Sequana Medical Submits IPO Prospectus Highlighting alfapump® and DSR® Platforms for Refractory Fluid Overload

Sequana Medical
Developer of Antidiuretic Fluid Overload Treatment Solutions
Fluid overload is a common and serious clinical complication in patients with liver disease, heart failure, and cancer, leading to increased mortality, recurrent hospitalizations, severe pain, dyspnea, and limited mobility.
Although diuretics are the standard treatment, many patients have developed resistance to them. Surgical interventions such as paracentesis and transjugular intrahepatic portosystemic shunt (TIPS) can further alleviate the condition, but they are invasive, cumbersome, and carry a risk of complications. Currently, there are limited effective therapeutic options for fluid overload, leading to suboptimal clinical outcomes, high costs, and a significant negative impact on patients' quality of life.
After recognizing the urgent need for innovative breakthroughs to overcome bottlenecks in the management of fluid overload, a healthcare company based in Zurich, Switzerland, entered the field. Founded in 2006, Sequana Medical is a medical device company specializing in the treatment of resistant fluid overload and is listed on Euronext Brussels (stock code: SEQUA.BR).
Currently, based on the severity of ascites, common treatment methods include oral diuretics, therapeutic (large-volume) paracentesis, transjugular intrahepatic portosystemic shunt (TIPS), and liver transplantation; however, all current treatments have varying degrees of limitations or side effects.
The efficacy of diuretics and a salt-restricted diet in the treatment of malignant ascites is limited. Furthermore, high-dose diuretic therapy may induce renal hypoperfusion, impair glomerular function, thereby increasing renal burden and leading to renal insufficiency or even renal failure. It is estimated that 40% of patients with heart failure develop diuretic resistance or intolerance. Once this occurs, or if renal failure begins to develop, clinical alternative options become very limited and exhibit significant constraints.
The use of intraperitoneally injected chemotherapy agents may prevent ascites accumulation; however, this symptomatic relief is often temporary, and ascites will inevitably recur, potentially necessitating surgical intervention for further symptom management.
When pharmacological therapy and dietary restrictions are no longer effective, a common treatment is paracentesis, an invasive procedure that involves inserting a large-bore needle into the abdomen to drain fluid over several hours. Paracentesis removing more than 5 liters of fluid is termed large-volume paracentesis (LVP). Although LVP is generally considered safe, it is a painful and cumbersome process that provides only short-term symptom relief, as repeated procedures are required when ascites reaccumulates.
For patients with refractory hepatic ascites, in addition to repeated large-volume paracentesis (LVP), another treatment option is transjugular intrahepatic portosystemic shunt (TIPS). TIPS redirects a significant portion of blood flow around the damaged liver back into the main vasculature. However, the reduced blood flow through the liver impairs its ability to filter toxic substances from the blood, thereby increasing the risk of hepatic encephalopathy. This risk further escalates with advancing age. Consequently, TIPS poses substantial risks for patients over 65 years of age.
However, for those seeking liver transplantation, the primary challenges are the severely limited supply of donor livers and the prohibitive medical costs. Furthermore, patients must take immunosuppressive medications for life to mitigate the risk of graft rejection by the recipient’s immune system.
To address the drawbacks of current treatment methods, Sequana Medical has dedicated nearly 20 years to developing an innovative implantable micro-pump system for managing fluid balance in the body: alfapump.®and DSR®It is Sequana Medical’s proprietary system, designed to work in synergy with the human body to treat diuretic-resistant fluid overload, enabling patients to avoid invasive surgical procedures and return to a normal life.
