Innovation and Transformation: The Latest Chapter of Cell Therapy in Autoimmune Diseases
Source: Zhoudu Capital
1.0 Safe and Effective Immune Resetting – The Holy Grail of Autoimmune Diseases
In the vast realm of medicine, autoimmune diseases act like hidden warriors, subtly affecting approximately 5–10% of the global population. These conditions arise when the body’s immune forces mistakenly identify self-antigens as foreign enemies, thereby unleashing an endless civil war. Although it remains challenging in certain cases to pinpoint the specific antigenic epitopes triggering the conflict, the polyclonal activation of the immune system, coupled with selection defects and altered response patterns in B or T lymphocytes, gives rise to a cohort of autoreactive cells. Armed with autoantibodies, these cells inflict tissue damage and inflammation on the battlefield.
In fact, autoimmune diseases is an umbrella term for approximately 80 conditions, affecting about one-tenth of the global population.1. Although the corresponding classifications and treatment approaches vary, traditional therapies for severe cases involve extensive exposure to glucocorticoids and continuous use of immunosuppressants. Such regimens are associated with significant side effects, a high risk of infection, substantial negative impact on patients’ quality of life, and an inability to fully control the disease. For certain conditions characterized by clearly defined autoreactive B cells, such as systemic lupus erythematosus (SLE), B cells in patients mistakenly identify parts of the body as foreign substances and attack them. Therefore, scientists have hypothesized: If we could develop a drug capable of destroying autoreactive B cells, could patients be freed from those harmful antibodies that drive lupus?
It is fair to say that the answer is affirmative. As early as 2002, David Isenberg, who later became President of the British Society for Rheumatology, and his team pioneered the clinical application of B-cell depletion therapy. In six female patients aged 20 to 40 years with active systemic lupus erythematosus (SLE) who were refractory to standard immunosuppressive therapy, the Isenberg team administered two infusions of 500 mg rituximab, two infusions of 750 mg cyclophosphamide, and high-dose oral corticosteroids. The results showed that, except for one patient who developed neurological injury and was lost to follow-up after three months, the remaining five patients achieved substantial improvement in disease assessment. Moreover, the overall safety profile of this regimen was favorable, suggesting that B-cell depletion did not lead to serious infections.2
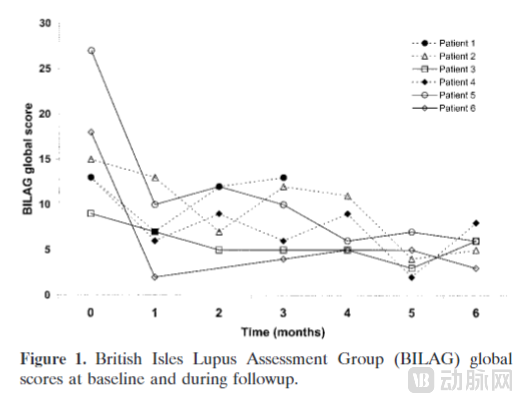 Note: The British Isles Lupus Assessment Group (BILAG) index, used on the vertical axis, is a common tool for assessing SLE disease activity. A total BILAG score exceeding 10 points is generally considered to indicate moderate or higher disease activity.
Note: The British Isles Lupus Assessment Group (BILAG) index, used on the vertical axis, is a common tool for assessing SLE disease activity. A total BILAG score exceeding 10 points is generally considered to indicate moderate or higher disease activity.
While an initial treatment response is certainly encouraging, the ultimate clinical goal for rheumatologists remains achieving 100% remission in patients, thereby preventing further organ damage. Consequently, Isenberg’s team continued to follow up with the five patients who participated in the trial and remained available for ongoing assessment. At a mean follow-up duration of approximately 12.6 months, two patients exhibited low BILAG scores (5 and 3, respectively) and required reduced doses of oral prednisolone, whereas two other patients experienced relapses at 7 and 8 months, respectively. In other words, although anti-B-cell antibody therapy has shown promising early results, not every patient responds to monoclonal antibody treatment; the ideal scenario of a one-click “immune reset,” akin to restoring a computer to its factory settings, has not yet been realized. Indeed, in two subsequent double-blind, placebo-controlled trials in patients with systemic lupus erythematosus (SLE) and lupus nephritis—conducted against a background of standard maintenance therapy—the rituximab-treated groups failed to meet the primary efficacy endpoints at Week 52.3, although both trials demonstrated significant improvements in certain subgroups (such as Black and Hispanic participants in EXPLORER) and for certain serum biomarkers (such as anti-dsDNA levels in LUNAR), with the overall safety profile of the treatment group being comparable to that of the control group.4 5

Note: B-cell depletion therapies are generally considered to be associated with serious infections. Interestingly, in two double-blind controlled trials, the incidence of infections and serious infections was higher in the placebo group than in the treatment group, possibly due to improved physical condition following antibody therapy in patients with the underlying disease. Similar intergroup safety profiles were observed in a double-blind controlled trial of obinutuzumab, a next-generation anti-CD20 monoclonal antibody featuring glycoengineered FcγRIIIa-enhanced effector function for more effective B-cell depletion; specifically, the rates of infection and serious infection were lower in the treatment group than in the placebo group (NCT02550652).6
Based on the negative results from the Isenberg team’s work and the EXPLORER study, Edward M. Vital, who was still a doctoral candidate in 2006, sought to investigate the reasons underlying the low efficacy rate of rituximab. In an article published in 2011, Edward’s team evaluated 39 patients with active systemic lupus erythematosus (SLE) and analyzed their B-cell composition. They identified two potential factors contributing to the failure of these patients to achieve long-term remission: (1) anti-CD20 monoclonal antibodies failed to effectively clear B cells from tissues; and (2) the quantities of memory B cells and plasma cells played a significant role in distinguishing between patients with early relapse and those with sustained response.7. In short, B-cell depletionDepth(from blood to tissues) andBreadth(The insufficiency from mature B cells to plasma cells) may be the reason why early therapies failed to achieve immune reset, which also provides a hint for the development direction of next-generation therapies in the future. In fact, there are cases in Europe and the United States where lymphocyte ablation combined with autologous or allogeneic hematopoietic stem cell transplantation has been used to treat various severe autoimmune diseases, aiming to achieve better efficacy by more intensively clearing B cells. In an observational study involving over 1,300 patients, 43% to 71% of autoimmune disease patients achieved long-term drug-free remission three to five years after transplantation; however, treatment-related mortality as high as 5% to 7% has limited the application prospects of this approach.8 9. In 2019, Edward Vital, who had become an Associate Professor at the University of Leeds School of Medicine, succeeded David Isenberg as the head of the British Isles Lupus Assessment Group (BILAG), and he remains committed to seeking better novel therapies, more optimal immune reset strategies, and patient education for systemic lupus erythematosus.

Note: Third from the left in the front row is Professor David Isenberg; fourth from the left in the front row is Edward Vital (Image source: X/Twitter)
Fast-forwarding to 2020, Dr. Liu Fang from the General Hospital of Chengdu Military Command and Dr. Zhang Hongyu from Peking University Shenzhen Hospital reported a case involving dual-target CD19/BCMA CAR-T therapy. The patient was a 41-year-old newly diagnosed with stage IV diffuse large B-cell lymphoma (DLBCL) and had a 20-year history of systemic lupus erythematosus (SLE). The medical team employed a conditioning regimen of fludarabine and cyclophosphamide, followed by administration of CAR-T cells at a dose of 5.3×10⁶/kg. Complete remission of the lymphoma was achieved by day 28, accompanied by a significant reduction in the patient’s antinuclear antibody levels.10. In subsequent follow-up reports, the patient’s B cells recovered after 260 days, and symptoms of systemic lupus erythematosus (SLE) and lymphoma went into remission at 23 months, with an overall favorable safety profile for the treatment.11. Although this case is not solely focused on autoimmune diseases, compared with the antibody therapies and hematopoietic stem cell transplantation therapies from earlier experiments, we seem to be one step closer to the ideal of immune reset.
Perhaps guided by the industry consensus toward more comprehensive B-cell depletion, or inspired by the experience of Chinese teams, Professor Georg Schett from Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU) in Germany has developed a strong interest in exploring whether CAR-T therapy can help patients with autoimmune diseases reset their immune systems and achieve deep, drug-free remission (“So the idea was that when you could deplete B cells as good as in cancer in lymphoma leukemia in autoimmune disease that you could really reset the entire disease and allow a deep drug-free remission in these patients”).

Professor Georg Schett (Image credit: Simone Kessler/Uniklinikum Erlangen)
Professor Schett and his team subsequently launched a series of trials aimed at comprehensively evaluating the potential and efficacy of CAR-T therapy in treating autoimmune diseases. Meanwhile, astute immunology experts in China also demonstrated strong interest in this emerging therapeutic strategy and rapidly initiated related research endeavors, striving to achieve breakthrough progress in this frontier area of medicine.
