2025 Alzheimer's Disease Early Screening Industry Research Report: Two Breakthrough Therapeutics and 46 Blood-Based Diagnostic Kits Approved, Marking a Substantive Transformation in Early Detection
Early screening for Alzheimer’s disease (AD) is undoubtedly one of the most prominent niche sectors in the field of in vitro diagnostics (IVD) in 2024. AD is a neurodegenerative disorder characterized by an insidious onset and slow progression, and it represents the most common form of dementia. Previously, AD medications such as donepezil and rivastigmine offered only limited therapeutic benefits, primarily slowing disease progression rather than providing a cure. However, with the continuous growth of the elderly population, the increasing adoption of early screening and diagnosis concepts, breakthroughs in innovative diagnostic technologies such as blood-based tests, and a series of positive developments in the innovative AD drug sector since 2023 that have dispelled decades of setbacks and gloom, substantial opportunities for early AD screening have emerged.
Building on this foundation, VBInsight has authored the “2025 Industry Research Report on Early Screening for Alzheimer’s Disease,” with a primary focus on early AD screening. The report analyzes the clinical value and development trends of biomarkers and detection technologies for early AD screening, and explores product commercialization strategies.
Core Viewpoints:
Pain Points in Early Screening for Alzheimer’s Disease: Insufficient Public Awareness and Limitations of Screening TechnologiesThe burden of Alzheimer’s disease (AD) is substantial, making early screening an urgent priority. According to clinical feedback, the main challenges in early AD screening currently include insufficient public awareness of the disease, limitations in screening technologies, a scarcity of specialized institutions, and poor patient compliance. In particular, the widespread tendency to ignore early memory decline in the elderly results in missed opportunities for early intervention. Furthermore, AD diagnostic techniques currently used in clinical practice are either invasive, costly, or unable to accurately identify asymptomatic patients, leading to low compliance with early detection efforts.
Blood tests may be the most suitable AD detection technology for large-scale early screening.AD early screening products suitable for large-scale application should be evaluated across six dimensions: biomarker combinations, sensitivity, standardization, accessibility, early detection capability, and convenience. Overall, blood tests offer cost-effectiveness, non-invasiveness, repeatability, and accessibility, enabling the identification of patients in the ultra-early stages of AD, thus making them suitable for large-scale early screening of AD. Furthermore, the regulatory approval process for AD blood test products in China is advancing rapidly, with 47 AD blood test kits already approved by the National Medical Products Administration (NMPA).
PET imaging and cerebrospinal fluid testing are the “gold standards” for diagnosing Alzheimer’s disease (AD), but they are difficult to apply in large-scale early screening, and there are few imaging agent products approved in China.PET imaging is costly and equipment availability is limited. In China, only Aβ-PET imaging agents from Xiantong Pharmaceutical have received approval from the National Medical Products Administration (NMPA), while no tau-PET imaging agents have been approved yet. Cerebrospinal fluid testing is invasive and causes significant trauma; currently, only Roche’s products have been approved by the Hainan Provincial Medical Products Administration.
Leverage Early Screening as the Cornerstone to Accelerate the Development of a Comprehensive Industrial Ecosystem for Alzheimer’s Disease Diagnosis and Treatment.Currently, the domestic ecosystem for Alzheimer’s disease (AD) diagnosis and treatment is characterized by its niche nature, low volume, and fragmentation. The key to establishing a comprehensive AD diagnostic and therapeutic system lies in the effective implementation of early screening. Only by ensuring high-quality advancement of front-end early screening, maximizing the identification of patients in the early stages of AD, and subsequently implementing optimal early intervention measures, can the pressures and challenges faced in the back-end treatment and rehabilitation phases be alleviated.
The following is an excerpt from the report:
Public Awareness and Early Screening Technologies Both Require Improvement
According to clinical feedback, the current challenges in early screening for Alzheimer’s disease (AD) are mainly reflected in insufficient public awareness of the disease, limitations of early screening technologies, a scarcity of specialized institutions, and poor patient compliance.
