First-in-Class TCR-T Therapy Tecelra Approved: Navigating Commercialization Challenges Beyond CAR-T Pitfalls

Adaptimmune
T Cell Therapy Developer
In August, two milestone events occurred in the TCR-T field.
First, the TCR-T cell therapy Tecelra (afami-cel), developed by Adaptimmune, received FDA approval for the treatment of synovial sarcoma, making afami-cel the first TCR-T therapy approved for treating solid tumors. Subsequently, Xiange Pharmaceutical’s TAEST16001 injection was included in China’s Breakthrough Therapy Designation list for the indication of advanced soft tissue sarcoma, becoming the first TCR-T cell therapy in China to receive IND approval for clinical trials.
The regulatory approval and market launch of TCR-T therapy also signify that this emerging technology has transitioned from the clinical stage to the commercialization stage, injecting a “shot in the arm” into the TCR-T sector and significantly boosting industry confidence.
In the past two years, multinational corporations (MNCs) have also entered the TCR-T space. In November 2022, AstraZeneca announced the acquisition of Neogene Therapeutics, a company focused on developing TCR-T therapies, for $320 million. In addition to making multiple rounds of investments in TScan, which specializes in TCR-T therapies, Novartis has established a collaboration worth hundreds of millions of dollars with TScan to jointly develop TCR-T cell therapies targeting multiple novel antigens. In July 2023, Bristol Myers Squibb (BMS) made an additional investment of $35 million in Immatics, a company in the TCR-T therapy field. This August, China’s Northeast Pharmaceutical Group announced its plan to acquire a 70% equity stake in Beijing Dingcheng Peiyuan, a cell therapy company.
The entry of numerous multinational corporations (MNCs) underscores their strong confidence in the TCR-T sector, yet challenges encountered during the development of CAR-T therapies in recent years have left the market skeptical about the prospects of TCR-T. With the recent approval of a new therapy, we may now reconsider the commercialization pathway for TCR-T.
Approval is only the beginning; the key lies in how afami-cel delivers on its commercial value.
Since the procedures for TCR-T and CAR-T therapies are largely similar, their fundamental approach involves extracting the patient’s blood, isolating and purifying T cells from it, genetically modifying these T cells in vitro to enable specific recognition of target antigens—thereby generating CAR-T or TCR-T cells—culturing and expanding the engineered cells in vitro, and finally infusing them back into the patient.
In other words, the challenges encountered in the commercialization of CAR-T therapies are highly likely to be faced by TCR-T therapies as well.
Adaptimmune (ADAP), founded in 2008, was listed on the Fierce 15 a decade ago and has since gained substantial insight into its significance through years of market experience. Starting in the first half of 2024, ADAP has invested $114 million in building its commercialization team and authorized treatment centers, with plans to commit a comparable amount over the next 18 months to support the commercial operations of afami-cel.
Following the approval of afami-cel, ADAP has launched the first batch of 6 to 10 authorized treatment centers, five of which are already operational. In the coming years, ADAP plans to establish approximately 30 authorized treatment centers across the United States, covering around 80% of synovial sarcoma patients nationwide.
ADAP’s management expects that the relevant sales revenue from afami-cel will begin to be reflected in financial reports starting in Q4 2024, with revenue acceleration anticipated in 2025. Although the initial promotion of afami-cel is focused on the United States, ADAP’s management is committed to launching afami-cel in Europe and expanding its therapeutic indications to other HLA types and sarcomas.
This is because the patient population for the approved indications is relatively small.
According to public data, there are approximately 13,000 new cases of soft tissue sarcoma annually in the United States, with synovial sarcoma accounting for about 5%–10% of these cases. The patient pool becomes even smaller after screening based on HLA-A genotype and MAGE-A4 expression levels. Considering factors such as the therapy’s price tag of $727,000 and the FDA’s black box warning, Adaptimmune’s management projects peak sales for afami-cel at only $400 million.
Clearly, the $400 million in revenue was insufficient to cover ADAP’s commercialization investments, prompting company management to pin its growth strategy on the expansion into subsequent indications.
Currently, another advanced pipeline candidate of ADAP, lete-cel, is in Phase II clinical trials, with indications for synovial sarcoma and myxoid round cell liposarcoma. According to its Phase I clinical data, among 73 patients treated with lete-cel, 45 were evaluable for efficacy, achieving an objective response rate (ORR) of 40%, with a median duration of response of 10.6 months. ADAP predicts that the peak sales of lete-cel may be slightly higher than those of afami-cel, with a projected revenue split of 40% for afami-cel and 60% for lete-cel.