1.1 One Treatment, Long-Term Remission
In August 2021, Professor Georg Schett’s team published a case study in The New England Journal of Medicine, reporting on a female patient with severe systemic lupus erythematosus (SLE) involving the joints, kidneys, heart, and lungs. After experiencing relapse and resistance to various standard medications, the patient received CD19 CAR-T cell therapy. By day 44, her SLE Disease Activity Index (SLEDAI) score decreased from 16 to 0, with no significant adverse effects observed. The patient remained in remission four months after discontinuing all medications.12。
Despite involving only a single patient and a mere four months of observation, key findings such as “drug-free remission,” “normalization of serological markers,” and “rapid decline in urinary protein levels” quickly captured the attention of numerous experts in the field of autoimmunity. These results signal that we are moving closer to the goal of immune reset: CD19 CAR-T therapy induces a rapid reduction in antibody levels and sustained symptom relief by targeting plasmablasts. Given the pivotal role of B cells in various severe autoimmune diseases, interrupting the disease process at the B-cell level causes a cascading collapse, akin to a house of cards, thereby enabling long-term drug-free remission for patients—a therapeutic approach poised to fundamentally transform the landscape of autoimmune disease treatment.
The Schett team further fueled this exciting prospect: in September 2022, they reported in Nature Medicine the outcomes of CD19 CAR-T cell therapy in five patients with refractory systemic lupus erythematosus (SLE), including four women and one man. Lupus nephritis was resolved in all patients, with serum complement levels and anti-double-stranded DNA antibodies returning to normal. Furthermore, other SLE-related symptoms, such as arthritis, fatigue, and cardiac valve fibrosis, disappeared. During follow-up, all patients achieved drug-free remission, with the longest observation period reaching 17 months.13。
Nothing can now hinder Schett’s further exploratory strides. Successive achievements in the field of systemic lupus erythematosus (SLE) have bolstered his confidence to pivot toward other complex autoimmune diseases. In March 2023, his team published a case report in The Lancet on a patient with anti-synthetase syndrome (ASS). This male patient had suffered from active myositis for 18 months. His condition was poorly controlled with oral corticosteroids, and rituximab therapy failed to suppress myositis activity, even leading to dyspnea. Following CD19 CAR-T cell therapy, anti-synthetase antibodies were successfully eliminated, and complete symptom remission was achieved. Inflammation in the muscles and joints nearly resolved entirely, radiological signs of alveolitis disappeared completely, and muscle strength and endurance were restored. CD19+ B cells reappeared at day 100, and the patient remained drug-free for 180 days post–CAR-T cell therapy.14。
In December 2023, in response to the Phase 1b/2a clinical study results of Cartesian’s mRNA-engineered autologous CAR-T therapy for the treatment of severe myasthenia gravis15, Schett’s team published a case report in The Lancet Neurology on the successful treatment of myasthenia gravis (MG) with CD19-targeted CAR-T cell therapy. After various immunosuppressive therapies failed to control the patient’s condition, the patient received CD19-targeted CAR-T cell therapy. Two months later, muscle strength and fatigue showed significant improvement; the duration for which the patient could hold their arms outstretched horizontally steadily increased, and walking ability markedly improved without any assistive devices. The physicians plan to discontinue maintenance-dose immunosuppressants.16
 Seven Autoimmune Patients Who Successfully Participated in CAR-T Therapy Trials (Image Source: SIMOarts/Simone Kessler)
Seven Autoimmune Patients Who Successfully Participated in CAR-T Therapy Trials (Image Source: SIMOarts/Simone Kessler)
The enthusiasm for cellular therapy in autoimmune diseases reached a crescendo with Schett’s presentation at the American Society of Hematology (ASH) Annual Meeting in December 2023: among the 15 patients with autoimmune diseases who received CD19 CAR-T therapy, there were 8 with systemic lupus erythematosus (SLE), 4 with systemic sclerosis (SSc), and 3 with idiopathic inflammatory myopathies (IIM). All SLE patients achieved remission according to the DORIS criteria, all IIM patients met the major clinical response criteria established by the American College of Rheumatology/European Alliance of Associations for Rheumatology (ACR/EULAR), and all SSc patients showed a reduction in their European Alliance of Associations for Rheumatology Scleroderma Trials and Research Group (EUSTAR) activity index scores. During a median follow-up period of 15 months, autoantibodies disappeared in all patients, and they successfully discontinued immunosuppressive medications, including glucocorticoids. These results were subsequently published in the New England Journal of Medicine.17
At the 2024 European Alliance of Associations for Rheumatology (EULAR 2024) conference, Schett’s team presented updated follow-up data on the aforementioned 15 patients. Twelve patients had been followed for more than one year, with a median follow-up duration of 18 months. All patients maintained clinical remission and did not resume any immunosuppressive therapy. Regarding safety, one patient developed grade 4 neutropenia 120 days after treatment.18
Professor Georg Schett stated confidently in a press release, “We believe we have successfully identified a reset button that functions like a computer’s, capable of rebooting the immune system without error.”19Unsurprisingly, the use of cell therapy for autoimmune diseases has become a hot topic. Investors, sensing the spring breeze of recovery in the U.S. pharmaceutical investment market, are all asking: Are there any cell therapy projects targeting autoimmune diseases?
1.2 The Booming Development Enthusiasm in the Industry—A Tide Will Lift All Boats
Schett’s research has undoubtedly provided a significant boost to cell therapies whose indications are currently limited to hematologic malignancies. The successful reporting of a series of clinical trials has further galvanized enthusiasm within both the medical and investment communities for investing in cell therapies and other related approaches aimed at immune reset. We have also witnessed a wave of exciting mergers and acquisitions, large-scale IPOs, and a flurry of strategic pivots—converging independently yet consistently—toward the battlefield of autoimmune diseases. A surge of interest in “immune reconstitution” is now sweeping through both the industry and the investment sector:

Source: Public Information
The above list is not exhaustive; numerous cell therapy companies (whether autologous or allogeneic) and next-generation antibody-based drug developers are also charging toward the goal of “immune reset,” each driven by its own unique understanding.
2.1 Cell Therapy in Autoimmune is a well de-risk play
In reviewing the first part, we gained insight into the fact that the application of cell therapy in autoimmune diseases has not been an overnight success. In the past two years, “de-risking” has become a buzzword in the medical investment community. While seeking the next breakthrough therapy, investors are also eager to minimize the uncertainties inherent in drug development, making cell therapy for autoimmune diseases an approach with substantially mitigated risk.
Standing on the Shoulders of Oncology Treatment: As CD19 and BCMA targets have already been approved in the field of oncology, the industrial chain, manufacturing processes, and clinical applications are gradually maturing. Therefore, the application of cell therapy in autoimmune diseases is more akin to a well-established tool finally finding its optimal use case. The industry and clinicians can fully leverage the experience gained in oncology to further enhance capabilities in product design, manufacturing processes, and cost control. Taking off-the-shelf cell therapies, such as gene-edited CAR-T and CAR-NK therapies, as examples, the clinical data disclosed in recent years within the oncology field has arguably fallen short of previous industry expectations. This may be attributed to the short persistence of these cells in tumor environments, where they struggle against malignant B cells present at high orders of magnitude. However, in the field of autoimmune diseases, these disadvantages may potentially transform into certain advantages. Existing clinical data indicate that B-cell repopulation in patients with autoimmune diseases can occur as early as six weeks, suggesting that the depth of B-cell depletion appears to be more critical than its durability. Poseida Therapeutics, a universal cell therapy company, stated in its latest performance presentation what perhaps represents the industry’s general attitude toward developing treatments for autoimmune diseases: “not so much whether we will do it, but how.” Given that off-the-shelf CAR-T and CAR-NK therapies can be manufactured as standardized products and may induce milder drug-related adverse reactions, they hold promise for future expansion into outpatient settings. If the efficacy and safety of these therapies are validated, they are expected to offer broad application prospects.
Multinational pharmaceutical giants have shown strong interest.“The potential for a functional cure has never been realized before; (cell therapy for autoimmune diseases) could be a game-changer.” In an opinion piece published in Nature Reviews Drug Discovery in April 2024, Robert Plenge, Head of Research at Bristol Myers Squibb (BMS), shared BMS’s unique insights on the application of cell therapy in autoimmune diseases.28Dr. Plenge, formerly a rheumatologist, observed that his patients were often disheartened by the burden of long-term medication. With emerging clinical data on the application of CAR-T therapy in autoimmune diseases, Dr. Plenge believes that treatment in this field may have reached a historic turning point. In China, Jw Therapeutics’ CD19 CAR-T product, relma-cel, also presented preliminary clinical data for systemic lupus erythematosus (SLE) at EULAR 2024. Three subjects receiving low-dose treatment showed continued improvement in clinical indicators at the six-month follow-up and had discontinued conventional glucocorticoids and immunosuppressants. Across all dose groups, one case of grade 3 cytokine release syndrome (CRS) and two cases of grade 3 infections were reported, with no cases of neurotoxicity.29
Guided by this innovative R&D logic, Bristol Myers Squibb (BMS) is advancing the development of its CD19 NEXT product. At the 2024 J.P. Morgan Healthcare Conference, BMS unveiled this product as an advanced version of Breyanzi, achieved through process innovations. BMS believes that CD19 NEXT has the potential to treat a range of B cell-mediated autoimmune diseases, including systemic lupus erythematosus, myositis, and multiple sclerosis. Compared with the field of hematologic malignancies, the patient population for these autoimmune diseases is projected to be five to ten times larger.
