Humacyte's SYMVESS: The First FDA-Approved Tissue-Engineered Vascular Graft Set to Transform a $10B+ Market After Two Decades of Development

Humacyte
Developer of Vascular Disease and Anatomical Catheter Replacement Products
On December 19, 2024, the U.S. Food and Drug Administration (FDA) approved the marketing of the world’s first true tissue-engineered product—Humacyte, Inc.’s SYMVESS tissue-engineered vascular graft (6 mm inner diameter)., the first indication for this product is for adult patients requiring emergency revascularization due to traumatic injury of the lower extremity arteries, thereby avoiding amputation; this includes various types of trauma such as motor vehicle accidents, gunshot wounds, blast injuries, and industrial accidents.
In the future, this tissue-engineered blood vessel could be expanded to cover more indications, including establishing vascular access for hemodialysis in chronic renal failure, carotid artery reconstruction, lower extremity atherosclerosis, and coronary artery bypass grafting.
Small-diameter (inner diameter ≤6 mm) synthetic vascular grafts have recently emerged as a focal point of medical device research, development, and innovation in China. Although the Chinese market is well supplied with polymer-based synthetic grafts, such as expanded polytetrafluoroethylene (ePTFE) grafts, two major limitations of small-diameter ePTFE grafts have remained unresolved for five decades: First, poor biocompatibility prevents luminal endothelialization, predisposing to thrombosis and resulting in low long-term patency rates. Second, host cells fail to infiltrate the graft after implantation, precluding vascular wall remodeling; consequently, clinical use—particularly in dialysis access—is associated with an elevated risk of infection.
These two major shortcomings severely compromise clinical outcomes. Particularly in China, some patients experience acute thrombotic occlusion before discharge following ePTFE vascular graft implantation, leading to fear and distrust among both physicians and patients toward these products. This also significantly increases healthcare expenditures; although U.S. insurance coverage ensures payment, it still imposes a substantial economic burden.
The advantages of tissue-engineered vascular grafts lie in their unique regenerative properties, which enable rapid endothelialization of the lumen and recellularization of the vessel wall after implantation, thereby significantly improving long-term patency rates and providing resistance to infection.
The primary mechanisms of in vivo regeneration are as follows: Tissue-engineered vascular grafts are fabricated by seeding cells onto biodegradable polymeric tubular scaffolds and culturing them in vitro. Within 3 to 6 months after implantation, complete endothelialization of the lumen is achieved; endothelial cells constitute the most critical structure within the human vascular lumen for preventing thrombosis. Concurrently, host autologous mesenchymal stem cells migrate into the graft wall and naturally differentiate into vascular smooth muscle cells under pulsatile flow conditions. Consequently, approximately six months post-implantation, a neovessel resembling a native artery is regenerated.
The approval of this product is revolutionary in the field of tissue engineering and regenerative medicine, as it is the first successfully commercialized product since the concept was proposed in the mid-1980s.
Looking ahead, tissue engineering technology holds immense development potential and is expected to yield more regenerative medicine products—such as tissue-engineered heart valves, corneas, cartilage, and tracheas—bringing about disruptive transformations across multiple fields.

Key Milestones in the Development of Tissue-Engineered Vascular Grafts
Research and development of tissue-engineered artificial blood vessels began in the 1990s.In 1995, Dr. Laura Niklason, founder of Humacyte, an academician of the U.S. National Academy of Engineering and the U.S. National Academy of Medicine, and a professor in the Departments of Anesthesiology and Biomedical Engineering at Yale School of Medicine, was conducting postdoctoral research at Harvard University and MIT. During her clinical rotation as an anesthesiologist in the cardiovascular surgical intensive care unit (ICU) of a medical school hospital, Dr. Niklason learned that cardiac surgeons could only use patients’ autologous vessels, including the great saphenous vein, as conduit grafts for coronary artery bypass grafting (CABG) surgery.
In the 1980s and 1990s, more than 800,000 coronary artery bypass grafting (CABG) procedures were performed annually in the United States. Surgeons needed to make surgical incisions extending from the patient’s groin to the medial aspect of the ankle to harvest the great saphenous vein for bypass grafting. This procedure was extremely painful for patients and led to various postoperative complications. Furthermore, there was a lack of viable synthetic vascular substitutes available in clinical practice. This unmet clinical need motivated Dr. Laura Niklason to develop small-diameter artificial blood vessels.
