MRI-Guided Temporal Interference Stimulation Targeting the Fastigial Nucleus: A Standardized Protocol for Post-Stroke Balance Rehabilitation

Neurodome
Neurodome, Inc.
High incidence of lower limb motor dysfunction and balance instability after stroke; conventional rehabilitation and traditional non-invasive brain stimulation struggle to precisely modulate the fastigial nucleus (FN) responsible for balance and coordination.Transcranial Temporal Interference (TI) stimulation can non-invasively focus on deep brain regions.However, there is currently a lack of standardized implementation processes for stroke populations. Recently,Professor Gao Qiang from West China Hospital of Sichuan UniversityTeam CollaborationProfessor Tian Liu from Xi'an Jiaotong UniversityThe team published a study in the "Journal of Visualized Experiments,"A standardized protocol for TI-targeted FN based on individualized MRI guidance and modeling was proposed for the first time.The system verified the repeatability, precise targeting, and clinical safety of the procedure, providing a standardized technical model for non-invasive deep brain neuromodulation in stroke-related balance disorders.
TI stimulation via two pairs of scalp electrodesEnter separatelyTwo high-frequency currents (I₁, I₂),There is a relationship between the two currents.Tiny frequency difference,Two sets of oscillating electric fields (E₁, E₂) are formed in the brain (Figure 1). The two sets of electric fields interfere and superimpose in the deep target area, generatingLow-frequency Amplitude Modulation (AM) Envelope Electric Field.Deep neurons are sensitive to low-frequency envelope components, while the superficial cortex responds weakly to high-frequency carriers, thus achievingSelective activation of deep neurons, avoiding superficial cortex,Achieve precise regulation under non-invasive conditions.
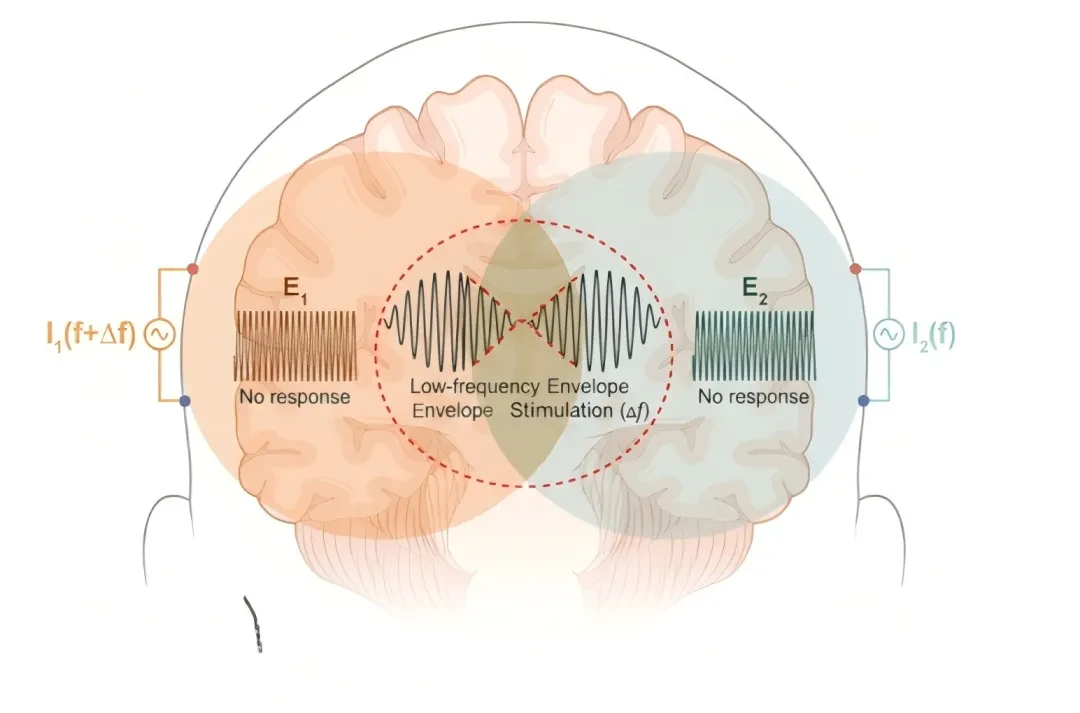
Figure 1. Schematic diagram of TI stimulation
Subject Screening and Preparation
Strictly exclude individuals with intracranial metal implants, epilepsy, skull defects, severe heart, liver, or kidney diseases, and mental disorders; evaluate history of head trauma and medication use through a non-invasive brain stimulation safety questionnaire. Adhere to the Declaration of Helsinki and sign the informed consent form. Collect1mm high-resolution T1-weighted MRI (SNR≥20),If necessary, supplement with T2 or CT to clearly display the posterior cranial fossa structures, laying the foundation for individualized modeling.