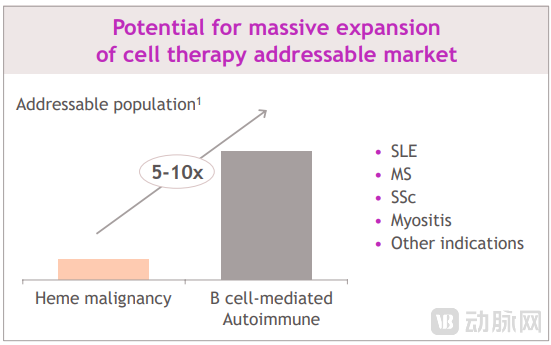 Source: 2024 JPM BMS Investor Deck
Source: 2024 JPM BMS Investor Deck
In the competitive landscape of cell therapy, BMS’s rival Novartis is demonstrating relentless R&D momentum. Novartis is developing an innovative CD19 CAR-T product, YTB323 (rapcabtagene autoleucel), which employs the same CAR structure as the approved Kymriah and leverages Novartis’s T-Charge platform for manufacturing. This approach is expected to shorten the production cycle and enhance T-cell stemness (“T-Charge preserves T cell stemness, the ability to self-renew and mature”).30). At the 2023 American College of Rheumatology (ACR) Annual Meeting, Novartis presented primary efficacy and safety data for YTB323 in the treatment of three patients with severe systemic lupus erythematosus (SLE) (NCT05798117). All patients received preconditioning with cyclophosphamide and fludarabine, with follow-up periods ranging from 28 to 106 days. The results showed a reduction in SLEDAI-2K scores for all three patients, while the Physician’s Global Assessment (PGA) scores decreased from approximately 75 to between 15 and 40. Anti-double-stranded DNA (anti-dsDNA) antibody levels were significantly reduced in the first two patients. Regarding safety, no serious adverse events or deaths were reported in the study. Patients 1 and 2 experienced cytokine release syndrome (CRS; Grade 1 or 2), and Patients 1 and 2 developed hypogammaglobulinemia (Grade 2 or 3). These preliminary data provide positive signals regarding the potential of YTB323 in the treatment of SLE, demonstrating Novartis’ strong commitment and scientific capability in advancing CAR-T therapy for autoimmune diseases.
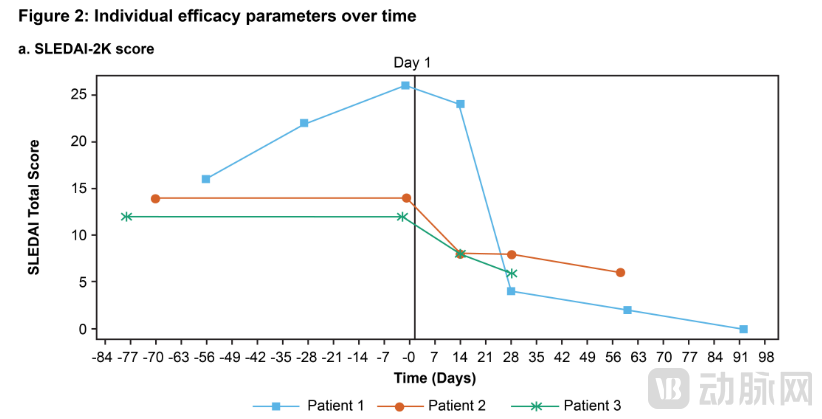
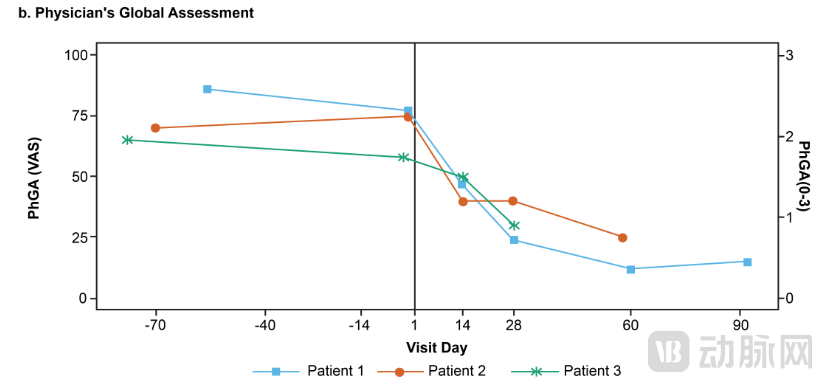 Source: An Open-label, Multicenter, Phase 1/2 Study to Assess Safety, Efficacy and Cellular Kinetics of YTB323, a Rapid Manufacturing CAR-T Cell Therapy Targeting CD19 on B Cells, for Severe Refractory Systemic Lupus Erythematosus: Preliminary Results
Source: An Open-label, Multicenter, Phase 1/2 Study to Assess Safety, Efficacy and Cellular Kinetics of YTB323, a Rapid Manufacturing CAR-T Cell Therapy Targeting CD19 on B Cells, for Severe Refractory Systemic Lupus Erythematosus: Preliminary Results
Dr. Andrew Baum, a highly respected figure on Wall Street, has long been a staunch advocate for the use of cell therapies in treating autoimmune diseases. During a quarterly conference call in his career as an analyst, he publicly encouraged Novartis to accelerate the research and development of its cell therapy products in the field of autoimmune diseases. In his report, Dr. Baum expressed the view: “We believe that for refractory autoimmune diseases, CAR-T cell therapy represents the most disruptive and commercially promising opportunity since the resurgence of immuno-oncology in 2011.”31“Recently, Dr. Baum joined Pfizer as Chief Strategy and Innovation Officer, a new role that undoubtedly fuels our anticipation for Pfizer’s proactive expansion in the field of cell therapy for autoimmune diseases.”
3.1 Overview of Leading Players in the Field

● Introduction: Kyverna Therapeutics, founded in 2018, completed a total of $180 million in financing prior to its initial public offering and listed on the Nasdaq (Ticker: KYTX) in February 2024, raising $319 million.
● Technical Highlights: KYV-101 utilizes a CAR structure optimized by the U.S. National Institutes of Health (NIH) based on Gilead/Kite’s Yescarta framework. Its differentiating features include the use of fully human CD19 CAR domains and optimized hinge and transmembrane domains (CD8α hinge and TM domains versus CD28 hinge and TM domains), with the aim of enhancing drug safety. Meanwhile, Kyverna is collaborating with the gene-editing company Intellia Therapeutics to develop next-generation universal gene-edited CAR-T therapies. Currently, KYV-101 is in Phase I clinical trials, with four studies underway targeting systemic lupus erythematosus, lupus nephritis, myasthenia gravis, and multiple sclerosis.