Several well-known global manufacturers of synthetic vascular grafts, such as Gore and Bard, have used conventional technologies to develop ePTFE synthetic vascular grafts with inner diameters of 3.5 mm and 4 mm and anticoagulant coatings for coronary artery bypass grafting. However, due to inherent limitations in materials science, these grafts remain prone to thrombosis and occlusion, posing life-threatening risks to patients. As early as the 1980s, the American professional society for cardiac surgery prohibited the clinical use of such products, causing the development of small-diameter synthetic vascular grafts to stagnate.
To address this challenge, Dr. Laura Niklason decided to employ classical tissue engineering techniques to culture blood vessels in vitro—essentially allowing them to “grow” in the laboratory.Tissue engineering technology has provided a revolutionary new approach for the in vitro cultivation of artificial blood vessels: by seeding cells onto tubular biodegradable biomaterials, tissue-engineered blood vessels with morphology and performance closely resembling those of natural human blood vessels are constructed in vitro.
After implantation into the human body, tissue-engineered blood vessels undergo remodeling by autologous cells, including vascular endothelial cells and vascular smooth muscle cells, within a certain period. This process generates neointima that mimics native arteries, significantly improving vessel patency and performance. The material basis of tissue-engineered artificial blood vessels is essentially an acellular matrix product primarily composed of human vascular collagen. Compared with synthetic polymer materials, these scaffolds exhibit superior biocompatibility, which can greatly enhance long-term patency rates while providing resistance to thrombosis, infection, calcification, and intimal hyperplasia.
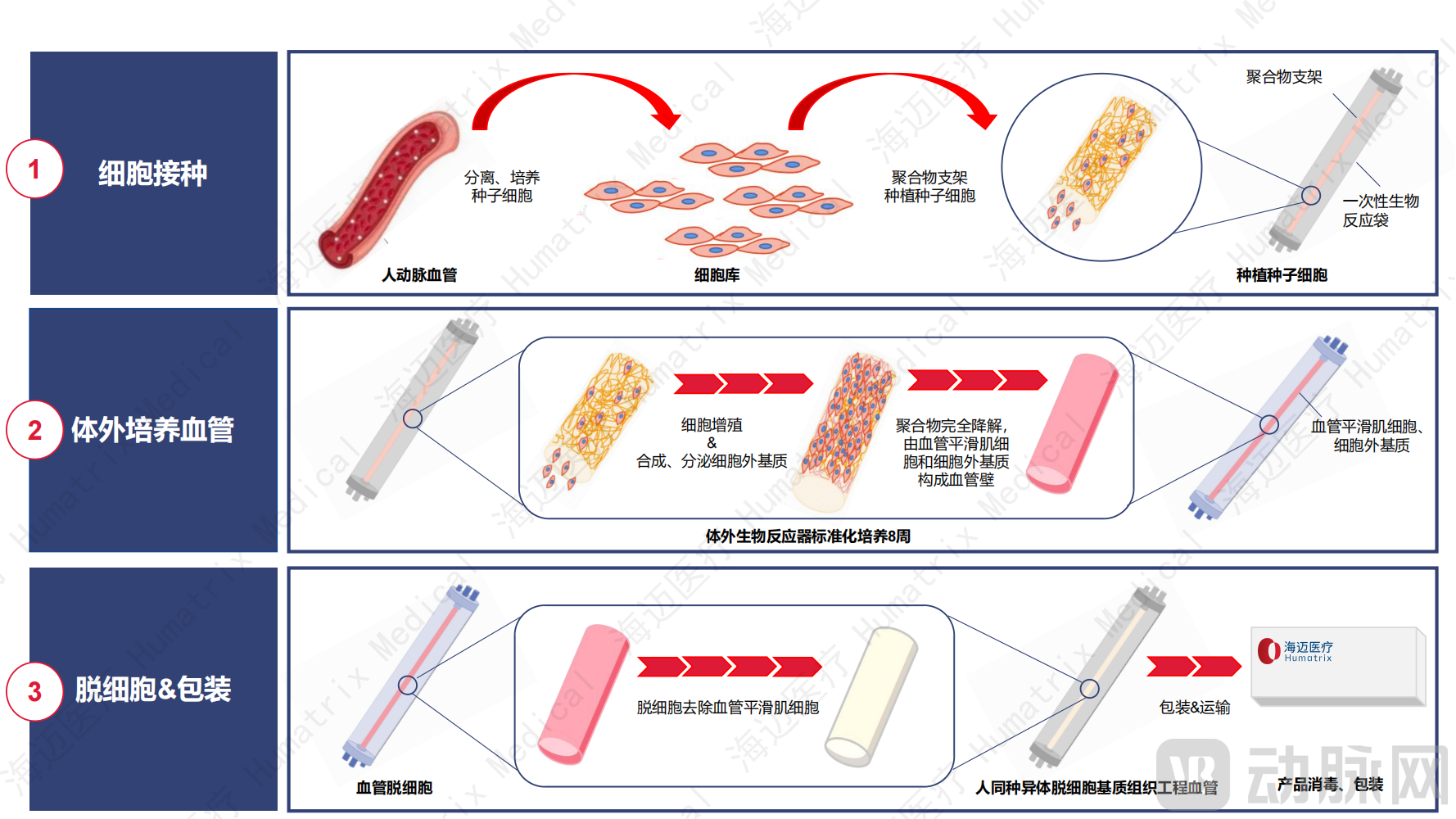 Process Flowchart of Tissue-Engineered Blood Vessels. Image source: Hymed Medical Technology (Suzhou) Co., Ltd.
Process Flowchart of Tissue-Engineered Blood Vessels. Image source: Hymed Medical Technology (Suzhou) Co., Ltd.
The Commercialization Journey of Tissue-Engineered Vascular Grafts: A Thirty-Year Odyssey. Transforming Laboratory Innovations into Market-Ready Products Is a Story Filled with Challenges and Breakthroughs.
