Three Living Xenotransplantations in One Year Signal a Surge in Organ Transplant Innovation
In May this year, the First Affiliated Hospital of Anhui Medical University, in collaboration with Yunnan Agricultural University, successfully transplanted a genetically modified pig liver into a patient with severe liver cancer.
On postoperative day 7, the patient was able to ambulate freely. No hyperacute or acute rejection reactions were observed. The coagulation system was functioning normally, and liver function had returned to normal. Regarding the transplanted porcine liver, approximately 200 mL of golden-yellow bile was secreted daily. CT and ultrasound confirmed that blood flow in the hepatic artery, portal vein, and hepatic veins of the graft was entirely normal.
This is the fifth living xenotransplantation case worldwide, with three of these cases occurring in 2024 alone.
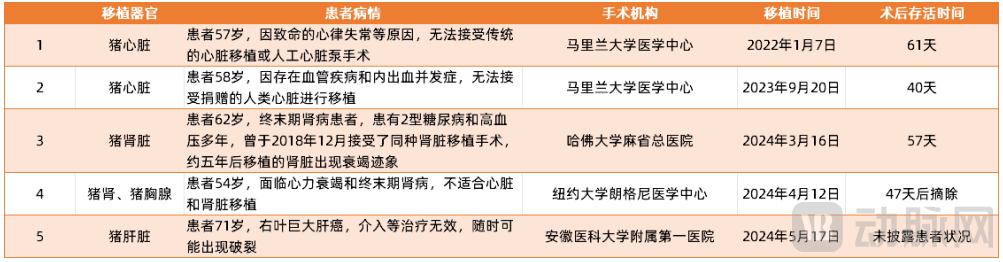
Five Cases of Living Allogeneic Organ Transplantation from 2022 to 2024
In addition to living-subject experiments, transplantation trials involving deceased human bodies are also accelerating. In March this year, a team from Xijing Hospital of the Air Force Medical University separately transplanted multi-gene-edited pig livers and kidneys into two brain-dead human recipients, with both organs functioning normally for a certain period post-operatively. Similarly, the First Affiliated Hospital of Kunming Medical University collaborated with Yunnan Agricultural University to conduct a combined liver-kidney xenotransplantation experiment from pigs to brain-dead human recipients, which also achieved promising progress.
Amid a surge in clinical trials, organ transplantation appears to be on the verge of a technological leap.
Broadly defined, organ transplantation is not limited to xenotransplantation (from animals to humans); it also includes allogeneic transplantation (from human to human), a technically mature procedure in which viable donor organs are surgically transferred into patients to replace organs that have lost their function.
Currently, transplantation of most major organs—including the heart, lungs, liver, kidneys, pancreas, small intestine, and skin—has been achieved. Furthermore, tissue transplantation, such as corneal and vascular grafts, is also widely applied in clinical practice.
However, the current organ transplantation industry is far from mature. Taking kidney transplantation, the most common procedure, as an example, it is the preferred treatment option when feasible in cases of bilateral renal failure or when chronic renal insufficiency progresses to end-stage renal disease. Furthermore, compared with peritoneal dialysis and hemodialysis, kidney transplantation offers significant advantages in terms of long-term survival rates, quality of life, and treatment costs.
However, since kidney transplantation primarily relies on histocompatibility matching, many patients pass away without ever receiving treatment due to the scarcity of donor kidneys and unsuccessful matches.
According to international organ donation and transplantation registry data, more than 345,400 patients were still waiting for organ transplants by the end of 2020. In that year alone, 23,103 patients on the waiting list died regretfully without receiving a kidney transplant.
Another set of data more directly illustrates the current situation: among the over 2.66 million patients with end-stage renal disease (ESRD) undergoing dialysis worldwide, only 5.65% are able to receive a kidney transplant.
To address this challenge, countries around the world are promoting the improvement of industry-related laws and regulations, establishing a more transparent and fair organ donation and transplantation system. By streamlining relationships, clarifying legal frameworks, and accelerating public education, these efforts aim to foster proper public understanding of organ transplantation, thereby encouraging greater participation in organ donation.
