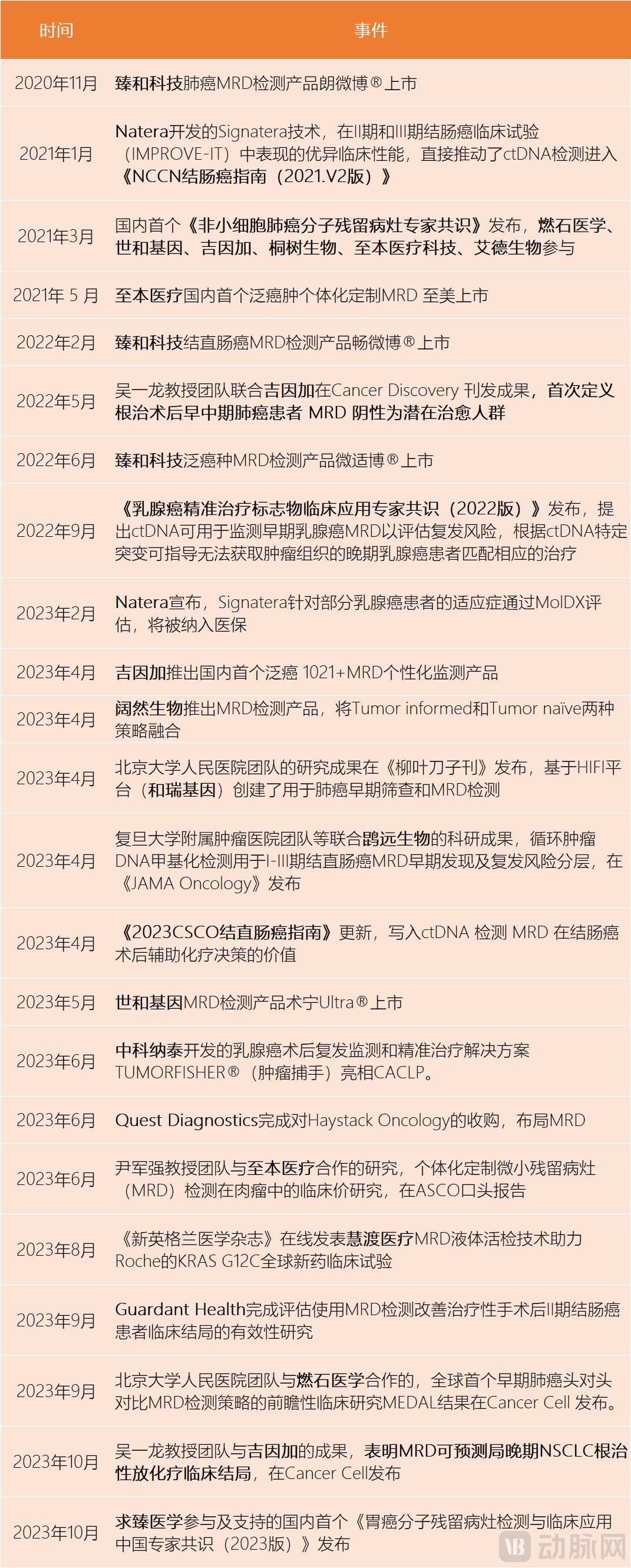
Key Milestones in the MRD Field Since 2020 (in Chronological Order)
Since the beginning of 2023, clinical evidence related to minimal residual disease (MRD) has been published intensively, covering various decisions in the clinical diagnosis and treatment of cancer. After years of betting on MRD, the tumor genetic testing industry has finally ushered in a window of opportunity for the commercialization of MRD. Meanwhile, the long-quiet domestic tumor next-generation sequencing (NGS) market appears poised for an imminent showdown.
In a sense, the commercial application of MRD has exceeded manufacturers’ expectations, becoming an outlet for recurrence anxiety among patients with early-stage cancer. “Many cancer patients today are highly capable learners; they read clinical guidelines on their own and familiarize themselves with both conventional and innovative diagnostic and treatment approaches,” Lu Leilei, Chief Operating Officer of Geneseeq Technology, told VCBeat. “However, overall, the clinical application of MRD is a matter of great seriousness.”