Ideal tissue-engineered vascular grafts must meet multiple key technical specifications and performance criteria. First, they must possess excellent mechanical properties to withstand hemodynamic pressures and fluctuations after implantation. While polymeric materials can relatively easily be processed to achieve mechanically robust profiles that satisfy clinical requirements, it is considerably more challenging for tissue-engineered vascular grafts to attain comparable mechanical performance. Second, tissue-engineered vessels should have the capacity for self-regeneration and repair, enabling them to remodel into neovessels akin to native arteries after implantation. Finally, production cost is a critical factor that cannot be overlooked. Cytograft, after more than 20 years of research and development, developed a scaffold-free, autologous cell-based tissue-engineered vascular graft and conducted clinical trials in 10 patients. However, each production batch required 7–9 months, and the manufacturing cost per graft was $15,000. These prohibitive costs rendered commercialization unfeasible, leading the company to cease operations in 2015. Achieving these ideal performance attributes requires overcoming multiple technical barriers.
The Three Classic Elements of Tissue-Engineered Blood Vessels: Biodegradable Scaffold Materials, Seed Cells, Growth Factors, and Culture Conditions. Each Step Faces Significant Technical Challenges.Biodegradable scaffold materials require precise control over their degradation rate to adapt to changes in the culture environment. The source and quality of seed cells are equally critical, as their limited number of passages imposes stricter requirements for sustained industrial-scale mass production. Finally, simulating the entire process of vascular development and growth (akin to fetal development in utero) within a mere two months is a process that demands extremely high precision and control over growth factors and culture conditions.
Industry insiders pointed out: “The key to Humacyte becoming the first company to gain product approval lies in its selection of the correct technological pathway and its resolution of mass-production challenges. Traditional tissue engineering techniques produce blood vessels containing living cells, which cannot be stored or transported at room temperature; instead, they require cryopreservation in liquid nitrogen for delivery to the operating room. This approach incurs high costs, fails to meet the clinical requirement for ‘on-demand availability,’ and poses significant immunogenicity risks due to the presence of living cells, thereby presenting substantial commercialization challenges. Humacyte has effectively addressed these mass-production hurdles by decellularizing the living-cell-containing blood vessels while retaining the extracellular matrix. This eliminates the need for liquid nitrogen storage, enables transport to the operating room, and keeps production, storage, transportation, and usage costs within a reasonable range!”