For instance, countries with high organ donation rates per million population, such as Spain and France, implement an "opt-out" system, whereby individuals who have not explicitly refused donation during their lifetime are presumed to be organ donors; most U.S. states have adopted a system in which individuals register their willingness to donate organs when applying for a driver’s license.
In China, the Regulations on Human Organ Donation and Transplantation, issued by the State Council, officially came into effect on May 1 this year, further standardizing the organ transplantation industry. Compared with the Regulations on Human Organ Transplantation implemented in 2007, the new regulations add the word “donation,” highlighting the importance of organ donation and strengthening incentives and guidance for organ donation.
Meanwhile, the organ transplantation industry continues to evolve, striving to maximize the survival rate of ex vivo organs.
Currently, the mainstream mechanical perfusion techniques for liver preservation and transportation are divided into two technical pathways: normothermic perfusion and hypothermic perfusion, which can serve different donor types and treatment scenarios.
Normothermic Machine Perfusion (NMP) of the liver maintains perfusion temperatures at 35–38°C, keeping the organ in a state of physiological metabolism with high oxygen consumption; therefore, oxygenated blood products are required for perfusion. Its advantages include the ability to assess liver quality via bile production and lactate clearance rates, offering potential for therapeutic delivery applications in the future. Disadvantages include the risk of secondary hepatic ischemia even from brief interruptions in perfusion, risks associated with blood products, operational complexity, and high perfusion costs.
Hypothermic Machine Perfusion (HMP) of the liver maintains perfusion temperatures between 0–12°C, suppressing hepatic metabolism under hypothermic conditions. Its advantages include enhanced hepatic tolerance to ischemia at low temperatures, reduced incidence of postoperative biliary complications caused by ischemia, and prevention of warm ischemic injury and functional loss due to brief technical failures. A disadvantage is that there are fewer indicators available for assessing liver function under hypothermic conditions compared with Normothermic Machine Perfusion (NMP).
Among the commercially available liver mechanical perfusion devices worldwide, Transmedics and OrganOx both utilize NMP technology, while XVIVO employs a temperature-controlled perfusion system. In China, the mechanical perfusion systems from Jiankeng Medical, Qidian Medical, and Lapusheng all adopt HMP technology.
Notably, JianGeng Medical’s LifePort Kidney Transport Box is used by hundreds of Organ Procurement Organizations (OPOs) or transplant centers across nearly 40 countries and regions. Among the 57 OPOs in the United States, 54 utilize LifePort products for mechanical perfusion of donor kidneys, securing the leading market share.
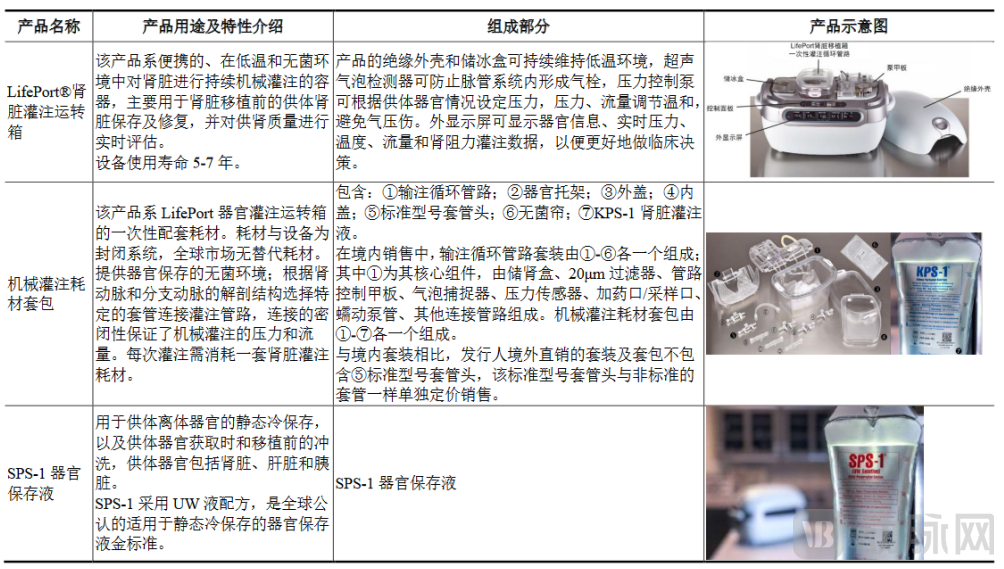 Jiankeng Medical LifePort Product Portfolio
Jiankeng Medical LifePort Product Portfolio
Singularity Medical has established an in-depth collaboration with the First Affiliated Hospital of Sun Yat-sen University to launch the “Ischemia-Free Liver Perfusion System.” This system provides blood and oxygen supply to ex vivo organs, maintaining normal liver physiological function without interrupting blood flow. It overturns the traditional method of static cold storage for organs, significantly mitigates ischemia-reperfusion injury in donor organs, markedly improves transplant prognosis, and propels organ transplantation into the “era of warm transplantation.”