“At present, MRD testing is more commonly used in clinical practice for patients with early-stage breast cancer.” Another industry practitioner also highlighted the early adoption of MRD among tumor patients. Among several types of malignant tumors with high incidence rates in China, breast cancer possesses characteristics that are conducive to the promotion of MRD. First, the prognosis is relatively favorable, with a five-year survival rate for early-stage breast cancer approaching 90%. Second, there is a slightly higher proportion of younger women among patients, who tend to have higher levels of education and place greater emphasis on their health. They are more inclined to pursue complete cure through rigorous and cautious treatment.
Research indicates that tumors are composed of many distinct populations of cancer cells, each harboring dynamically evolving genomes. The greater the diversity of these tumor cell populations, the higher the likelihood of cancer recurrence within one year following treatment. “The profound fear and uncertainty associated with malignant tumors stem from the persistent risk of recurrence and metastasis, even after patients have undergone highly standardized curative surgery,” stated Dr. Wang Dongliang, Chief Medical Officer at Gene+ (Ji Yin Jia).
As part of standardized treatment, cancer patients are required to undergo regular follow-up examinations to manage the risk of recurrence. Such assessments undoubtedly pose a significant challenge for cancer patients. After all, once a recurrence progresses to a tumor detectable by medical imaging, management may become more complex than at initial diagnosis.
MRD provides a tangible representation of the tumor recurrence timeline, thereby alleviating excessive anxiety for some patients with early-stage cancer. Based on historical testing data, the MRD positivity rate among early-stage patients is approximately 10%, while it reaches about 50% in patients with stage III lung cancer.
“Our research found that among early-stage lung cancer patients who underwent curative surgery, the peak incidence of MRD positivity occurred 18 to 24 months postoperatively,” Gong Yuhua told VCBeat. Over the past six years, Gene+ has conducted extensive clinical studies on minimal residual disease (MRD) to examine the relationship between MRD dynamics and the progression of various tumors. In another study, the Gene+ team discovered that tumor patients with postoperative MRD positivity typically experienced recurrence within 6 to 9 months after the positive result was detected.
Of course, prognostic assessment represents only a small fraction of the clinical value of MRD. More importantly, MRD should provide physicians with more personalized information regarding patients’ disease status. Given that tumors are constantly evolving and changing, continuous MRD monitoring is essential to generate a sufficiently robust volume of informative data.
In clinical practice, a portion of the tissue resected during surgery serves as the baseline sample for minimal residual disease (MRD) analysis, undergoing whole-exome sequencing or deep sequencing covering a large number of genetic loci. Subsequently, patients typically undergo their first blood draw between one week and one month postoperatively. Follow-up blood samples are then collected every 3 to 6 months, adjusted according to the tumor-specific release kinetics, for dynamic monitoring of specific locus panels. The 2021 "Expert Consensus on Molecular Residual Disease in Non-Small Cell Lung Cancer" recommends close follow-up management for NSCLC patients with positive MRD results after surgery, suggesting MRD testing every 3 to 6 months.
Unlike companion diagnostics, which typically require only a one-time test, MRD fosters closer collaboration between users and vendors. As the highly uncertain early-stage R&D phase nears its end, the competition to navigate the future commercialization path may pose an even greater challenge for oncology NGS companies. But that is a story for another time.
MRD has long been held in high regard by the industry. Among the three major application scenarios of tumor NGS, MRD represents the fastest-growing and most promising segment. According to Frost & Sullivan data, the market size for cancer prognosis and monitoring in China increased from RMB 64.9 million in 2018 to RMB 600 million in 2022, representing a nearly tenfold growth. This rapid expansion is expected to continue for at least the next 3–5 years.
Over the past two years, the prosperity of China’s MRD industry ecosystem has been evident.
First, the spectrum of cancer types covered by MRD is rapidly expanding. TechFrom a technical perspective, MRD monitoring can be performed for any tumor type; however, cancers with higher mutational burdens allow for more sensitive MRD tracking. For tumor types with insufficient tracking loci, MRD monitoring can be achieved by adjusting the panel size or by tracking a greater number of clonal variants. “Of course, clinical need is the most critical determining factor—for instance, whether there are sufficient treatment options available to alter the patient’s disease course based on MRD results, thereby delivering overall benefit,” stated Du Bo, founder of Zhenhe Technology.