Public awareness of Alzheimer’s disease (AD) remains severely inadequate, posing significant challenges for market education.This is manifested in the following aspects: First, public education and awareness are insufficient; many people lack an accurate understanding of Alzheimer’s disease (AD) and confuse it with other neurodegenerative diseases that cause cognitive decline. Second, most potential patients and their families fail to fully recognize the severe burden and distress caused by AD, resulting in little willingness or initiative to seek medical help. Third, there is a widespread tendency to ignore early signs of memory loss in the elderly, thereby missing opportunities for early intervention. Fourth, due to significant stigma associated with the disease, some patients are reluctant to disclose their condition to family members and physicians after experiencing cognitive decline, leading to delays in diagnosis and treatment.
There is a shortage of specialized institutions and qualified professionals.Alzheimer’s disease (AD) is a neurological disorder. Compared with common conditions seen in neurology outpatient clinics, such as stroke and peripheral nerve injury, AD has a relatively low consultation rate. Coupled with its insidious onset and the lack of medications capable of reversing the disease after diagnosis, specialized institutions, platforms, and physicians dedicated to the treatment and rehabilitation of AD constitute a very small niche within the field of neurology in China. The annual volume of diagnosed and treated cases is very low, and the rates of early misdiagnosis and missed diagnosis are relatively high. As a result, a large number of individuals with potential or confirmed AD do not receive professional diagnosis, treatment, and rehabilitation guidance.
Poor patient compliance.Alzheimer’s disease (AD) typically onsets in individuals aged 65 and older. Given that AD pathogenesis is multifactorial, early intervention requires a prolonged duration with delayed observable efficacy, leading to poor adherence and limited engagement from both patients and their families during the early intervention phase.
Limitations of Early Screening Technologies.Currently, the AD detection techniques used in clinical practice are either invasive, such as cerebrospinal fluid testing, or costly, such as PET imaging, or unable to accurately screen asymptomatic patients, such as neuropsychological assessments, leading to poor compliance with early screening.