In China, artificial blood vessel companies are experiencing strong growth momentum, with multiple enterprises actively engaging in the research and development of related technologies.China has adopted a dual-track strategy in the research and development of artificial blood vessels: on one hand, it is committed to developing polymer-based artificial blood vessels to achieve domestic substitution of existing imported products; on the other hand, it is actively advancing the R&D of next-generation tissue-engineered blood vessels, aiming for breakthroughs in the high-end medical sector. Companies engaged in the development of small-diameter artificial blood vessels include Haimai Medical, Lingbo Biotechnology, and Shanghai Changdi, among others. According to investigations, Haimai Medical is the only company in China that benchmarks against Humacyte’s technological approach. The company focuses on the development and production of small-diameter tissue-engineered blood vessels and initiated clinical trials in September 2024.
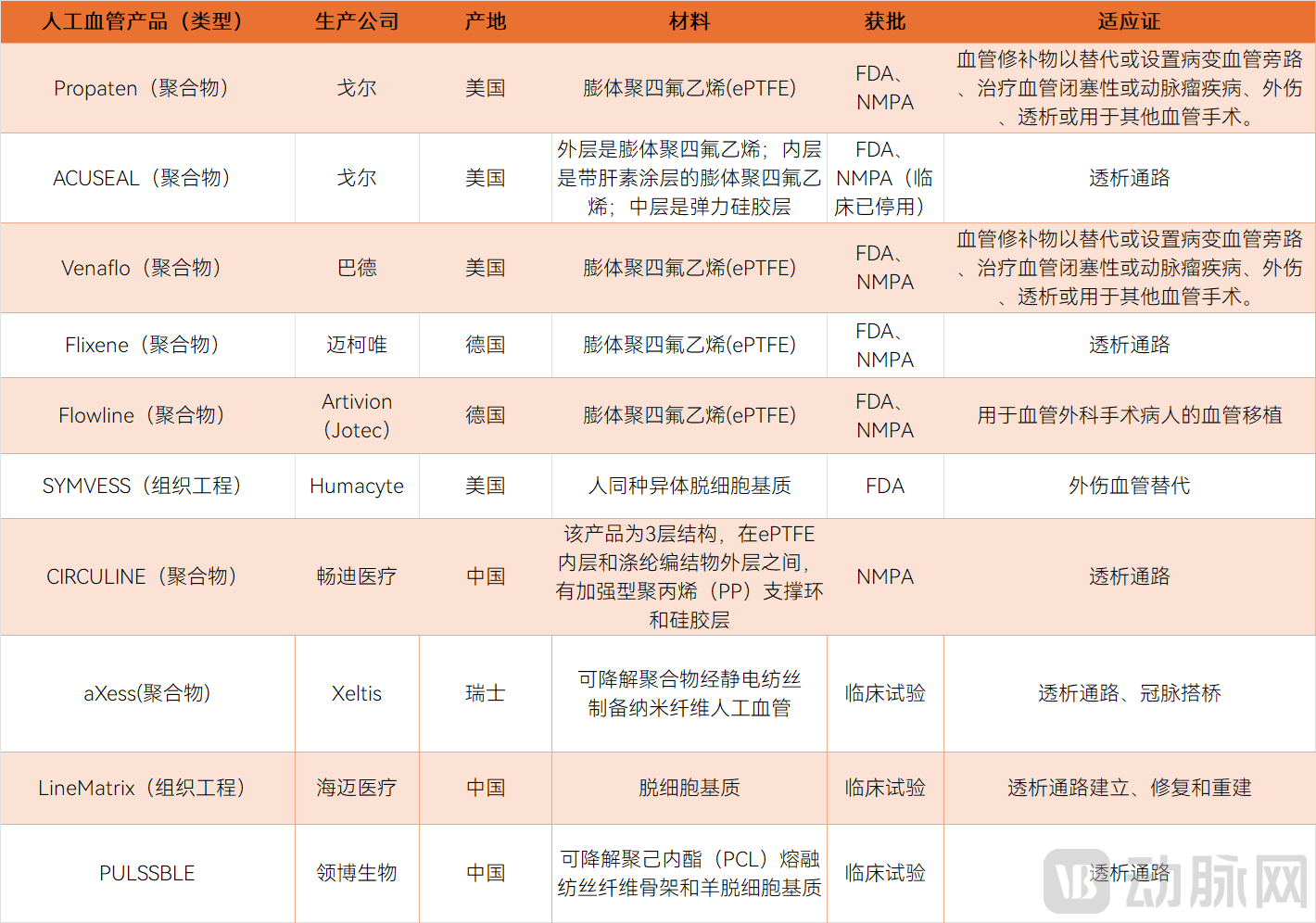
Selected Global Small-Diameter Artificial Vascular Grafts: Listed and In-Development
The approval of tissue-engineered blood vessels signals immense commercial potential. In the medical field, artificial blood vessels have a wide range of applications, including but not limited to: vascular replacement in trauma surgery, establishment of vascular access for hemodialysis in chronic renal failure, treatment of lower extremity atherosclerosis and coronary artery bypass grafting (CABG) surgery, as well as bioartificial pancreas development. These scenarios present substantial unmet clinical needs.