Furthermore, the company has directed its technological breakthroughs toward kidney sources by launching the “Organ Saver” device. This device enables the use of organs from donation after circulatory death (DCD)—a source previously inaccessible through conventional methods—potentially increasing the organ supply by more than 50% and alleviating the shortage of donor organs.
Although various innovations centered on ex vivo organ preservation have effectively improved the five-year survival rate of transplant recipients and, to some extent, expanded the supply of viable donor organs, xenotransplantation remains the fundamental solution to bridging the substantial gap between organ demand and availability.
In preclinical studies using non-human primate models, the kidney and heart are considered the most suitable organs for xenotransplantation. Following CRISPR-mediated genomic editing of the donor pig to knock out antigen-encoding genes, insert human genes, and eliminate porcine endogenous retroviruses, the pig kidney survived for 758 days in a cynomolgus monkey recipient.
In terms of cardiac transplantation, the longest survival time for orthotopic heart transplantation (removal of the recipient's heart) is 264 days, while the record for heterotopic heart transplantation (leaving the recipient's own heart in place) has reached nearly 1,000 days.
However, postoperative survival rates remain unsatisfactory, both in the five cases of living xenotransplantation mentioned above and in human-to-human organ transplants.
Excluding the xenogeneic liver transplantation performed by the First Affiliated Hospital of Anhui Medical University, for which treatment outcomes have not yet been disclosed, the longest survival time among patients undergoing other living-donor xenogeneic organ transplantations was only 61 days. Data on allogeneic transplantation presented in the USRDS 2021 Annual Report indicate that the ten-year survival rates after kidney transplantation from deceased donors and living donors were 49.5% and 65.5%, respectively, highlighting substantial room for improvement.
Infection is the most common cause of early mortality after kidney transplantation, associated with factors such as excessive postoperative immunosuppression, malnutrition, and postoperative complications. Taking excessive immunosuppression as an example, in patients who have undergone kidney transplantation, insufficient immunosuppression may lead to rejection, resulting in structural damage to the graft, loss of graft function, and difficulties in re-transplantation; conversely, excessive immunosuppression increases the risk of infection and malignancy.
Furthermore, while commonly used immunosuppressants (such as cyclosporine, tacrolimus, and mizoribine) provide stable therapeutic efficacy, they are associated with drawbacks including frequent adverse reactions and limited treatment options. In addition, the high cost of biologic immunosuppressants imposes a significant financial burden that, to some extent, hinders the postoperative recovery of surgical patients.
Therefore, long-term, continuous care and support are crucial for such patients. Physicians need to continuously monitor and adjust the patient’s immune status and the condition of the transplanted organ to detect and address issues as early as possible. On the other hand, the industry should also actively explore novel immunosuppressive agents to strike a new balance between therapeutic efficacy and health economics.