Individualized Target Localization and Model Construction
Based on MRI ReconstructionIndividualized Head Model,Automatically segment into six types of tissues: scalp, skull, cerebrospinal fluid, white matter, gray matter, and lesion area, and assign conductivity values;Using Neurodome's NervioWeb simulation modeling softwarePerform modeling and simulation;ThroughFinite Element MethodGenerate mesh and solve for electric field distribution.The Culmen of the Cerebellum in Standard Brain Atlas via Nonlinear RegistrationMapped to individual space for precise target localization. Set TI optimization parameters (including FN coordinates, current constraints, focusing optimization mode) and output only whenEffective Electrode Arrangement, Current of Each Channel, and Maximum Electric Field Envelope in the Target AreaThe optimization was successfully confirmed at the time (Figure 2).
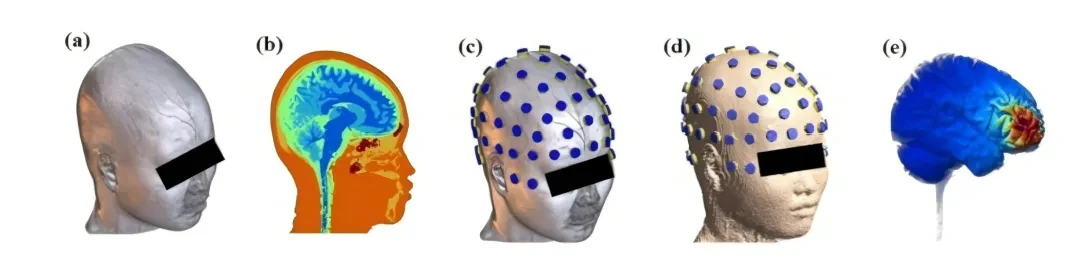
Figure 2. Subject-specific electric field simulation process (A) T1-weighted MRI acquisition; (B) Tissue segmentation; (C) 10-10 EEG electrode registration; (D) Tetrahedral finite element mesh generation; (E) Intracranial electric field distribution calculation.
Optimization and Implementation of Stimulation Parameters
Two pairs provide high-frequency carrier current(2 kHz and 2.005 kHz)The electrodes are placed on the occipital scalp, byNeurodome's NervioX-1000 StimulatorDrive (Fig. 3A). Simulation phase requirementsFN area electric field strength > 0.2 V/m and deep/cortical electric field ratio > 3:1,Ensure deep focusing and low superficial stimulation. Optimize electrode arrangement and current ratio based on the 10-10 EEG system. In actual operation,Electrode impedance is strictly controlled to be <8 kΩ,Good contact ensured by scalp abrasion and conductive gel; before stimulationLow-intensity pre-stimulation assessment of tolerance,Real-time monitoring of impedance and adverse reactions throughout the procedure. The study adoptedRandomized, double-blind, sham-controlled design,The sham stimulation group completely simulated the real process to maintain the effectiveness of blinding.
Electric Field Simulation Verification: Deep Targeting with Precision and Controllability
High-resolution T1 MRI successfully achieved six-class tissue segmentation and supported electrode arrangement optimization (Fig. 3A). Simulations showed that although the high-frequency carrier electric field was strong in the superficial layer,Low-frequency AM envelope electric field precisely focuses on the FN core region(Figure 3B),Electric field intensity in FN region > 0.2 V/m,Confirm that the process can be stably achieved.Deep targeting while avoiding excessive stimulation of superficial layers.