If afami-cel and lete-cel are merely the pioneers, then ADAP’s true high hopes rest on uza-cel. Its primary indication, platinum-resistant ovarian cancer, has already entered Phase II clinical trials, and the patient population for this indication is substantially larger than that of the previous two pipelines. According to data from the American Cancer Society (ACS), there were more than 21,000 new cases of ovarian cancer in the United States in 2021 alone, making ovarian cancer the leading cause of death among gynecologic cancers in the country. Furthermore, uza-cel is being developed for urothelial carcinoma and head and neck cancer, both currently in Phase I clinical trials.
As can be seen, although afami-cel achieved first-in-class status, a qualitative leap in commercialization may only become evident upon the approval of uza-cel. The question remains: can ADAP hold out until that day?
In the development of new targets and novel technological approaches, cases of early starters ultimately lagging behind are commonplace.
Shortly after the approval of afami-cel, Adaptimmune released its interim report. As of the end of June 2024, Adaptimmune held approximately $200 million in cash, with fixed assets under $50 million, and reported a current period loss of approximately $100 million, indicating that its cash reserves may only suffice until next year. In response, Adaptimmune entered into a collaboration agreement with Galapagos regarding uza-cel for the indication of head and neck cancer. Under this agreement, Adaptimmune is eligible to receive a $100 million upfront payment, a $100 million option exercise fee, and up to $460 million in various milestone payments.
For biotech companies, tight funding is the norm. It takes at least two to three years of market cultivation to successfully commercialize a drug, raising questions about whether subsequent pipeline candidates can keep pace and whether the company itself can sustain operations. Being acquired by a multinational corporation (MNC) may be one viable path. Prior to this, Roche, GSK, and Astellas had all collaborated with Adaptimmune, but ultimately chose to part ways.
The recent volatility in ADAP’s stock price also reflects market sentiment. Following the approval of afami-cel, ADAP’s share price fell for five consecutive days, plunging nearly 20% on the day of approval, before trading sideways for another five days. It then rebounded by 18% after the release of the mid-year report, highlighting the market’s ambivalence.
Perhaps we can extrapolate the development of TCR-T therapy from that of CAR-T.
The first approved CAR-T therapies were Novartis’s Kymriah and Gilead’s Yescarta in 2017. Based on the newly released interim financial report data, Kymriah’s sales in the first half of 2024 amounted to $233 million, a 12% year-on-year decrease, with its peak sales likely to cap at $500 million. In contrast, Gilead’s Yescarta is projected to reach $1.6 billion in sales this year, with estimated peak sales exceeding $2 billion.

Latest Revenue Performance of Mainstream CAR-T Therapies Abroad, Based on Corporate Financial Reports
BMS received approval for two CAR-T therapies in 2021: Breyanzi, targeting CD19, and Abecma, targeting BCMA. Their respective sales are projected to reach $500 million and $400 million this year. Notably, Abecma’s sales declined by 37% compared to the first half of last year. In contrast, Johnson & Johnson’s Carvykti generated $133 million in revenue shortly after its approval in 2022, surged by 276% to $500 million in 2023, and rose another 81% year-over-year to $343 million in the first half of 2024. It is expected to cross the $1 billion annual sales threshold in 2025, just three years after its market launch.
Given that CAR-T therapies are generally priced at around $400,000, achieving $1 billion in sales would be considered an outstanding performance. Currently, only Gilead’s Yescarta and Johnson & Johnson’s Carvykti appear capable of reaching this milestone.
Carvykti, co-developed by Johnson & Johnson and Legend Biotech, has demonstrated excellent clinical data and is considered best-in-class. The most significant reason why Gilead’s Yescarta has surpassed Novartis’ Kymriah in sales may lie in the differences in efficacy.
According to FDA label data, Yescarta demonstrates a complete response (CR) rate of 65% and an overall response rate (ORR) of 83%, with the incidence of grade 3 or higher cytokine release syndrome (CRS) at 9%. In contrast, Kymriah reports corresponding figures of 32% for CR and 50% for ORR, while the proportion of grade 3 or higher CRS stands at 48%. This indicates that, given comparable pricing, therapies offering superior efficacy and a more favorable safety profile regarding CRS are naturally more marketable.
On the other hand, various CAR-T therapies are striving to expand their indications. Whether it is the sales-leading Carvykti, or Abecma and Breyanzi, which are currently lagging behind, as well as the domestically produced zevorcabtagene autoleucel, all have received approval for clinical trials of new indications in the first half of this year.