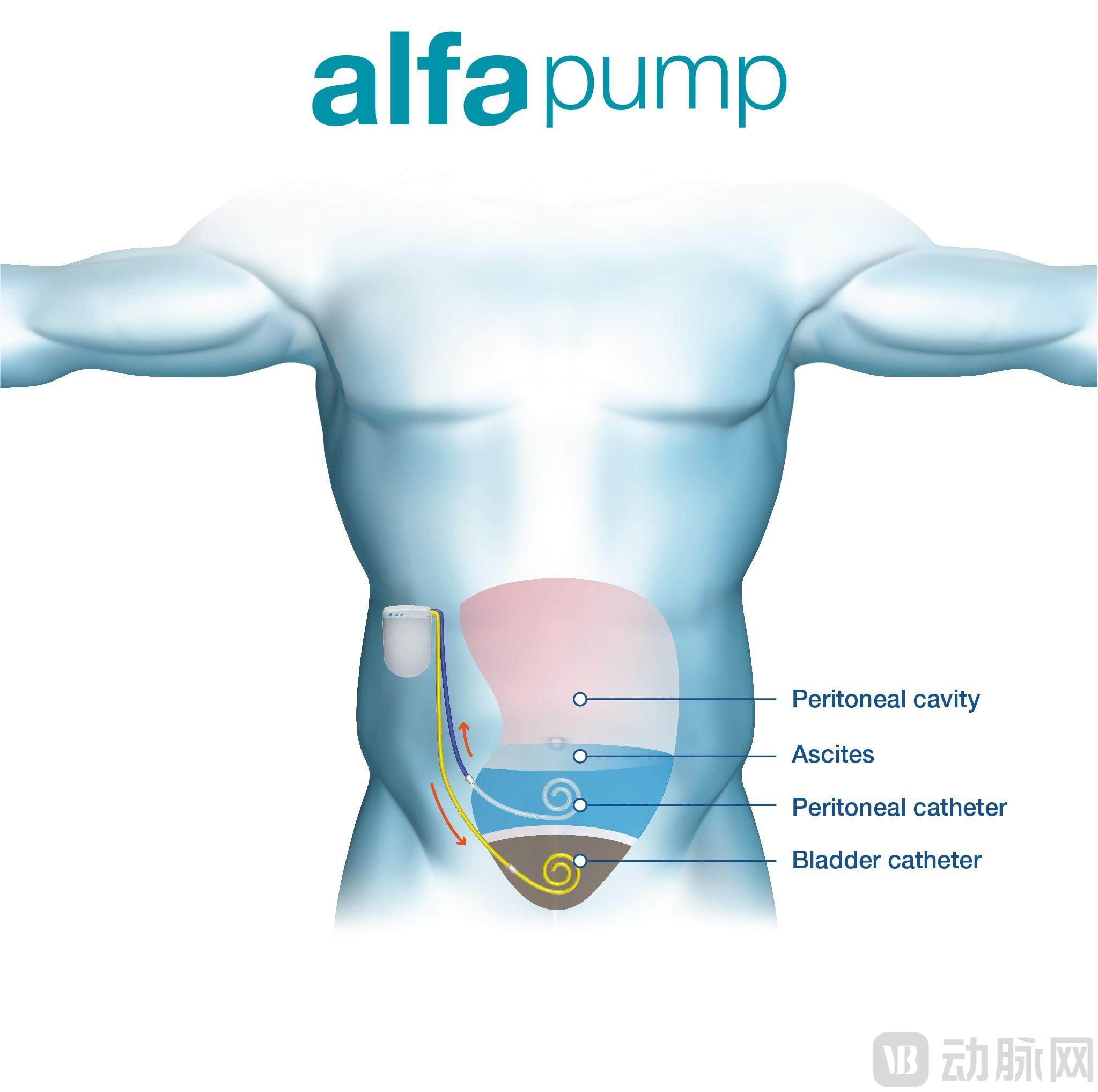
alfapump®It is one of the first medical devices designed for the treatment of ascites. It is a battery-powered micro pump that continuously and controllably drains ascitic fluid from the peritoneal cavity into the bladder, from where it is excreted from the body. As an automated drainage system, alfapump®Eliminates the need for repeated invasive procedures, requiring no needles, external tubing, or repeated punctures.
in alfapump®Sequana Medical has invested significant R&D efforts into the precise operation of its pump and control device, enabling the system to be programmed, charged, and monitored wirelessly.
alfapump®It is a fully implantable system that can be implanted subcutaneously in patients via minimally invasive surgery. The procedure is simple and short, typically requiring only 30 to 60 minutes, and can be performed under local anesthesia. Thanks to its fully implantable nature, patients can maintain normal mobility and activity levels without the need for repeated hospital visits for puncture-based treatments. After the patient receives the alfapump implant®Afterward, the physician will perform wireless programming to ensure optimal daily fluid drainage. The specific schedule can be tailored to the patient’s individual daily routine.
alfapump ®Can be implanted via minimally invasive surgery
alfapump®Wireless charging can be performed transcutaneously. Therefore, the only task required of patients is to charge the battery through the skin for approximately 20 minutes daily using a wireless charger (smart charger). Once fully charged, the battery can pump up to 4 liters of ascitic fluid. The system monitors bladder and intraperitoneal pressures via pressure sensors to ensure optimal fluid management and incorporates an anti-occlusion control algorithm.
alfapump ®The system’s proprietary DirectLink technology enables physicians to remotely monitor pump performance. During charging, the alfapump®The data is transmitted to the smart charger, and then wirelessly transferred via mobile network to a secure server for 24/7 analysis using DirectLink technology. Sequana Medical’s data specialists receive pump performance information (such as output volume and charging status) and report it to clinicians, enabling them to monitor changes in pump performance data more closely and manage patients more effectively.

alfa Pump®Enables 24/7 continuous monitoring
The concept of alfapump® dates back to 2000, originating from physicians’ need to find new treatments for ascites.
2005, alfapump®the first prototype was unveiled, validating its technical feasibility. In 2008, the first patients received implants of the device. In 2011, alfapump®Received the CE mark for the treatment of refractory ascites in liver cirrhosis. In 2012, alfapump®Commercially launched at the EASL Congress, and received CE marking for malignant ascites removal in the same year.
Thereafter, Sequana Medical continued to invest in the alfapump.®in clinical, technical, and commercial development, the Company completed the MOSAIC IDE feasibility study in North America for patients with recurrent refractory ascites due to liver cirrhosis, and announced the results of the European randomized controlled trial as well as preliminary findings from the post-marketing surveillance registry for patients with refractory ascites due to liver cirrhosis.