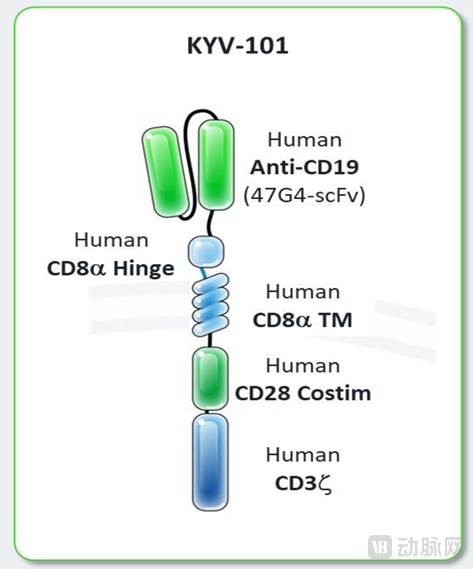
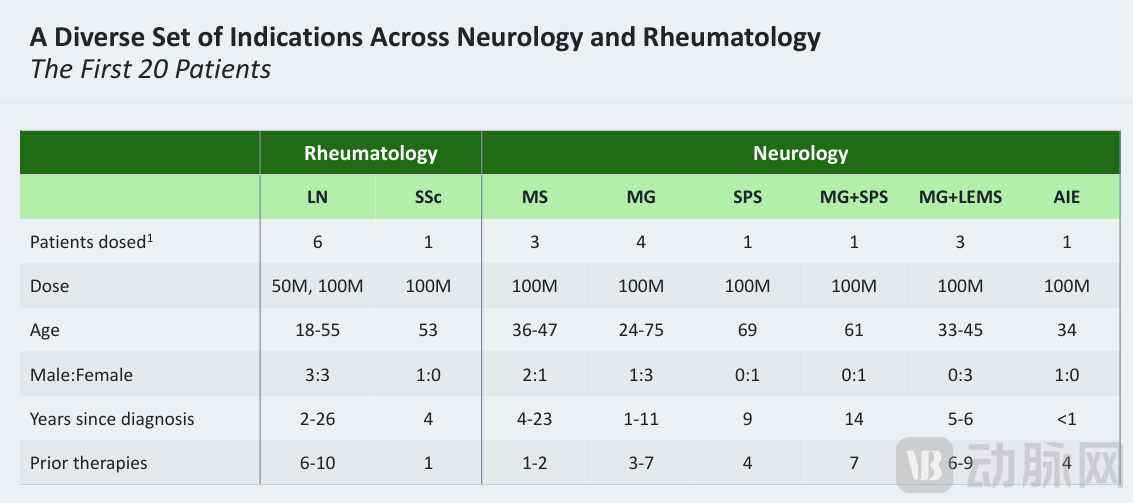
Source: May 2024 Investor Deck, Display of KYV-101’s Drug Structure and Clinical Data from the First 20 Patients

● Introduction: Cabaletta Bio is a biotechnology company founded in 2017, initially built upon the chimeric autoantibody receptor T cell (CAAR-T) technology developed by Dr. Aimee Payne and Dr. Michael Milone at the University of Pennsylvania. The company is dedicated to selectively targeting and eliminating B cells that express specific self-antigens, thereby reducing the risk of non-specific B-cell depletion. However, due to suboptimal efficacy of its lead candidate, DSG3-CAART, in treating mucous membrane pemphigoid (mPV), and the growing body of global evidence supporting the use of CAR-T therapies for autoimmune diseases, Cabaletta Bio entered into a collaboration agreement with Legend Biotech in October 2022. Under this agreement, “Legend Biotech granted Cabaletta exclusive global rights to develop, manufacture, and commercialize its fully human CD19 sequence for use in Cabaletta’s modified T-cell products targeting autoimmune diseases.” In return, Legend Biotech received an upfront payment of $162 million, along with potential development and commercialization milestone payments and sales royalties. Consequently, Cabaletta Bio has redirected all its resources toward its CD19-CAR-T pipeline candidate, CABA-201. In terms of capital markets, Cabaletta Bio completed a total of $88 million in financing prior to its initial public offering and listed on the Nasdaq in October 2029 (Ticker: CABA), raising $74.8 million.
● Pipeline Status: Cabaletta is advancing the Phase 1/2 clinical trial of CABA-201 for the treatment of systemic lupus erythematosus, pemphigus (exploring a regimen without lymphodepletion), autoimmune myositis, systemic sclerosis, and generalized myasthenia gravis.
● The IR Deck outlines the product’s origins and highlights key points for investors to consider, making it a valuable reference.
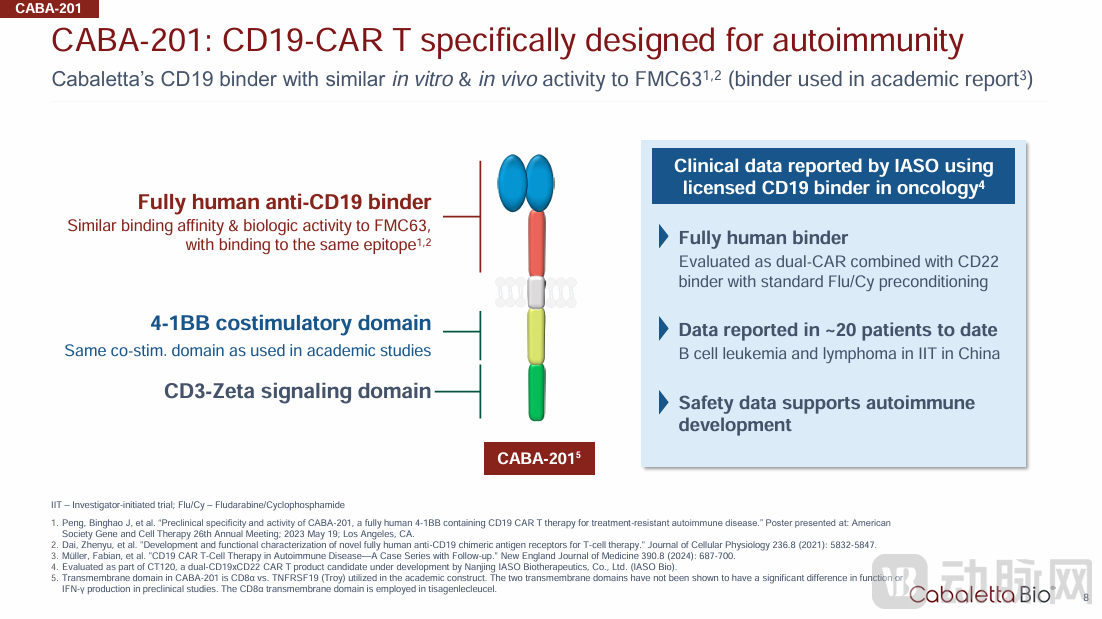
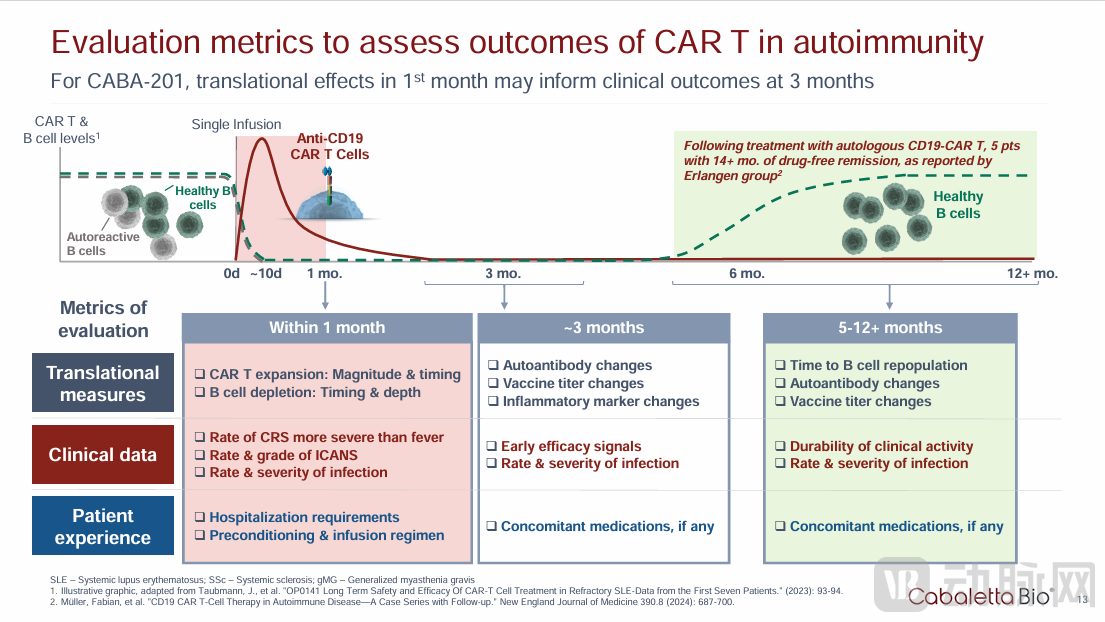 Source: May 2024 Investor Deck
Source: May 2024 Investor Deck

● Introduction: During the Q4 2023 earnings call, Nkarta’s management announced that the company would lower the development priority of its NKX019 (CD19 CAR-NK) program for the acute myeloid leukemia (AML) indication, shifting focus instead to autoimmune diseases. Inspired by the work of Schett’s team, the company believes that achieving immune reset in autoimmune diseases is more critical than durability, noting that “depth but not the duration of B-cell killing is key to driving clinical benefit in auto-immune disease.”
● Technical FeaturesNkarta has conducted multifaceted explorations for NKX019, including a lymphodepletion strategy designed to differentiate the pharmacokinetics of NK cells, sustained stimulation via membrane-bound IL-15, and novel co-stimulatory domain designs. The Investigational New Drug (IND) application for NKX019 was approved in the fourth quarter of 2023. This dose-escalation trial will evaluate NKX019 in patients with refractory lupus nephritis (LN), who will receive three doses of NKX019 following lymphodepletion (LD) with cyclophosphamide (Cy)-only regimens. Nkarta expects to provide updates on clinical progress in the first half of 2024.