According to research, AD early screening technologies suitable for large-scale application shouldBiomarker Panels, Sensitivity, Standardization, Accessibility, Early Screening, ConvenienceEvaluation Across Six Dimensions. First, early screening products for Alzheimer’s disease (AD) should ideally enable multiplex testing, covering established core biomarkers such as Aβ40, Aβ42, and p-tau181. Second, AD early screening products must demonstrate high sensitivity. Third, the products need to be standardized to ensure stability, accuracy, and reliability. Fourth, reagents and equipment should not be excessively costly; otherwise, they would fail to comply with existing pricing standards for medical services. Fifth, ultra-early detection capability is required to identify asymptomatic patients as soon as possible. Sixth, testing convenience is essential: since AD patients are predominantly elderly individuals with compromised physical function, potentially accompanied by mobility limitations and declines in vision and hearing, the testing process must ensure both convenience and comfort. Unfortunately, no current early screening technology can simultaneously meet all these clinical expectations.
Currently, AD detection technologies can be categorized into four types: neuropsychological assessment, neuroimaging techniques, cerebrospinal fluid (CSF) testing, and blood-based testing.
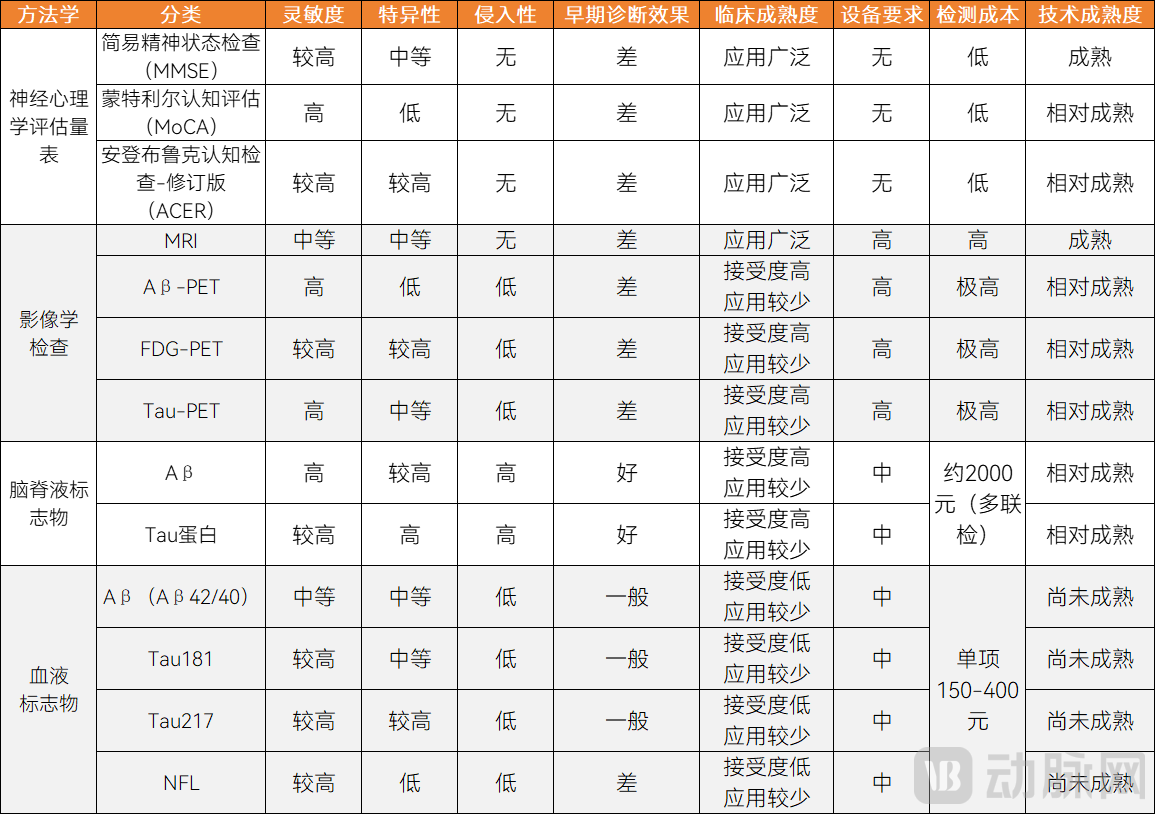
Classification and Characteristics of AD Detection Technologies
Neuropsychological assessment techniques are relatively mature, but it is difficult to detect early-stage asymptomatic patients.
Early screening technologies for Alzheimer’s disease (AD) must be capable of identifying asymptomatic individuals in the early stages, while the detection methods should offer substantial cost-effectiveness and be scalable for large-scale implementation. In the past, neuropsychological assessments were widely used as an AD screening tool due to their low cost and technological maturity.
Neuropsychological assessments also have multiple limitations, making early screening for Alzheimer's disease (AD) quite difficult when relying solely on these assessments.First, the design of assessment scales is complex, and most widely adopted scales originate from Western countries. Their wording and concepts pose comprehension difficulties for the elderly population, particularly those with lower levels of education. Second, neuropsychological assessments are primarily designed for patients who already exhibit cognitive impairment, lacking sufficient sensitivity to detect early-stage patients who are asymptomatic or present with very mild symptoms.
PET imaging is the “gold standard” for diagnosis, but its high cost hinders widespread adoption.
PET has shifted medical imaging from “visible detection” to “early detection,” offering new possibilities for the precise early diagnosis of Alzheimer’s disease (AD). The PET techniques commonly used in AD diagnosis include amyloid-beta (Aβ)-targeted PET (Aβ-PET), microtubule-associated protein tau-targeted PET (tau-PET), and glucose metabolism-targeted PET (FDG-PET). In brief, Aβ-PET imaging offers the most significant advantage in the precise early diagnosis of AD, tau-PET imaging is used to assess AD progression, and FDG-PET imaging is employed to evaluate neuronal injury.