Previously, breast cancer was not a key focus for domestic MRD manufacturers, given the relatively long disease-free survival period following radical mastectomy and the more established standardized treatment protocols. However, as interventional studies in breast cancer have demonstrated the clinical value of MRD, product development in this field has also gained momentum.
Secondly, MRD at the current stage can already meet the monitoring needs throughout the entire course of cancer.For patients with early-stage tumors, MRD can be used to adjust subsequent treatment plans. Studies have shown that postoperative MRD testing can guide therapy: if residual disease is detected, patients may receive more intensive adjuvant therapy, whereas those who are MRD-negative may be spared such treatment. “It is worth noting that for tumor patients who consistently test negative for postoperative MRD, adjuvant therapy after surgery may still be omitted, even if their clinical stage has progressed to Stage II or III,” pointed out a practitioner.
For advanced metastatic tumors, a broad definition of MRD is adopted to evaluate treatment efficacy by assessing molecular residual disease. This approach is necessary because any given drug may be ineffective in a subset of patients. Typically, treatment response is assessed 6–8 weeks after initiating therapy by re-evaluating medical imaging to monitor changes in lesion size. However, with MRD testing, blood samples can be collected at a specified time after the first treatment cycle to predict whether the patient will benefit. This strategy not only reduces the waiting period for patients but also mitigates the risk of tumor progression during that interval.
“In fact, as long as a tumor exhibits uncontrolled growth, MRD holds certain clinical significance,” stated Dr. Wang Dongliang.
Third, accuracy has improved significantlyAfter years of development, mainstream MRD technologies have managed to control the false-positive rate at a low level while ensuring sufficiently high confidence in negative results. “From a technical development perspective, MRD detection aims to determine the presence or absence of very low-frequency tumor-derived ctDNA, which places high demands on detection technology,” Chen Weizhi, Chief Scientific Officer at Zenith & Beyond (Zhenhe Technology), told VCBeat. “On NGS platforms, technical noise and biological noise are the primary technical challenges when detecting very low-frequency signals. On the basis of ensuring the specificity of the detection technology, improving the sensitivity of MRD detection has always been a key challenge that major platforms strive to overcome. For instance, Kuoran Biology has launched Tumor-informed + Tumor-naive MRD testing products, which combine the advantages of both strategies. This approach not only enables personalized customization and precise MRD monitoring but also detects other hotspot mutations, significantly reducing the likelihood of false-negative results caused by tumor heterogeneity.”
“Based on recent clinical practice, patients with early-stage tumors who undergo surgery and test negative for MRD postoperatively indeed have a very low risk of recurrence in the short term,” summarized Dr. Dongliang Wang. He noted that it is generally possible to assure patients with confidence that if they undergo MRD testing through mainstream industry companies and receive a negative result, their risk of recurrence over the next 3–6 months is typically below 5%.
"As one of the first companies in China to strategically position itself in the MRD field, Gene+ initiated its project in 2015 and launched its first-generation product in 2017. 'The entire process was fraught with uncertainty; it was not until around 2019 that expert consensus statements began to emerge,' Gong Yuhua told VCBeat. 'Since then, both physicians and patients have gradually come to accept MRD.' She has observed that, particularly over the past two years, acceptance of MRD has continued to rise: patients are proactively inquiring about MRD-based products, while physicians generally understand and recognize the clinical value of MRD and are willing to adopt it."
“In formal hospitals, oncologists will definitely attach importance to this result, as it has become a widely accepted consensus,” said Zhang Lijun, Senior Director of Medical Strategy at Zhenhe Technology. As for whether clinicians will directly adjust treatment plans based on MRD test results, he believes that this is not yet certain. Physicians require more comprehensive and higher-level evidence to guide treatment decisions, and many prospective interventional studies on MRD are still ongoing. “However, doctors will explain the pros and cons to patients based on MRD test results and respect their choices.”
Returning to Commercialization: The Realistic Dilemmas of MRD Are Evident. As a product designed for the entire course of oncology care, MRD currently has a very niche active user base.