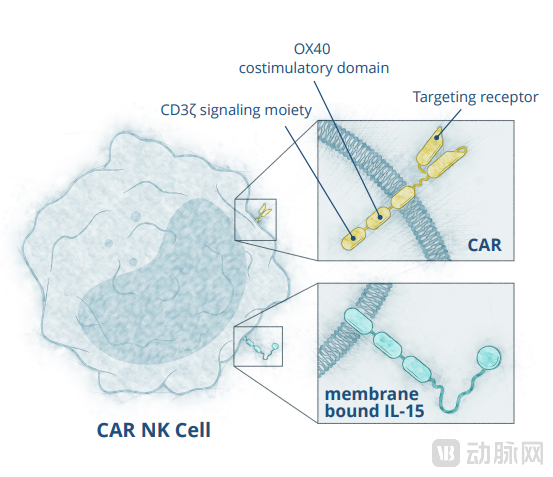 Source: March 2024 Investor Deck; Nkarta’s CAR-NK product utilizes a distinct co-stimulatory domain design and expresses IL-15 on the cell surface to promote in vivo persistence.
Source: March 2024 Investor Deck; Nkarta’s CAR-NK product utilizes a distinct co-stimulatory domain design and expresses IL-15 on the cell surface to promote in vivo persistence.

● IntroductionCartesian Therapeutics (Ticker: RNAC) is the world’s first company to apply mRNA technology to cell therapies for the treatment of autoimmune diseases, and it is currently advancing its core product, Descartes-08, through Phase 2b clinical development. Cartesian went public in November 2023 via a reverse merger with Selecta Biosciences. Perhaps due to this less conventional path to listing, the company has attracted relatively low market attention thus far, with a market capitalization of approximately $500 million as of May 2024. Notably, Dr. Timothy Springer, a renowned professor at Harvard Medical School and co-founder of both Selecta Biosciences and Moderna, personally invested $60 million in Cartesian. Professor Springer has successfully participated in the founding and incubation of multiple enterprises. According to his profile on the Harvard University website, his personal internal rate of return (IRR) reached an impressive 78% from 2008 to 2016, excluding founder’s equity.33
● Technical Features: The company’s core pipeline asset, Descartes-08, is an autologous, mRNA-encoded, BCMA-targeted CAR-T cell therapy (also known as rCAR-T). Possibly due to the inherently short persistence of mRNA-engineered CAR-T cells, Descartes-08 demonstrates a favorable safety profile in clinical settings, with apparently lower risks of cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS), and currently enables outpatient administration within 15 minutes. However, also attributable to its shorter persistence, Descartes-08 requires once-weekly dosing for six consecutive weeks. In current small-sample studies, over 70% of patients have maintained durability up to one year. In short, the distinctiveness of Descartes-08 lies in creating a cell therapy that behaves more like a biologic agent, striving to balance efficacy with convenience of administration. Descartes-08 is currently in Phase 2 clinical development. In Phase 1, seven patients with severe myasthenia gravis showed sustained disease improvement nine months after initial treatment, with no signs of CRS or ICANS. Five patients maintained clinical improvement at Month 12; among those who experienced disease relapse at 12 months, one patient achieved rapid improvement in clinical scores upon retreatment. The company expects to provide updated data from the randomized, double-blind, placebo-controlled Phase 2b trial (N=30) by mid-2024.
● Presentation of Clinical Data in Investor Communications:
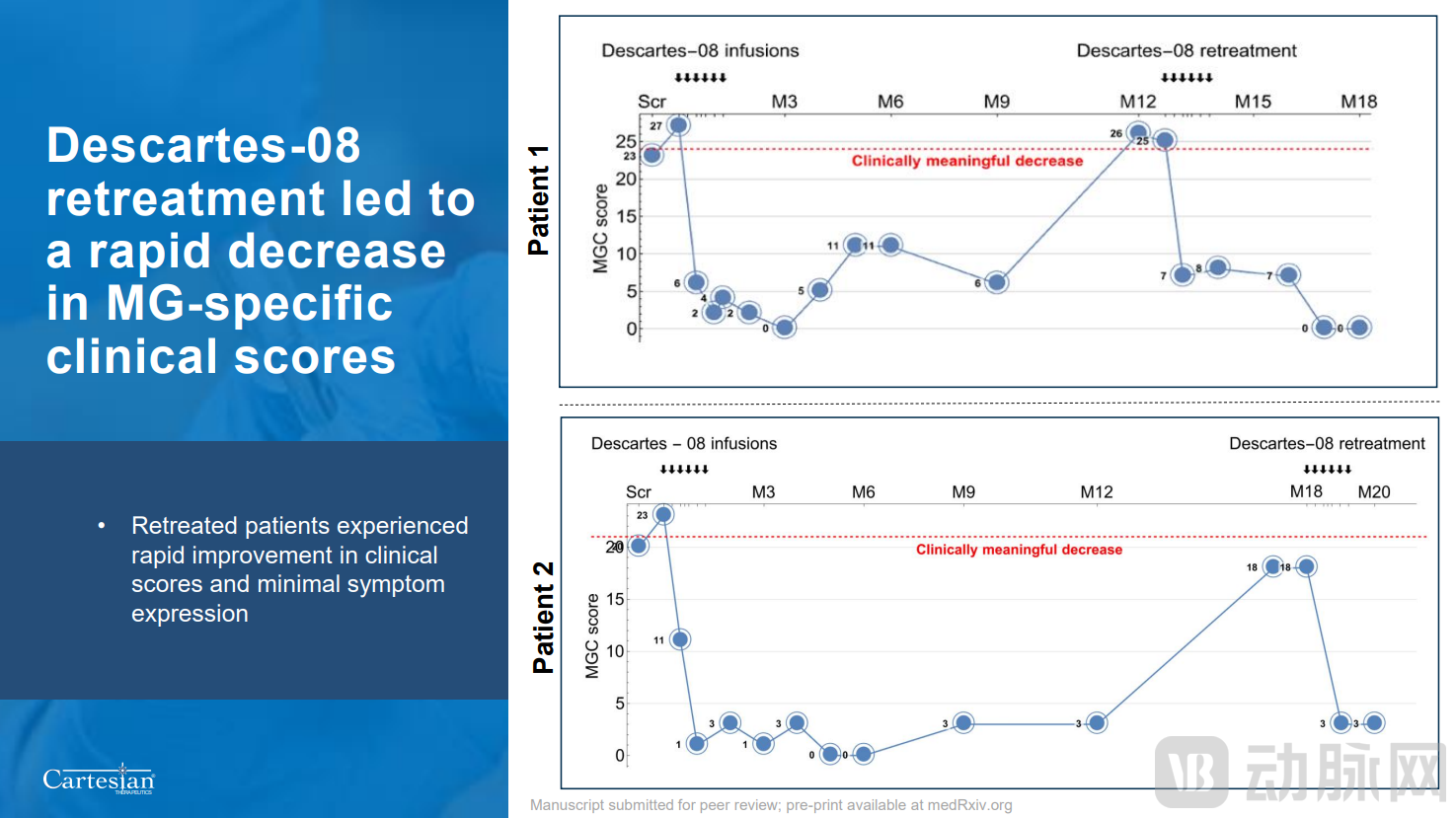
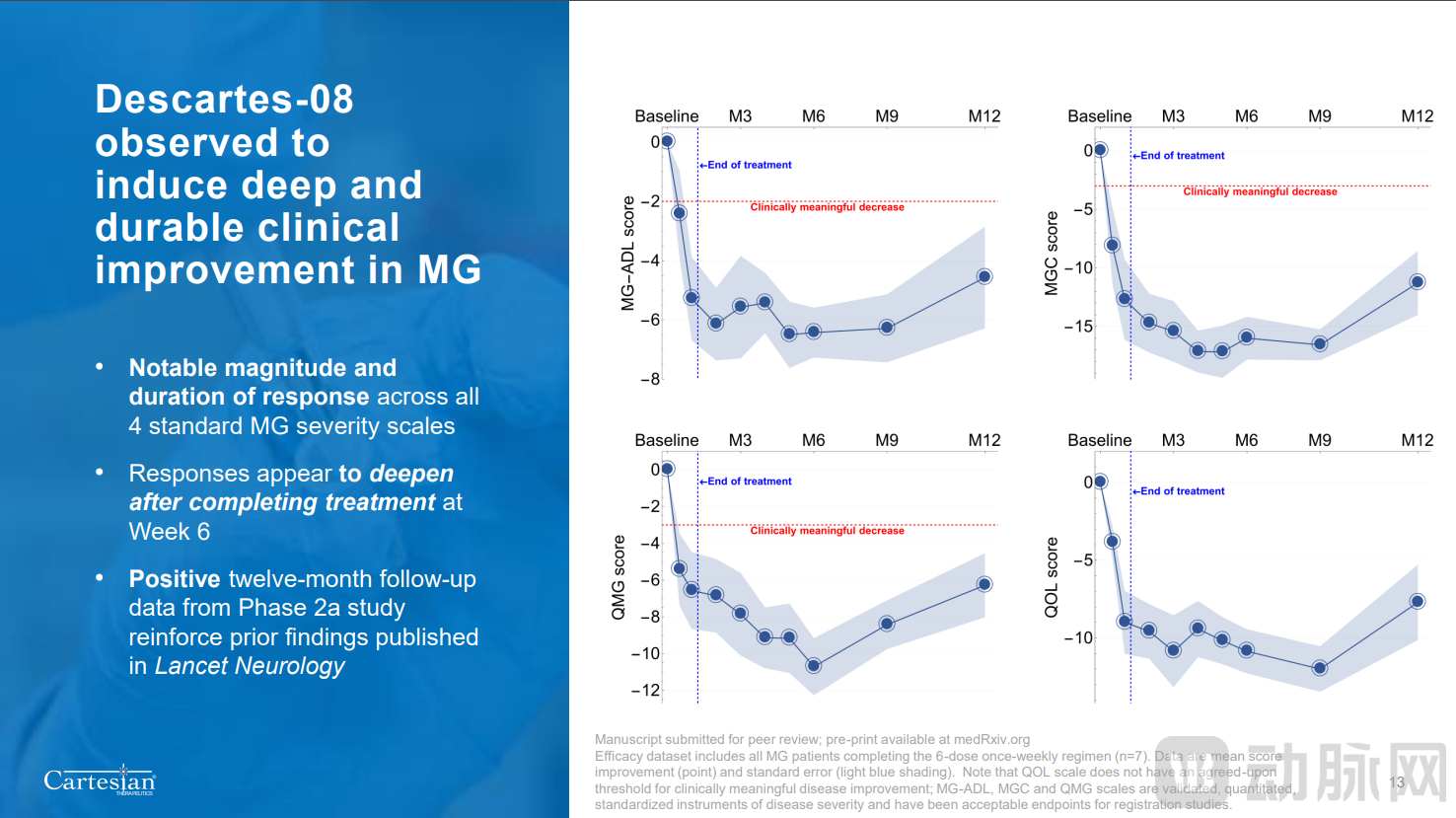
Source: May 2024 Investor Deck. The first article, covering 7 patients, was published in The Lancet Neurology in July 2023 (https://doi.org/10.1016/S1474-4422(23)00194-1). A preprint of the 12-month follow-up article from the same trial was released in January 2024 (https://doi.org/10.1101/2024.01.03.24300770).