The first approved indication for tissue-engineered artificial blood vessels focuses on vascular replacement for traumatic lower extremity arterial injuries, a sector poised for rapid growth in the U.S. market.According to statistics, there are approximately 72,000 open surgical procedures for traumatic vascular replacement performed annually in the United States. This volume is supported by the country’s mature trauma care system, which has established a four-level trauma care network covering more than 580 trauma centers, indicating a broad market prospect. U.S. commercial insurance strongly supports innovative medical technologies through mechanisms such as the New Technology Add-On Payment (NTAP). Once superior products receive FDA approval, patients will have priority access to these enhanced treatments covered by commercial insurance. Given China’s large population base, the demand for traumatic vascular replacement is similarly substantial, and its market potential should not be underestimated. Meanwhile, rising global geopolitical tensions have increased the need for pre-war stockpiling or immediate use of small-diameter synthetic vascular grafts, making domestic substitution an urgent priority.
Another indication for tissue-engineered artificial blood vessels with substantial clinical demand is the arteriovenous vascular access for chronic renal dialysis.According to a 2024 report in JAMA, more than 3.5 million people worldwide are undergoing maintenance dialysis, with approximately 90% receiving hemodialysis. In 2021, 540,000 registered patients in the United States received maintenance hemodialysis. Data from China’s National Renal Dialysis Registry System (CNRDS) show that the number of registered hemodialysis patients in China was approximately 200,000 in 2012 and reached 916,000 by 2023, with more than 160,000 new cases added annually in recent years. This highlights the substantial clinical demand for tissue-engineered vascular grafts in this field.
The third major application scenario is lower extremity atherosclerosis.Regarding peripheral artery disease (PAD), according to Frost & Sullivan, the number of PAD patients in China is projected to increase from 52 million in 2021 to 62 million in 2030, representing a compound annual growth rate (CAGR) of approximately 2.1%. Globally, the number of PAD patients is expected to rise from 289 million in 2021 to 372 million in 2030, with a CAGR of approximately 2.8%. Currently, only 0.2% of patients undergo revascularization therapy. Although the volume of peripheral endovascular interventions is increasing year by year, concerns regarding long-term efficacy and the fact that many patients are not suitable candidates for endovascular procedures remain. Tissue-engineered vascular grafts offer higher long-term patency rates and superior clinical outcomes; consequently, the number of open surgical procedures utilizing artificial grafts is expected to increase steadily in the future.
The fourth major application scenario is coronary artery bypass grafting (CABG) surgery.Globally, there are no commercially available small-diameter vessels for coronary artery bypass grafting (CABG). In November 2024, Humacyte presented preclinical data on the use of its 3.5 mm tissue-engineered vascular grafts in an orthotopic CABG baboon model at the 100th American Heart Association (AHA) Scientific Sessions in the United States, with human registrational clinical trials expected to commence shortly. According to the 2023 White Paper on Cardiovascular Surgical Procedures and Extracorporeal Circulation Data in China, the annual number of CABG procedures in the country exceeds 70,000, with an average requirement of 2.5 conduit vessels per patient. Therefore, tissue-engineered vascular grafts hold broad application prospects and a substantial market potential in CABG surgery.