According to incomplete statistics from VCBeat, MRD products currently on the market are priced at an average of approximately RMB 15,000. Based on a market size of RMB 600 million in 2022, even with rapid market penetration, the annual number of MRD tests conducted in China amounted to only 40,000, representing a very small proportion of the vast population of new and existing cancer patients.
For MRD to achieve widespread clinical adoption, challenges at both ends of the spectrum must be addressed. One end is linked to clinical practice: how to interpret and apply patients’ MRD monitoring results. This tests not only the clinicians who make direct treatment decisions but also the developers of MRD products. The other end is tied to technology: ensuring that MRD test results accurately reflect the level of minimal residual disease in cancer patients, while keeping costs under control. As the concept of MRD testing becomes increasingly prevalent, this accuracy should be regarded as the foundational cornerstone of any MRD product.
First, compared with the potential clinical value of MRD, the accumulation of existing research data is still very limited.In theory, MRD can provide clinical information at least equivalent to that of medical imaging. Based on qualitative or quantitative MRD results, clinicians can make decisions regarding various aspects of oncology treatment, such as whether postoperative patients should receive chemotherapy, whether patients undergoing chemotherapy should discontinue treatment, and whether patients currently in treatment should switch regimens.
However, existing clinical research evidence is insufficient to support the realization of these clinical values by MRD, or the experiments designed to verify certain clinical values of MRD are difficult to implement in practice. For instance, in clinical practice, many patients with early-stage lung cancer or colorectal cancer receive adjuvant chemotherapy after curative resection. In reality, however, such chemotherapy offers very limited benefits in terms of reducing recurrence rates and extending survival for a subset of patients. Although some studies have indicated that postoperative chemotherapy may even be associated with a higher risk of recurrence in MRD-negative patients, direct research evidence supporting the discontinuation of chemotherapy based on MRD status remains very limited.
Second, it remains difficult to determine at which stage of clinical oncology diagnosis and treatment MRD should be incorporated.Theoretically, MRD positivity is not equivalent to tumor recurrence or metastasis. Data indicate that it remains unclear whether MRD positivity leads to clinical manifestations, or how long it may take for such manifestations to appear—ranging from as short as three months to six months or even a year. Clinically, there is no consensus yet on the subsequent management of MRD-positive cases.
“Currently, it depends on the clinician’s understanding and practice style,” said Dr. Lu Leilei. Physicians who are more familiar with minimal residual disease (MRD) or who adopt a relatively aggressive treatment approach may directly escalate therapy based on MRD-positive results, while others may recommend additional tests, such as PET-CT, to comprehensively evaluate the findings. “This scenario is more common among breast cancer patients.”
Third, the existing regulatory environment remains unclear on how to approve innovative medical devices such as MRD.This is also the biggest challenge facing the clinical penetration of MRD. “It’s not that doctors are unwilling to accept it; rather, they hope to adopt this advanced technology under more compliant conditions,” pointed out Du Bo. He noted that since there are currently no compliant MRD products available in China, even if physicians believe patients may benefit, they still have reservations about their actual use.
“While the clinical penetration rate of MRD will certainly increase compared to the past, it remains very low when calculated against the proportion of millions of newly diagnosed and existing cancer patients each year,” stated Dr. Wang Dongliang. The fundamental reason is that although leading tumor NGS companies in China have generated certain clinical evidence through relevant studies, they have not yet received regulatory approval or reimbursement support as seen in the United States; thus, related enterprises still need to make further efforts.
The threshold for commercializing MRD products is extremely high. From product design to clinical validation, it requires sustained investment of substantial clinical resources and R&D funding. The product registration process further demands long-term, iterative communication with regulatory authorities, necessitating time for accumulation. “We need to be even more patient in refining our products,” lamented Lu Leilei.
As more potent new treatment regimens continue to emerge, malignant tumors are becoming—and will ultimately become—chronic diseases with which humans can coexist. We look forward to the day when minimal residual disease (MRD) monitoring for malignant tumors becomes as routine and essential as blood glucose monitoring for diabetes or blood pressure measurement for hypertension, serving not only as an effective surveillance tool but also as a constant companion in patient care.