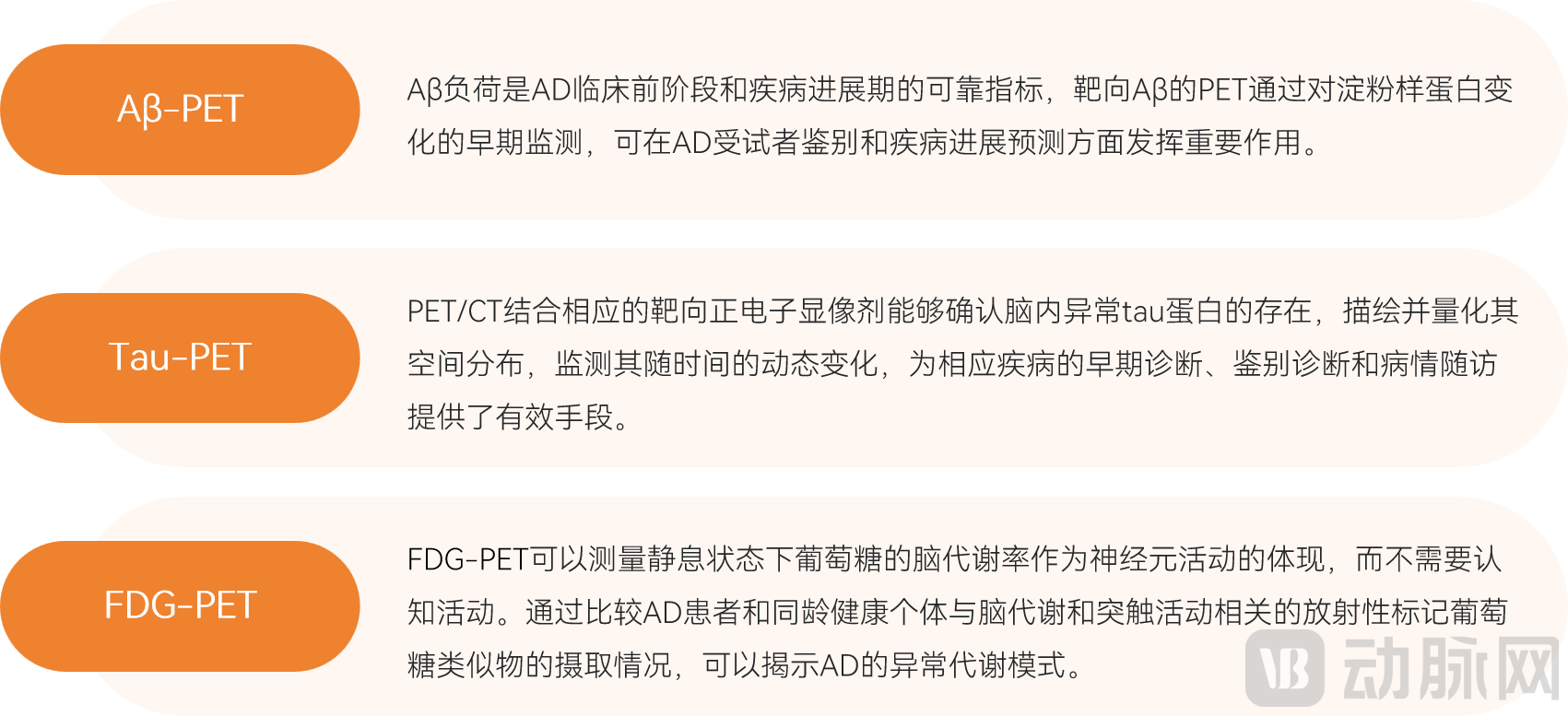
Applications of Various PET Techniques in the Diagnosis of Alzheimer's Disease
Aβ-PET facilitates the early diagnosis, differential diagnosis, and follow-up treatment of Alzheimer’s disease (AD), representing one of the most commercially mature PET imaging technologies.In 2012,18F-Florbetapir, approved by the FDA, is currently the most widely used Aβ imaging agent. In 2023, Sinotau Pharmaceuticals’ fluorine-[18F] Beta-benzene Injection has been approved by the NMPA, becoming the first Aβ imaging agent approved in China. In addition, Andike's fluorine [18F] Lobepine Injection has been submitted for marketing approval.
Tau-PET is used to assess disease severity and helps predict the progression of MCI. The main imaging agents for tau-PET include18F-AV1451 (T807)、18F-THK5351、18F-THK5317 and11C-PBB3, etc., among which18F-AV1451 (T807) is an FDA-approved imaging agent.
However, PET imaging has limitations such as poor spatial resolution, high cost, limited availability of equipment, out-of-pocket payment requirements for patients in most regions, and exposure to radiation. Due to these constraints, PET imaging fails to meet the affordability and accessibility needs for early screening of Alzheimer's disease (AD).
CSF Testing: Highly invasive, poor patient compliance; only Roche is approved in China
As cerebrospinal fluid (CSF) is in direct contact with the brain’s extracellular space and typically reflects pathological changes in the brain, it serves as an optimal source for pathological biomarkers, offering high specificity and sensitivity.