Humacyte’s stock price surged following the FDA approval of its product for market launch. However, analysts have since raised questions about the commercialization timeline and market size of its tissue-engineered vascular grafts.
From a health economics perspective, Humacyte’s SYMVESS human acellular vessel not only significantly improves clinical outcomes but also substantially reduces the additional medical expenditures associated with traditional ePTFE vascular grafts due to thrombosis or infection.
Professor Qiu Xuefeng, Founder, Chairman, and CEO of Humacy Medical Technology (Suzhou) Co., Ltd., stated: “In 2020, Laura Niklason, founder of Humacyte, published a paper in Nature Reviews Nephrology that analyzed the advantages of tissue-engineered vascular grafts from a health economics perspective. Although each ePTFE vascular graft is priced at $1,000–$4,000, the United States incurs approximately $4 billion in additional annual costs solely due to infections associated with dialysis access grafts, while medical expenditures for managing vascular thrombosis, stenosis, and other complications are far higher. In contrast, although Humacyte’s grafts are priced at $25,000 each, the total medical costs during clinical use are significantly reduced. Prior to receiving FDA approval, Humacyte had already been assigned four ICD-10-PCS reimbursement codes by the U.S. Centers for Medicare & Medicaid Services (CMS).”
The innovation of tissue-engineered artificial blood vessels lies not only in their replacement of traditional polymer-based grafts but also in their superior biocompatibility and capacity for self-repair and regeneration, thereby opening up new possibilities for their application across diverse medical scenarios.
Industry insiders point out, “After achieving breakthroughs in the field of tissue-engineered vascular grafts, the next major advancement in tissue engineering is expected to emerge in the field of tissue-engineered heart valves!”
Currently, artificial heart valves are primarily categorized into mechanical heart valves and bioprosthetic heart valves. The leaflets of mechanical heart valves are made of pyrolytic carbon, which exhibits poor biocompatibility. Although their service life can exceed 50 years, patients require lifelong anticoagulation therapy with warfarin. Warfarin anticoagulation necessitates frequent monitoring and is associated with numerous complications; in severe cases, it can lead to thrombosis or major hemorrhage, posing a life-threatening risk to patients. The leaflets of bioprosthetic heart valves are constructed from non-viable bovine pericardium or porcine heart valves. However, the chemical cross-linking process used in their manufacturing makes them prone to calcification, leading to valve degeneration and a limited service life of approximately 10–15 years. Both types of artificial heart valves lack the capacity for self-regeneration and repair within the body.
In comparison, tissue-engineered artificial heart valves possess unique self-repair and regenerative capabilities, enabling endothelialization of the leaflet surface and re-cellularization within the leaflets. They regenerate into living tissue after implantation, which can significantly extend valve service life and eliminate the need for long-term anticoagulation therapy.
Another promising direction in Humacyte’s pipeline is the use of tissue-engineered vascular grafts as carriers for islet transplantation to treat type 1 diabetes. Scientists have long been exploring cell-based therapies to achieve a complete cure for type 1 diabetes. Recently, Vertex Pharmaceuticals’ stem cell therapy VX-880, developed for type 1 diabetes, has entered pivotal Phase 3 clinical trials. However, stem cell-derived islets lack an optimal transplantation vehicle. Humacyte’s bioengineered pancreas, utilizing its tissue-engineered vascular graft technology, has completed preclinical studies in non-human primates (baboons).