Overall, in recent years, only Gilead and Johnson & Johnson have truly emerged as leaders in the CAR-T sector, achieving strong commercial performance. Products with limited clinical value are seeing their markets shrink. Meanwhile, companies—whether leading or temporarily lagging—are committed to expanding indications in an effort to unlock larger market opportunities.
In contrast to the arduous and slow expansion of CAR-T therapy from hematologic malignancies to solid tumors, TCR-T therapy offers a more accessible pathway for identifying corresponding targets in solid tumors. This is because TCR-T cells rely on effective interactions with specific MHC molecules to mediate immune-mediated tumor cell killing. The advantage of MHC molecules lies in their ability to present intracellular antigens on the cell surface, thereby not being limited to antigens expressed solely on the surface of tumor cells, unlike CAR-T therapy.
Simply put, while CAR-T therapy is limited to recognizing antigens on the surface of cancer cells, TCR-T therapy can target intracellular antigens within cancer cells. Therefore, TCR-T holds greater promise in the treatment of solid tumors. Furthermore, TCR-T demonstrates superior advantages in terms of stability and safety.
According to WHO data, there were approximately 19.758 million new cancer cases globally in 2021, including about 1.305 million new cases of hematologic malignancies, accounting for less than 10%, while the remaining 90% consisted of new solid tumor cases. The market sizes for these two categories are not on the same order of magnitude. With the subsequent approval of TCR-T therapies, the disparity in their growth potential is expected to widen further.
In other words, the success or failure of TCR-T therapy may not depend solely on ADAP’s first-mover advantage, but rather on the number of companies subsequently entering the field and the extent of their indication coverage.
Despite the potential for TCR-T therapies to face the same commercialization challenges as CAR-T therapies, this has not deterred Chinese companies from making strategic investments in the field.
Concurrently with the approval of Adaptimmune’s product, Xiangxue Pharmaceutical’s TCR-T therapy, TAEST16001, was included in China’s Breakthrough Therapy Designation list, positioning it to potentially become the first marketed TCR-T therapy in the country.
Not only Xiangxue Pharmaceutical, but there are also about 20 companies in China that have laid out the TCR-T track. From the perspective of indications, it includes various solid tumors such as advanced soft tissue sarcoma, ovarian cancer, head and neck cancer, gastric cancer, liver cancer, and non-small cell lung cancer. Compared with CAR-T, which started from hematologic malignancies and struggled to expand into solid tumors, TCR-T therapy has more prospects.
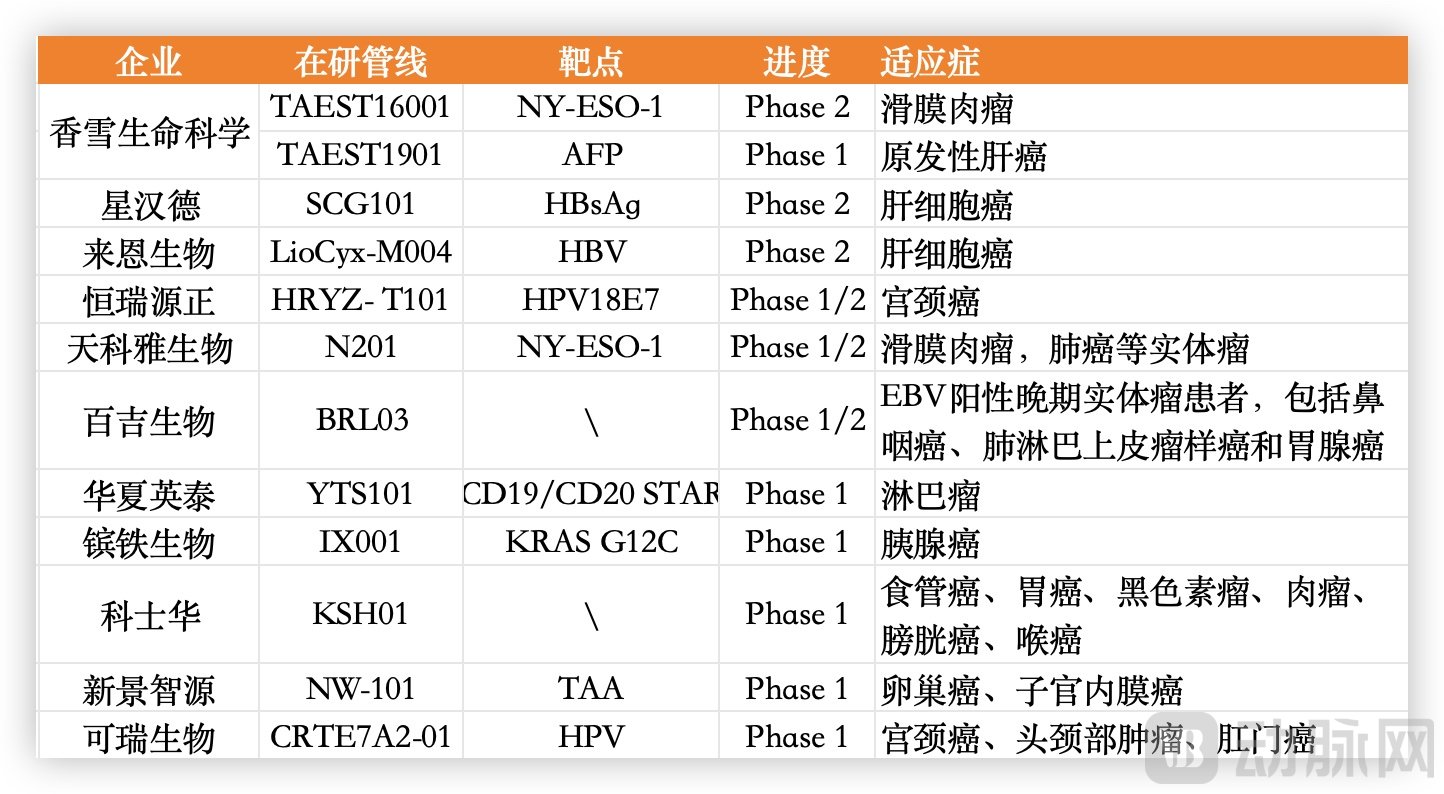
TCR-T Product Pipelines in Clinical Trials in China, Data Sourced from Company Websites