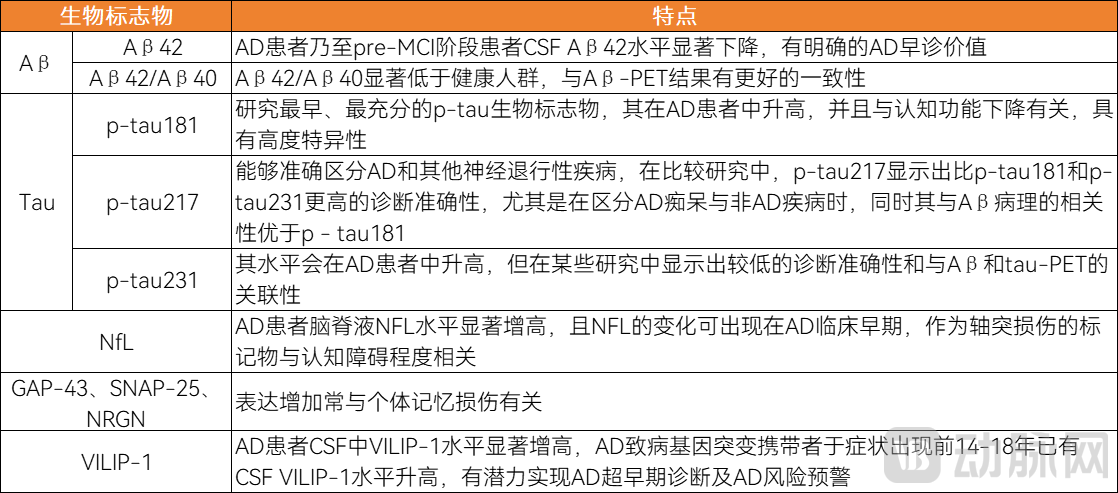
AD Cerebrospinal Fluid Biomarkers
In terms of diagnostic technologies, cerebrospinal fluid (CSF) testing for Alzheimer’s disease (AD) can employ enzyme-linked immunosorbent assay (ELISA), liquid chromatography-tandem mass spectrometry (LC-MS/MS), multiple reaction monitoring (MRM), flow cytometry, and single-molecule immunoassays.
The FDA has approved cerebrospinal fluid (CSF) diagnostic kits for Alzheimer’s disease from two companies, both utilizing chemiluminescence assays.

Progress of Overseas Companies and Products in AD Cerebrospinal Fluid Testing
In China, only Roche’s cerebrospinal fluid test for Alzheimer’s disease has been approved in Hainan.In 2024, Roche Diagnostics’ cerebrospinal fluid (CSF) assay panel for Alzheimer’s disease (AD) was officially approved by the Hainan Provincial Medical Products Administration as an imported medical device urgently needed for clinical use. By quantitatively measuring the concentrations of Aβ(1-42) (Aβ-42), p-tau, and t-tau in human CSF, the product is used to assess cognitive impairment caused by AD, demonstrating up to 90% concordance with PET imaging. Currently, these products have been formally implemented at Ruijin Hospital Hainan Hospital, where real-world studies have been initiated.
The limitation of cerebrospinal fluid testing is that sample collection requires lumbar puncture, which poses significant risks for the elderly population and precludes its use in large-scale screening.Furthermore, the high cost is a major barrier hindering the clinical application of cerebrospinal fluid (CSF) testing. Currently, CSF testing in China is conducted exclusively through third-party medical laboratories, which predominantly use imported products. In the future, with the market entry of domestically produced CSF testing products, there will be significant room for price reduction.
Blood tests offer distinct advantages, as they can detect early-stage patients and be implemented on a large scale. As an economical, convenient, minimally invasive, and highly accessible testing technology that has emerged in recent years, blood testing is well-suited for large-scale early screening of Alzheimer’s disease (AD), holding significant importance for early screening, early diagnosis, and follow-up monitoring of AD. Currently, discussions surrounding blood-based testing for AD primarily focus on advances in biomarkers, selection of technical pathways, and progress in product commercialization.
p-tau217 May Be the Optimal Blood-Based Biomarker for Alzheimer’s Disease
p-tau217 demonstrates superior diagnostic performance and has gained significant attention in recent years. Compared with other phosphorylated tau isoforms, plasma p-tau217 exhibits greater magnitude of change in patients with Alzheimer’s disease (AD), with levels increasing during the preclinical stage of AD. This enables earlier identification of AD pathological changes, offering diagnostic accuracy comparable to cerebrospinal fluid (CSF) testing. For Aβ pathology, plasma p-tau217 accurately identifies individuals who are Aβ-PET positive. For tau pathology, it accurately identifies those who are tau-PET positive or have elevated CSF p-tau181 levels. In a prospective cohort study, p-tau217 showed a stronger correlation with Aβ positivity than plasma p-tau181, p-tau231, N-terminal tau, GFAP, or NfL.