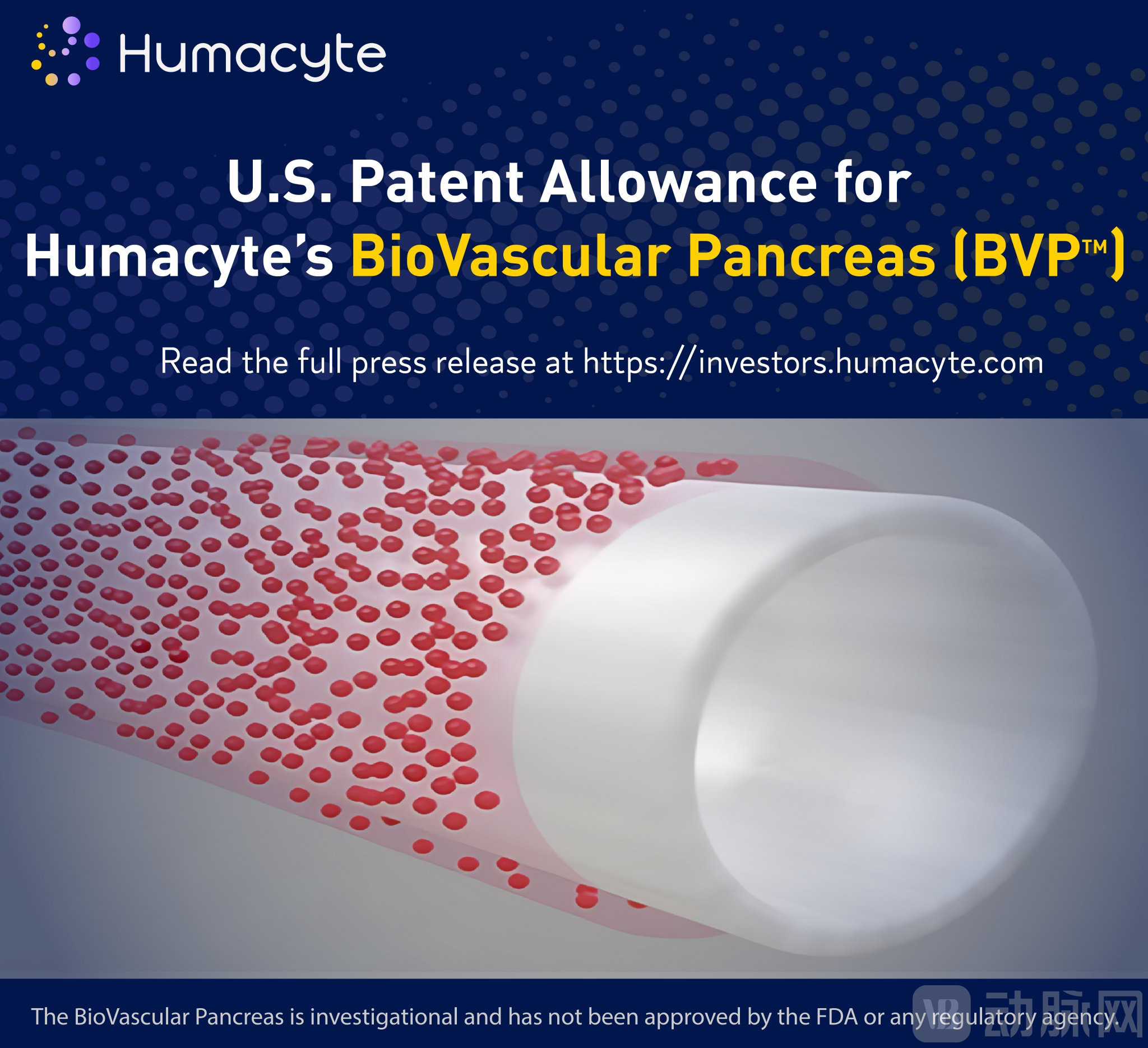
Schematic of Humacyte's Artificial Pancreas Product
Humacyte further collaborates with the Juvenile Diabetes Research Foundation (JDRF) to utilize tissue-engineered human acellular vessels as “carriers” for islet cell transplantation. By implanting these vessels between an artery and a vein, a fully functional bioengineered pancreas is regenerated in vivo, effectively regulating patients’ blood glucose levels and eliminating the need for long-term insulin injections.
Over the past three decades, tissue engineering has transitioned from the laboratory to commercialization, a journey marked by twists and turns—“filled with tears and embraces.” Looking ahead, we anticipate that tissue engineering will usher in a new chapter in regenerative medicine, spearheading a revolution in the regeneration of human tissues and organs.

Group photo of some members of the Vacanti and Langer laboratories (1995)
Reference: Breuer CK. The development and translation of the tissue-engineered vascular graft. J Pediatr Surg. 2011 Jan;46(1):8-17. doi: 10.1016/j.jpedsurg.2010.09.058. PMID: 21238633.