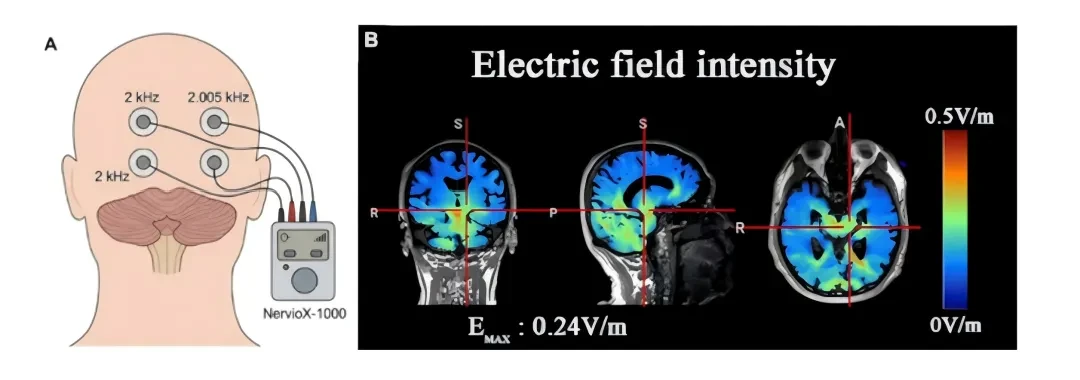
Figure 3. Standard head model simulation of electric field intensity (A) Schematic diagram of optimized electrode arrangement (occipital electrodes, NervioX-1000 driver); (B) Electric field intensity distribution in the target area (EMAX: maximum electric field in the target area).
Multi-dimensional Experimental and Computational Evidence
Multiple studies have consistently confirmed that TI can precisely target deep brain regions (Figure 4): Violante et al. found,Hippocampal-targeted TI stimulation modulates BOLD responses, enhances episodic memory, and does not activate superficial cortical layers.(Figure 4A); validated in rodent studies,TI can selectively modulate hippocampal γ oscillations while preserving the superficial cortex.Confirm the "penetration" characteristics of high-frequency carriers (Figure 4B); Missey et al. confirmed,TI can promote memory encoding only when the stimulation frequency matches the rhythm of the target network.(Figure 4C); further research on motor regulation shows,Striatal-targeted TI improves motor skills and Parkinson's disease-related tremors, while lower limb cortical TI enhances motor abilities.(Fig. 4D-F).
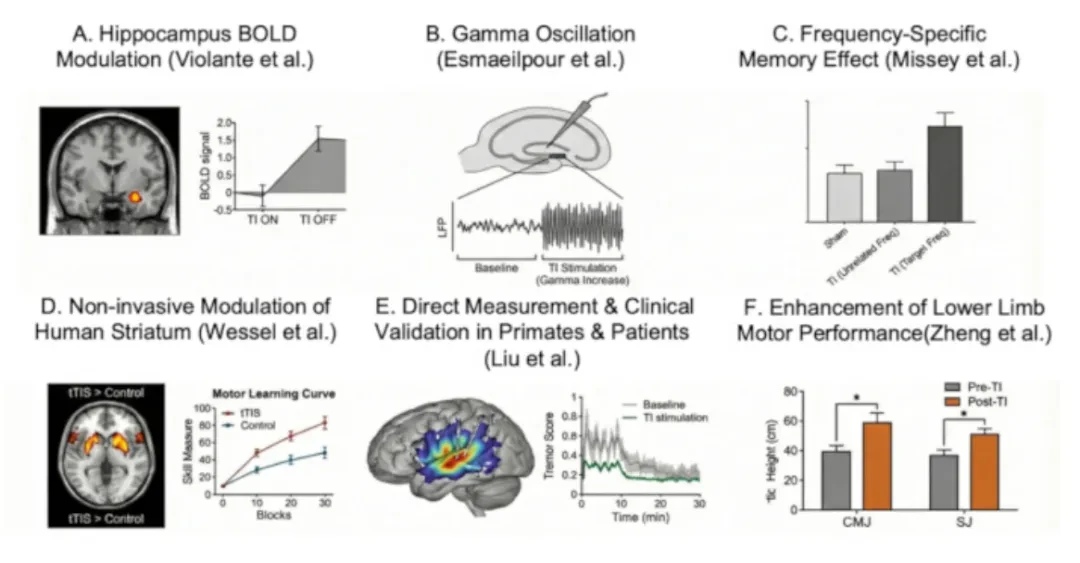
Figure 4. Representative findings from previous TI studies (A) Hippocampal BOLD and memory modulation; (B) Selective modulation of hippocampal γ oscillations; (C) Frequency-dependent memory encoding; (D) Striatal motor regulation; (E) Validation of deep electric fields in primates; (F) Improvement in lower limb motor function.