Companies such as Star-Hans Biotech, Layline Bio, Xiangxue Pharmaceutical, and Hengrui Yuanzheng are at the forefront of R&D progress, with each having pipeline candidates that have entered Phase II clinical trials. For instance, Layline Bio’s lead product, LioCyx-M, is an HBV-specific TCR-T cell therapy that uses mRNA technology to encode T-cell receptors for the treatment of hepatocellular carcinoma. Previous clinical data showed a duration of response of 27.7 months and a median overall survival of 33 months, leading to the granting of Fast Track designation by the U.S. FDA.
It is evident that numerous domestic companies in China have established TCR-T drug development platforms with independent intellectual property rights, extensively deploying pipelines for multiple solid tumors, with increasingly diversified targets for TCR-T cell therapies under investigation. In terms of indications, there is a substantial number of product pipelines targeting HPV-associated tumors and liver cancer. Regarding candidate product development, companies are employing innovative technologies, including mRNA technology and gene editing, to enhance the safety and efficacy of candidate products, while also exploring both viral and non-viral vectors.
Overall, the approval of the first TCR-T therapy signifies that the regulatory pathway has been cleared, and Adaptimmune, as a pioneer, will drive further exploration in commercialization. Meanwhile, the extensive deployment of TCR-T therapies in China has laid a solid foundation for future development.
Although CAR-T therapies with annual sales exceeding $1 billion have set a high benchmark, the landscape in China is quite different.
To date, five CAR-T therapies have been approved for marketing in China, with prices ranging from RMB 999,000 to RMB 1.29 million. Among these, only Relma-cel (Beinuoda) from JW Therapeutics has disclosed sales data. According to JW Therapeutics’ financial report, a total of 184 prescriptions for Relma-cel were issued in 2023, with 168 infusions completed, generating total revenue of RMB 174 million, a year-on-year increase of 19.3%. This performance shows a significant gap compared with similar products abroad.
The stark disparity in revenue stems from the fact that no CAR-T therapy has yet been included in the national medical insurance scheme. Although four CAR-T products passed the preliminary formal review for the 2024 National Reimbursement Drug List (NRDL), as announced by the National Healthcare Security Administration in its recent public notice, it remains exceedingly difficult for these million-yuan therapies to gain reimbursement coverage.
“Specialized therapies such as CAR-T are essentially unlikely to meet the criteria for inclusion in China’s national medical insurance scheme, given that the reimbursement environment for innovative drugs remains unchanged,” an industry insider told VCBeat. Companies have also recognized these challenges and have begun seeking solutions.