● Company Profile: ImmPACT Bio is a clinical-stage cell therapy company based in California, USA. The company was founded on the work of Associate Professor Yvonne Chen and Dr. Sarah Larson at the University of California, Los Angeles (UCLA). It is dedicated to developing differentiated CAR-T therapies that can effectively distinguish between cancerous and healthy cells, thereby enabling more precise targeted treatment. Public information indicates that ImmPACT Bio completed a $140 million Series B financing round in early 2024, led by Foresite Capital, Decheng Capital, and venBio.
● Technical Features: In August 2023, IMPT-514 received FDA approval for an Investigational New Drug (IND) application to conduct an open-label Phase 1b/2 dose-escalation trial for the treatment of active, refractory systemic lupus erythematosus (SLE). ImmPACT Bio anticipates that the first patient will be dosed in early 2024.34IMPT-514 is the company’s bispecific CD19/CD20 CAR-T therapy. Its CAR structure is identical to that of the company’s oncology product IMPT-314, which was initially developed to address antigen loss and immune escape in tumors through dual-target coverage. According to data published by the company, IMPT-514, with the same structural design, demonstrated excellent safety profiles in B-cell lymphoma studies (no ICANS cases and one case of CRS).35。
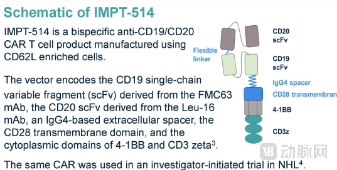
Source: ImmPACT Bio Official Website

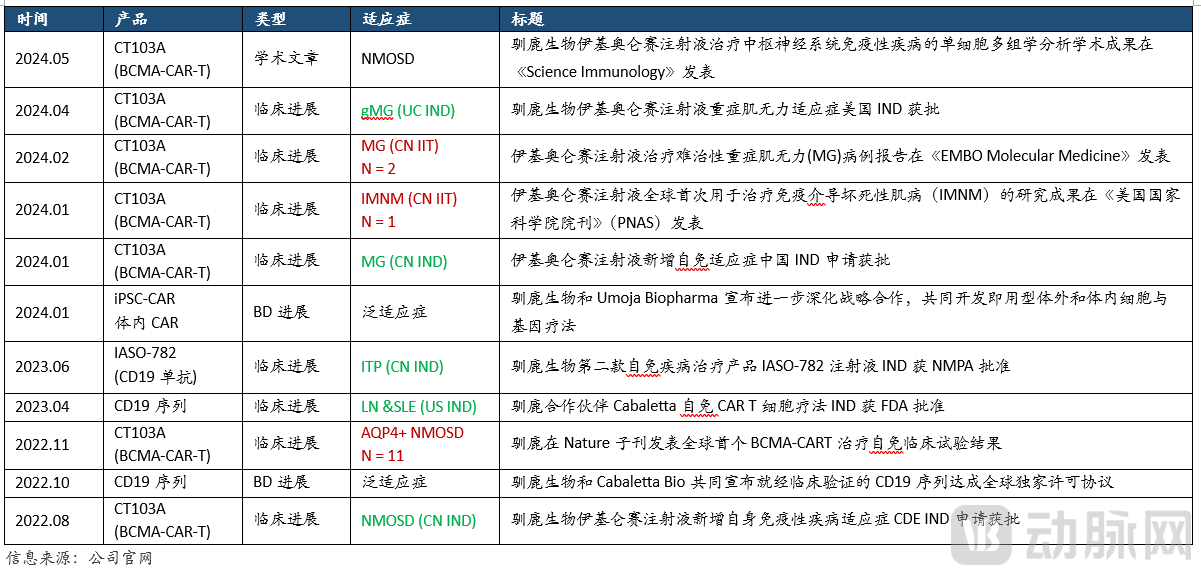
● Company Profile: Founded in 2017, RenovoLife is a biopharmaceutical company dedicated to the research and development, manufacturing, and commercialization of innovative cell therapies. With the development of cellular therapies for hematologic malignancies as its innovation cornerstone, the company is expanding into autoimmune diseases and antibody-based therapeutics. Its lead pipeline product is eltaglunoleucel injection (Fukesu®) was approved for marketing in June 2023 for the treatment of relapsed/refractory multiple myeloma (RRMM) in patients who have received four or more prior lines of therapy. Its earlier-line indication for the treatment of multiple myeloma (MM) in patients who have received two to three prior lines of therapy has entered Phase III clinical trials. Benefiting from its fully humanized targeted CAR structure, Fucosu®Demonstrating excellent efficacy and safety, it is currently in a phase of rapid commercial sales. In the field of autoimmune diseases, IASO Biotherapeutics is one of the first companies in China to apply cell therapy to autoimmune conditions. In investigator-initiated trials (IITs), Equecabtagene Autoleucel Injection has demonstrated breakthrough clinical efficacy in treating various autoimmune diseases and has received clinical trial approvals in both China and the United States for indications including neuromyelitis optica spectrum disorder (NMOSD) and myasthenia gravis (MG).
● Pipeline Overview: According to public information, IASO Bio has established a comprehensive presence in this field. In terms of target pipeline, the company’s fully human BCMA-CAR-T, fully human CD19 monoclonal antibody, and CD19/CD22 dual-target CAR-T have all accumulated substantial clinical data. From a technological perspective, the company’s BCMA CAR-T product received approval from the National Medical Products Administration (NMPA) for market launch in June 2023 and is currently undergoing commercial sales, indicating that IASO Bio ranks among the leaders in the entire cell therapy sector regarding manufacturing process maturity and production stability. Meanwhile, IASO Bio demonstrates strong business development (BD) partnership capabilities; its fully human CD19 sequence has been successfully licensed to Cabaletta Bio, an industry leader, serving as a core pillar supporting Cabaletta’s market valuation (in fact, Cabaletta’s stock price has increased more than tenfold since securing the license from IASO). In addition to Cabaletta, the company has entered into global BD licensing or R&D collaborations with overseas cell therapy firms Sana Therapeutics and Umoja Biopharma, actively exploring the development of next-generation cell therapy products.
 Source: Company Website
Source: Company Website
Currently, based on multiple clinical reports published by Xunlu Biopharma, the company and its partners have established a presence in several autoimmune diseases with significant unmet clinical needs, including systemic lupus erythematosus, lupus nephritis, immune thrombocytopenia, myasthenia gravis, immune-mediated necrotizing myopathy, neuromyelitis optica spectrum disorders, and warm antibody autoimmune hemolytic anemia (wAIHA).