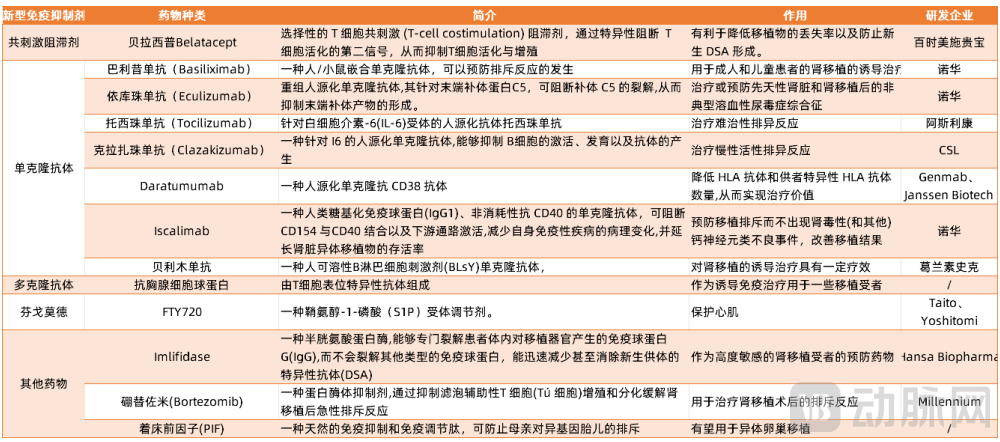 Inventory of Potential Novel Immunosuppressants
Inventory of Potential Novel Immunosuppressants
In contrast, approximately 30 genes are associated with xenotransplantation rejection, making the rejection response more complex and difficult to overcome. Furthermore, the immunosuppressive regimens required are more intensive than those for allotransplantation, exerting a greater impact on the human immune system. This increases the risk of innate immune system compromise and subsequent infection, potentially leading to severe complications.
In the world’s first two cases of xenotransplantation, Revivicor performed 10 genetic edits on the donor pigs. Three genes that trigger rapid antibody-mediated rejection in humans were knocked out, and six genes associated with immune rejection of human hearts—CD46, CD55, thrombomodulin, endothelial protein C receptor, CD47, and heme oxygenase-1 (HO-1)—were inserted into the porcine genome to minimize the likelihood of rejection.
eGenesis, founded by gene-editing pioneer George Church, bred genetically modified pigs for the world’s third living-human xenotransplantation procedure. These pigs underwent 69 genomic edits: three genes involved in the synthesis of porcine cell-surface glycan antigens were knocked out, and seven human genes related to rejection modulation were inserted to help porcine cells evade scrutiny by the human immune system. Additionally, the company inactivated porcine endogenous retroviruses (PERVs) in the donor pigs to reduce the risk of human infection.
However, the results indicate that the efforts of various companies in gene editing have not fully resolved the issue; xenograft rejection remains the ultimate hurdle to allogeneic organ transplantation.
In response to this challenge, startups such as NZeno in New Zealand, Xtransplant in Germany, and China’s Zhongke Aoge and Gelande Biologics have actively entered the field, cultivating donor pigs for xenotransplantation and achieving remarkable results. Specifically, they employ gene-editing technologies to create low-immunogenicity donor pigs, develop transplantable porcine red blood cells, skin, kidneys, and other tissues and organs, and expand the application of gene-edited donor pigs in biomaterials and regenerative medicine, thereby driving the development of China’s allogeneic organ transplantation industry.
As one of the three great miracles in the medical field, organ transplantation has most fully realized the dream of extending human life with high quality. However, extension is not the ultimate goal of modern medicine; tens of thousands of researchers, physicians, and patients are engaged in this endeavor to enable future transplant recipients to achieve a true rebirth.
Achieving such a breakthrough will inevitably involve countless failures, yet each failure holds its own significance. As the family of David Bennett, the recipient of the world’s first pig heart transplant, stated:
“We are grateful for every moment of innovation, every audacious dream, and every sleepless night, extending our thanks to all who contributed to this historic surgery. We hope this story marks the beginning of hope, not its end.”
Standing on the brink of a quantum leap in organ transplantation technology, we may be on the verge of witnessing hope itself.