Earlier this year, Fosun Kite and Chenxi Health jointly launched an “Outcome-Based Payment Plan” for axicabtagene ciloleucel injection (Yikaida). For this CAR-T therapy, priced at RMB 1.2 million, patients who fail to achieve complete response after treatment will receive a refund of up to RMB 600,000. Yikaida thus became the first innovative biologic drug in China to adopt outcome-based payment. However, such an approach is more suitable for products with higher objective response rates (ORR); applying this model to products with relatively lower ORR would increase operational risks for companies.
While companies have begun exploring new outcome-based payment models, CAR-T therapy remains prohibitively expensive for most ordinary households. As a result, domestic CAR-T products are increasingly seeking coverage through commercial insurance as a viable pathway.
For instance, Healios Biopharma’s naxicabtagene autoleucel injection found a breakthrough through inclusive supplementary medical insurance channels. Last November, this therapy was included in Hebei Province’s Huiminbao (inclusive commercial health insurance), enabling reimbursement coverage of up to approximately 80%. Fosun Kite’s axicabtagene ciloleucel injection was also included in city-level Huiminbao plans across 100 provinces and municipalities, as well as in more than 70 commercial insurance products, by the end of 2023. Previously, relmacabtagene autoleucel had already been covered by over 50 commercial insurance products and 75 local government supplementary medical insurance schemes.
Despite extensive exploration, the actual reimbursement rate by insurance remains low. Currently, various commercial health insurance plans and inclusive supplementary medical insurance (Huimin Bao) cover approximately 30%–40% of costs, leaving the remainder to be borne by patients. For treatments costing millions, this still represents a significant financial burden.
The challenges encountered by CAR-T therapy are equally faced by TCR-T therapy.
For TCR-T therapies, as with CAR-T, the challenges of complex manufacturing processes and high costs persist. The cumulative burden across multiple stages—including production, process development, quality control, consumables, and equipment—has kept prices consistently high. To achieve commercial success, new cell therapies may need to address cost and pricing issues in a phased manner.
In the short term, innovations in payment models can bring about tangible changes. Whether through expanded insurance coverage or the emergence of novel payment mechanisms such as outcome-based pricing and lump-sum buyout arrangements, these measures can alleviate part of the financial burden on patients within a relatively short period. Historical trends indicate that intensified competition can also drive drug pricing adjustments. For instance, Kymriah, the first approved CAR-T therapy, was initially priced at $475,000 upon market approval. Following the approval of Gilead’s Yescarta, Kymriah’s price decreased by approximately 30% over the next year.
Next are the mid-term objectives. This phase primarily relies on process improvements, including automated production, reduced costs for QA and QC testing, enhanced transfection efficiency, and improved production efficiency. Taking T-cell engineering, the core step in CAR-T drug manufacturing, as an example, viral transduction is currently the most commonly used method. However, the production and quality control processes for viral vectors are complex, and the cost of custom-producing viral vectors is high. Therefore, the efficacy of viral vectors is critically important for cost control and can directly impact profit margins.
Finally, regarding long-term objectives, the key at this stage lies in technological breakthroughs. Currently, the high production costs of cell therapies, including CAR-T and TCR-T, are primarily driven by the need for large quantities of active T cells. Directly isolating highly active T-cell subsets could optimize the manufacturing process. Alternatively, transitioning from autologous to allogeneic (universal) cell therapies would eliminate the need for customized production, thereby disrupting the existing paradigm and significantly reducing costs.
In addition, there is a prevailing view in the industry that cell therapy companies should establish deep partnerships with hospitals to reduce intermediate links and thereby lower costs. Currently, after patients undergo leukapheresis at medical institutions, their samples must be transported to manufacturing facilities for sorting and purification, T-cell activation, gene transduction, ex vivo T-cell expansion, washing, formulation, cryopreservation, testing, release, and then shipped via cold chain back to the medical institutions for final infusion into the patients. If these processes could be centralized within hospitals by establishing in-house cell therapy centers, this might represent another viable model for commercial implementation.
Currently, major domestic TCR-T therapy companies are not only continuously innovating and breaking through at the technical level but also targeting overseas markets, with multiple firms having initiated international multicenter clinical trials. From a product perspective, TCR-T therapies directed against various solid tumors have broader development prospects compared to CAR-T therapies. From a commercialization standpoint, the key to the success of TCR-T lies in how to avoid the pitfalls encountered during the commercialization of CAR-T therapies.