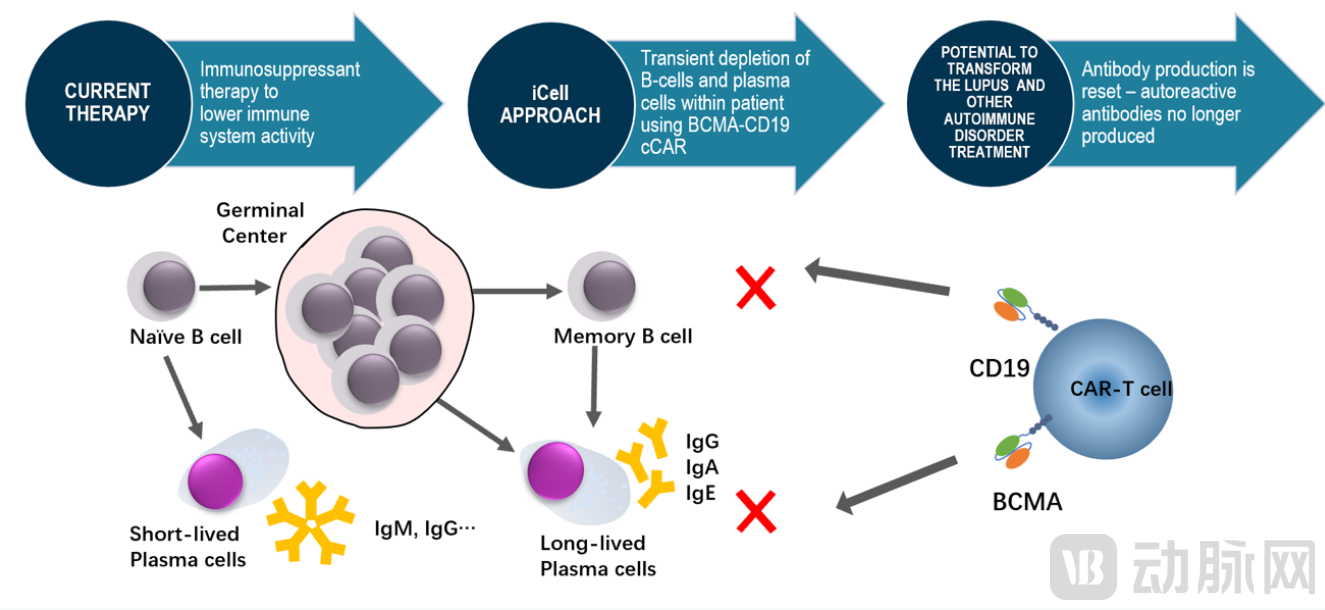
● Company ProfileiCell Gene Therapeutics was founded in 2014, built upon technology developed by Dr. Yupo Ma, Professor of Pathology at Stony Brook University, State University of New York. According to the company’s official website, iCell’s therapeutic development focuses include T-cell lymphoma, acute myeloid leukemia (AML), systemic lupus erythematosus (SLE), multiple sclerosis, and solid tumors. The product developed by the iCell team is termed compound CAR-T (cCAR-T), which incorporates two independently targeting CARs within a single construct. The company’s first product for autoimmune diseases targets both BCMA and CD19, aiming to achieve rapid and complete immune reset through dual-target coverage, resulting in “transient depletion of B-cells and plasma cells.”
● Pipeline OverviewIn the May 2024 issue of *Annals of the Rheumatic Diseases*, iCell reported positive results from its investigator-initiated trial (IIT) of BCMA-CD19 cCAR-T therapy for systemic lupus erythematosus (SLE) and lupus nephritis (LN). The trial was conducted at Zhongshan People’s Hospital and Peking University Shenzhen Hospital in China, with a follow-up period of up to 46 months. Specifically, all patients discontinued all medications prior to treatment. Ten LN patients received a single dose of cCAR-T cells at 3×10⁶/kg. Depletion of peripheral B cells and immunoglobulins was observed at 10 and 42 days post-treatment. B cells and IgM levels recovered within 2–6 months after treatment. Regarding clinical efficacy, all SLE patients who received the target dose (12/13) tested negative for autoantibodies (including those derived from long-lived plasma cells) and showed normalized complement levels three months after cCAR-T therapy. After 46 months of follow-up, patients achieved drug-free, asymptomatic remission. The mean SLEDAI-2K score decreased from 9.9 at baseline to 2.3 at three months. In terms of safety, a key concern for the industry, cCAR-T therapy demonstrated good tolerability. Only mild cytokine release syndrome (CRS) occurred (no cases of CRS > Grade 1), there were no instances of immune effector cell-associated neurotoxicity syndrome (ICANS), and one case of Grade 1 urinary tract infection was reported. Next, iCell plans to conduct clinical trials in both China and the United States.
 Source: Company Website
Source: Company Website
3.2 Future Catalysts for the Field
2024 is destined to be a year of rapid advancement in cellular immunotherapy. Let’s examine the “key catalysts” among publicly listed companies that are poised to further ignite market attention, ensuring we all stay at the “forefront of the era.”
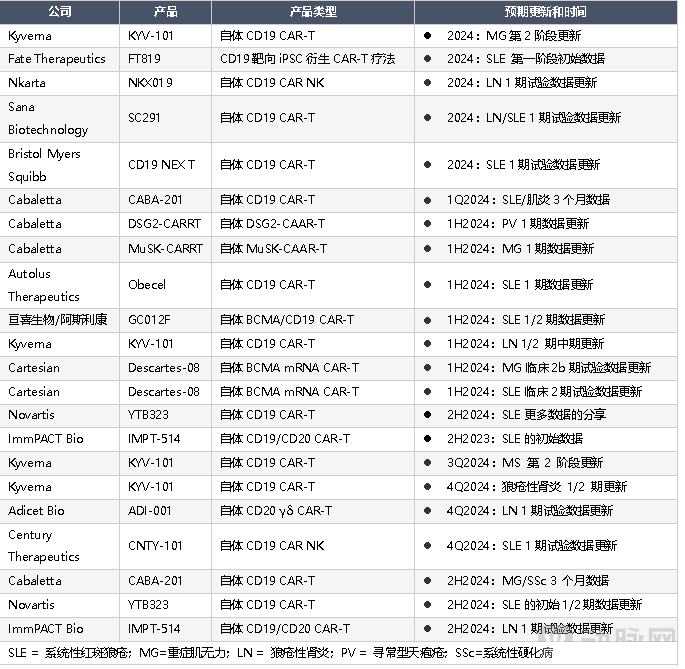
Source: Public Information
4.1 Takeaways—Key Issues Worth Attention in This Field
During the preparation of this report, our team inevitably encountered a series of questions. To delve deeper into these issues, we plan to proceed fromTechnology and ClinicalFrom this perspective, we have engaged in a series of self-posed questions and answers. We hope that this exploratory process will not only clarify our own uncertainties but also provide precise and detailed answers to certain questions investors may have in this field.
Q: In the context of cell therapy, which target or combination—CD19, BCMA, other B-cell targets, or even dual B-cell targets—will ultimately prevail?
A: There is currently no perfect answer, but we know that compared with CD19, BCMA can more deeply eliminate long-lived cells in the bone marrow, such as plasmablasts and plasma cells. If patients fail to achieve sustained drug-free remission with CD19 cell therapy, it may indicate that further depletion of plasma cells is more appropriate. Currently, one patient with autoimmune myositis in Schett’s team’s CD19 CAR-T treatment group experienced relapse after 1.5 years and did not respond to retreatment with CD19 CAR-T. This patient is expected to be eligible for further treatment with BCMA CAR-T. Regarding target selection for different disease populations, additional data are needed to help establish a screening framework and deepen our understanding of disease biology.
Q: Could the field of autoimmune diseases become a track where NK cells or allogeneic T cells achieve overtaking on a bend?
A: Based on current clinical data, we can observe that the pharmacokinetics (PK) of CAR-T therapy in patients with autoimmune diseases is significantly shorter than in cancer patients. Some patients begin to show B-cell reconstitution as early as six weeks after B-cell depletion; however, current follow-up data have not shown disease recurrence akin to that seen in oncology. Since the key to long-term remission in autoimmune diseases lies in the depth and breadth of B-cell depletion, the durability of depletion may be less critical in this context. Therefore, we may anticipate that CAR-NK and allogeneic CAR-T therapies, which have demonstrated suboptimal persistence of depletion in the oncology setting, could perform well in the treatment of autoimmune diseases. Numerous preclinical data are already available for review, and we look forward to further clinical data disclosures from relevant companies. Although multiple clinical studies—such as those led by Professor Schett’s team overseas, and by Carisoma Life Sciences and iCell Therapeutics in China—have set high standards for the field, we do not believe that cell therapy will achieve long-term remission in 100% of patients. In fact, a novel therapeutic agent that enables more than 50% of patients with autoimmune diseases to achieve a relapse-free survival of at least three years would be highly attractive to the patient population.
Q: Amid the surge in cell therapy for autoimmune diseases, what is the outlook for antibody-based treatments?