This study calculates simulation and in vivo validation
The research team's computational simulations have simultaneously confirmed,Optimized TI stimulation can precisely focus the electric field on FN.(Figure 5); currently being utilizedIntracranial Stereoencephalography in Epilepsy Patients(SEEG) recordings to further validate the in vivo physiological effects of the stimulation field.
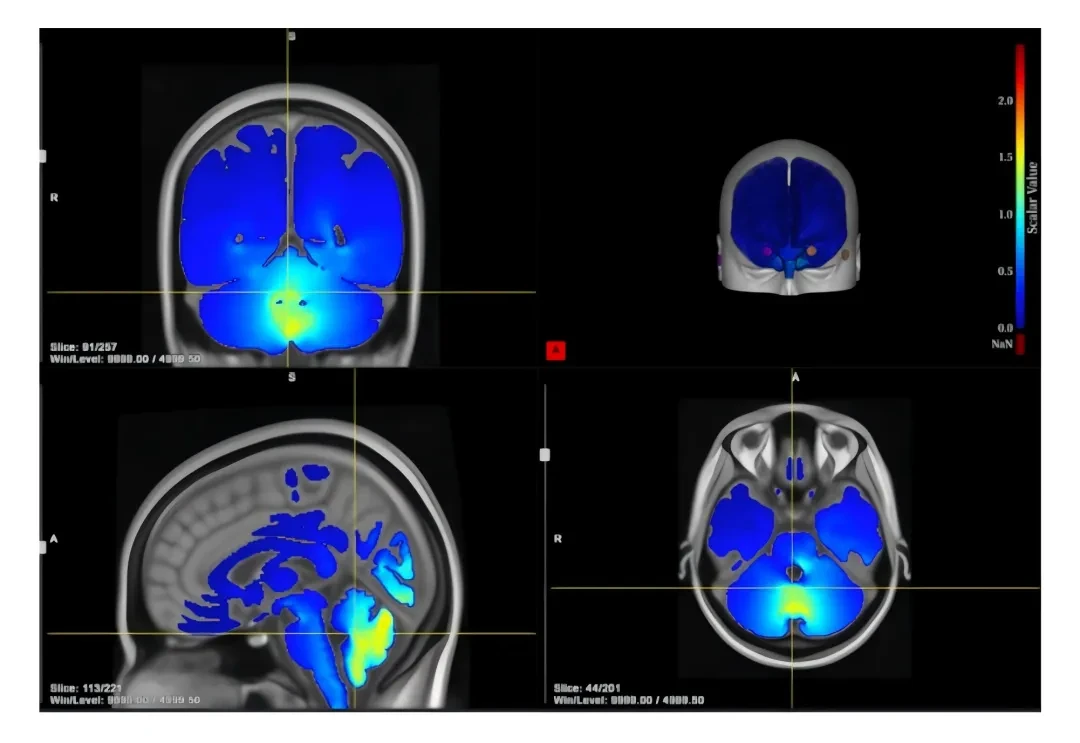
Figure 5. Cerebellar FN-targeted TI stimulation simulation on a standard head model shows that the dual-electrode configuration (P9/O9: 2.0 mA; FT10/O10: 1.292 mA) can precisely focus on the FN target.
Summary
The studyA standardized protocol for TI-targeted FN guided by individualized MRI modeling was first established for the stroke population.The system is solved.Inaccurate deep nucleus localization, electric field diffusion, and challenges in individualized adaptationSuch critical challenges. The entire solutionStandardized operation, precise targeting, and controllable safety,Provide a non-invasive deep modulation pathway for balance disorders after stroke, and also lay a methodological foundation for the study of cerebellar-related diseases such as ataxia.
References
He L, Wei Y, Gao C, et al. Magnetic Resonance Imaging-Guided Temporal Interference Stimulation of the Cerebellar Fastigial Nucleus in Stroke Patients for Balance. J. Vis. Exp. 2026; e70982.



Contact Consultation

WeChat Official Account
Neurodome
Pioneer in Non-Invasive Deep Brain Neuromodulation

Phone 400-629-2019
Email info@neurodomers.com