Following these studies, the alfapump® received recognition from key independent third parties in Europe and was incorporated into the EASL (European Association for the Study of the Liver) Clinical Practice Guidelines on decompensated cirrhosis, the German DGVS Guidelines for the Treatment of Complications of Liver Cirrhosis, and the UK NICE Interventional Procedures Guidance, for the treatment of refractory ascites caused by liver cirrhosis. In January 2019, the U.S. FDA granted the alfapump®Breakthrough Device Designation for the Treatment of Recurrent or Refractory Hepatic Ascites.
In 2017, Sequana Medical collaborated with Dr. Jeffrey Testani, Associate Professor at Yale University, to develop the DSR.®(Direct Sodium Removal) Technology. This is a breakthrough therapy for treating fluid overload in patients with congestive heart failure. It reduces bodily water content by directly removing sodium ions from the blood, thereby lowering fluid osmotic pressure. This technology avoids the use of medications such as diuretics, reduces the burden on the kidneys, and improves symptoms and prognosis in heart failure patients.
As a “sodium-free solution,” DSR®It will be infused into the patient’s abdomen and remain there for a certain period. Since the sodium concentration in the blood is much higher than that of DSR®The sodium concentration in the infusion solution; sodium diffuses from the peritoneal cavity wall into the DSR.®Infusion solution, resulting in DSR®The sodium content in the infusion fluid gradually increases. During this process, blood circulation maintains a high serum sodium concentration to facilitate sodium movement. Finally, remove the DSR.®The product and extracted sodium can complete the treatment.
2020, Single-Dose DSR®Preclinical and clinical proof-of-concept data for the therapy were published in *Circulation*, a high-impact cardiovascular journal. In May 2021, Sequana Medical reported the top-line results of RED DESERT, a study utilizing the first-generation DSR®Product (DSR 1.0): Repeat Dosing of DSR in Heart Failure Patients with Diuretic Resistance®Proof-of-concept study of the therapy. Building on the success of RED DESERT, the company initiated the SAHARA study in diuretic-resistant heart failure patients with persistent congestion and reported positive top-line data in November 2022.
First-Generation DSR®Clinical proof-of-concept studies conducted on the product (DSR 1.0) demonstrated that DSR®It can safely, effectively, and rapidly eliminate fluid overload in patients with heart failure, improve cardiac health, protect renal function, and restore the kidneys’ natural ability to manage fluid and sodium, thereby substantially and sustainably reducing the need for diuretic medications. In patients undergoing DSR®Among the treated patients, no subjects were rehospitalized for congestion during the study follow-up period, and all subjects improved by at least one NYHA class. The clinical benefits observed in the clinical study resulted in a 75% reduction in the predicted one-year mortality rate based on the Seattle Heart Failure Model.
Meanwhile, Sequana Medical has also developed the second-generation DSR® product (DSR®2.0), a proprietary sodium-free glucose/icodextrin peritoneal dialysis solution with superior therapeutic efficacy and an improved safety profile. Currently, the company is preparing the DSR®2.0 IND Application in the United States. Notably, DSR®The therapy has obtained composition-of-matter and method patents in the United States and Europe.
In December 2023, Sequana Medical submitted a Premarket Approval (PMA) application to the U.S. FDA. This submission was based on the successful implementation of the pivotal POSEIDON study, in which the alfapump was implanted in 69 patients across 18 centers in the United States and Canada.®. In the key cohort, the primary efficacy endpoint at 6 months post-implantation exceeded the prespecified threshold with statistical significance, and the primary safety endpoint data also met expectations. Data at 12 months post-implantation continued to demonstrate significant and durable clinical performance, with virtually no need for therapeutic bypass aspiration, and patients experienced clinically meaningful improvements in quality of life.
To promote the alfapump®Following PMA approval, Sequana Medical has decided to prioritize resources toward achieving this key milestone, which is expected to be completed in the second half of 2024. As a result, the company will significantly reduce its cash burn, cease all commercial activities in Europe, while retaining its CE mark.
This decision was also endorsed by Sequana Medical’s lenders. The lenders agreed to concentrate the company’s cash resources on the alfapump® system.®PMA approval, rather than debt repayment.
On February 8, 2024, Sequana Medical announced continued support from its two major shareholders—securing €3 million in convertible financing from Partners in Equity and Rosetta Capital, and agreeing to defer debt repayment payments.
The Foundation has also committed to providing the company with a total of €16 million in funding prior to FDA approval, and has agreed to defer all payments until after the approval of the alfapump PMA application. This further reduces the company’s cash requirements for 2024. Sequana Medical disclosed that its expected cash requirements for 2024 will be reduced to €13 million.
Next, Sequana Medical will focus on targeting the U.S. market and continue to concentrate on its DSR heart failure program. Following positive outcomes in the first three MOJAVE patients and successful review by the Data Safety Monitoring Board (DSMB), the company will make thorough preparations for the randomized phase of the study.