A: The early failure cases mentioned above primarily involved rituximab. As a chimeric antibody, rituximab has moderate affinity and is generally unable to effectively clear B cells within the lymphatic system. Although there is currently insufficient evidence to determine the depth of B-cell depletion required to achieve immune reset, existing data suggest that antibody drugs cannot reach the level of B-cell exhaustion achieved by CAR-T therapy. However, from the perspectives of patient population, convenience of administration, and health economics, an antibody product capable of depleting B cells to some extent may be a suitable option for patients with autoimmune diseases involving multiple systems who do not have relapsed or refractory conditions. Additionally, bispecific antibodies, such as those utilizing CD3 as a T-cell engager, may also play a role in the treatment of autoimmune diseases. Recently, Schett’s team published a case series in Nature Medicine detailing the successful treatment of six patients with rheumatoid arthritis using blinatumomab, a CD19/CD3 T-cell engager. Since the patients did not exhibit safety concerns commonly observed in oncology, such as cytokine release syndrome (CRS), immune effector cell-associated neurotoxicity syndrome (ICANS), or neutropenia, and demonstrated promising preliminary clinical efficacy, the ripple effect of this study led to a significant surge in the stock price of Cullinan Therapeutics, which had recently undergone a name change. Nevertheless, the study indicated insufficient durability of response following bispecific antibody treatment; several patients experienced a recurrence of inflammatory responses and required other biologics to control their disease. Therefore, we do not believe that bispecific antibody therapy can replace the robust immune reset capability demonstrated by cellular therapies.
Q: Will the latest black box warning for CAR-T therapy in oncology affect its application in autoimmune diseases?
A: Given that the incidence of T-cell lymphoma in cancer patients is significantly higher than in the general population, and that mutations associated with T-cell malignancies were present prior to T-cell infusion in cases monitored by the FDA, the risk of secondary tumors induced by subsequent CAR-T therapy remains to be observed. Considering the younger average age, reduced chemotherapy exposure, and lower mutation risk in patients with autoimmune diseases, safety concerns regarding CAR-T therapy in the autoimmune field may be less pronounced than in oncology. Furthermore, existing studies suggest that lymphodepletion regimens may increase the likelihood of secondary lymphomas to some extent. Consequently, many industry players, including Cartesian Therapeutics and Cabaletta Bio, are exploring strategies to reduce or even eliminate the use of lymphodepletion or preconditioning in autoimmune patients. However, whether such approaches will compromise the efficacy of “immune reset” requires validation through longer-term data.
5.1 Conclusion
 Image source: BMC Blog Chimeras: from Greek myth to scientific reality?
Image source: BMC Blog Chimeras: from Greek myth to scientific reality?
In the narrative tradition of ancient Greek mythology, the Chimera, a mythical creature blending features of multiple animals, symbolizes chaos and destruction in nature. However, in the field of modern medicine, we are witnessing an innovative transformation: harnessing the chimeric nature of this myth as a therapeutic strategy. By engineering specific antibodies onto the surface of T cells, scientists have skillfully directed this potential biological force, taming it into a precise CAR-T therapy. We anticipate that this “Chimera” of modern medicine, with its unique design and functionality, will leave a significant mark on medical history. Looking ahead to the next decade, we aspire to replicate the miracle of the “Emily Effect” from oncology within the realm of autoimmune diseases. We hope to witness patients with autoimmune diseases who undergo these novel therapies one day proudly holding signs reading “10 years clinical remission,” becoming symbols of steadfast courage and hope that inspire both cancer and autoimmune disease patients to conquer their illnesses.
*Article reference:
1. Incidence, prevalence, and co-occurrence of autoimmune disorders over time and by age, sex, and socioeconomic status: a population-based cohort study of 22 million individuals in the UK
2. Leandro, Maria J et al. “An open study of B lymphocyte depletion in systemic lupus erythematosus.” Arthritis and rheumatism vol. 46,10 (2002): 2673-7. doi:10.1002/art.10541
3. Abid, Naushad et al. “The Safety and Efficacy of Rituximab and Belimumab in Systemic Lupus Erythematosus: A Systematic Review.” Cureus vol. 15,6 e40719. 21 Jun. 2023, doi:10.7759/cureus.40719
4. Merrill, Joan T et al. “Efficacy and safety of rituximab in moderately-to-severely active systemic lupus erythematosus: the randomized, double-blind, phase II/III systemic lupus erythematosus evaluation of rituximab trial.” Arthritis and rheumatism vol. 62,1 (2010): 222-33. doi:10.1002/art.27233
5. Rovin, Brad H et al. “Efficacy and safety of rituximab in patients with active proliferative lupus nephritis: the Lupus Nephritis Assessment with Rituximab study.” Arthritis and rheumatism vol. 64,4 (2012): 1215-26. doi:10.1002/art.34359
6. Furie, Richard A et al. “B-cell depletion with obinutuzumab for the treatment of proliferative lupus nephritis: a randomised, double-blind, placebo-controlled trial.” Annals of the rheumatic diseases vol. 81,1 (2022): 100-107. doi:10.1136/annrheumdis-2021-220920
7. Vital EM, Dass S, Buch MH, Henshaw K, Pease CT, Martin MF, Ponchel F, Rawstron AC, Emery P. B cell biomarkers of rituximab responses in systemic lupus erythematosus. Arthritis Rheum. 2011 Oct;63(10):3038-47. doi: 10.1002/art.30466. PMID: 21618204.
8. Sullivan, Keith M et al. “Hematopoietic cell transplantation for autoimmune disease: updates from Europe and the United States.” Biology of blood and marrow transplantation : journal of the American Society for Blood and Marrow Transplantation vol. 16,1 Suppl (2010): S48-56. doi:10.1016/j.bbmt.2009.10.034
9. Farge, Dominique et al. “Autologous hematopoietic stem cell transplantation for autoimmune diseases: an observational study on 12 years' experience from the European Group for Blood and Marrow Transplantation Working Party on Autoimmune Diseases.” Haematologica vol. 95,2 (2010): 284-92. doi:10.3324/haematol.2009.013458
10.Liu F, Zhang H, Wang X, et alTHU0036 FIRST-IN-HUMAN TRIAL OF BCMA-CD19 COMPOUND CAR IN THE TREATMENT OF AUTOANTIBODY MEDIATED DISORDERSAnnals of the Rheumatic Diseases 2020;79:231.
11.Zhang, Wenli et al. “Treatment of Systemic Lupus Erythematosus using BCMA-CD19 Compound CAR.” Stem cell reviews and reports vol. 17,6 (2021): 2120-2123. doi:10.1007/s12015-021-10251-6
12. Dimitrios Mougiakakos et al. CD19-Targeted CAR T Cells in Refractory Systemic Lupus Erythematosus. NEJM, 2021, doi:10.1056/NEJMc2107725.
13. Anti-CD19 CAR T cell therapy for refractory systemic lupus erythematosus
14. CD19-targeted CAR-T cells in refractory antisynthetase syndrome
15. Safety and clinical activity of autologous RNA chimeric antigen receptor T-cell therapy in myasthenia gravis (MG-001): a prospective, multicentre, open-label, non-randomised phase 1b/2a study. Lancet Neurol 2023
16.Anti-CD19 CAR T cells for refractory myasthenia gravis
17. CD19 CAR T-Cell Therapy in Autoimmune Disease —A Case Series with Follow-up
18.Long-Term Safety And Efficacy Of Car-T Cell Treatment In Severe And Treatment Refractory Autoimmune Disease
19. Revolutionary cell therapy: Restarting immune system switches off autoimmune diseases. FAU Erlangen-Nürnberg.
20.Cullinan Therapeutics Announces Strategic Expansion Into Autoimmune Diseases
21. Eliem Therapeutics Announces Agreement to Acquire Tenet Medicines and Concurrent $120 Million Private Placement
22.Kyverna IPO adds to biotech momentum with $319M fundraise
23. AstraZeneca to Acquire Gracell Biotechnologies, Strengthening Its Cell Therapy Portfolio in Oncology and Autoimmune Diseases
24. Selecta Biosciences Announces Merger with Cartesian Therapeutics
25.NKARTA receives FDA clearance of IND application for NKX019 in lupus nephritis.
26.Nkarta Announces Pricing Of $240 Million Underwritten Offering
27. Cabaletta Bio Announces Closing of $100 Million Public Offering of Common Stock
28. Three-step cures for autoimmune diseases?
29.An open-label, single arm, multicenter study to evaluate relmacabtagene autoleucel, the CD-19 directed CAR-T cell therapy, for active systemic lupus erythematosus in China
30. Charging towards the next-generation of CAR-T – Novartis website
31. Poltreg Investor Presentation (Original source unknown)
32. Xunlu Bio and Cabaletta Bio Jointly Announce Global Exclusive License Agreement for Clinically Validated CD19 Sequence
33. Timothy A. Springer, PhD – Harvard University faculty profile