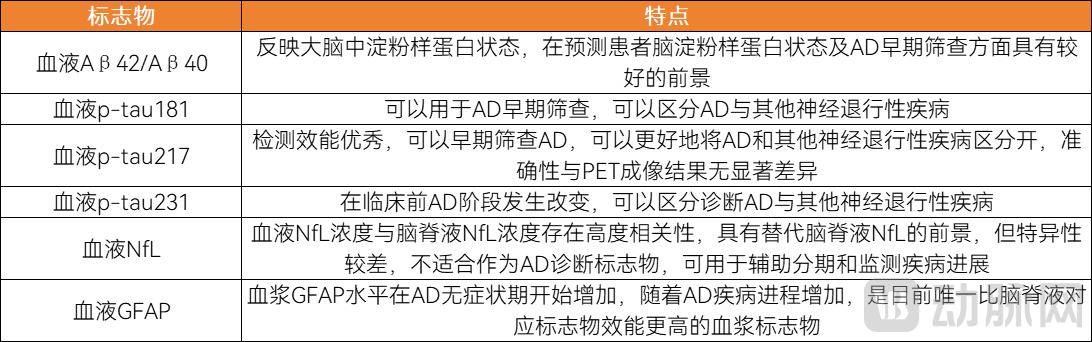
AD Blood Biomarkers
Single-Molecule Immunoassay Enables Precise Detection of Low-Abundance Biomarkers, Highly Aligned with the Needs for Early Screening of Alzheimer’s Disease
Changes in blood biomarker concentrations may be influenced by the permeability of the blood-brain barrier and alterations in systemic physiological status. Furthermore, as blood biomarker levels are lower than those in cerebrospinal fluid, their detection imposes more stringent requirements on analytical techniques.
Current blood-based testing technologies for Alzheimer’s disease (AD) include chemiluminescence, single-molecule immunoassay, mass spectrometry, and flow fluorescence. Each of these technologies has its own advantages and limitations in terms of cost-effectiveness, quantitative accuracy, and sensitivity for early screening. According to research, when applied to early AD screening, single-molecule immunoassay effectively meets the needs of early detection due to its ultra-high sensitivity.
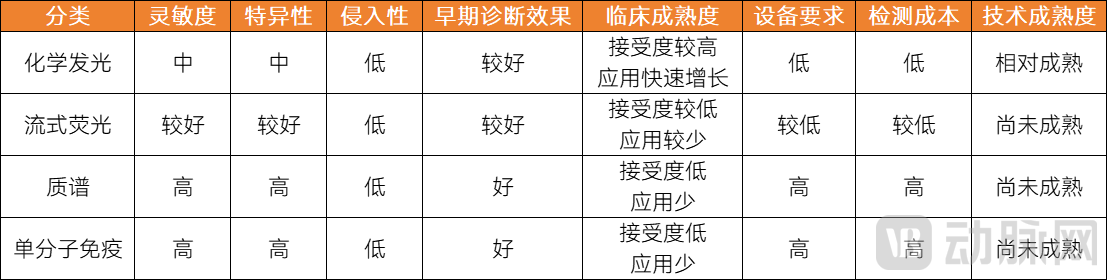
Comparison of Blood-Based Testing Technologies for Alzheimer’s Disease
Chemiluminescence has a leading advantage in terms of cost and installed base, but its sensitivity does not meet the requirements for early screening.Chemiluminescence technology is mature, with a high degree of automation, widespread equipment adoption, rapid testing times, and numerous approved products on the market. With transparent pricing and picogram-level detection sensitivity, it meets the requirements for clinical diagnosis. However, the sensitivity of chemiluminescence currently falls short of the demands for early screening. Chemiluminescence can only detect biomarkers present at relatively high concentrations in the blood, whereas biomarker levels are extremely low in asymptomatic patients during the early stages, making it unsuitable for early screening. Therefore, leveraging its installed base and cost advantages, chemiluminescence is better suited for outpatient settings to provide clinical diagnoses for symptomatic patients.
Moreover, chemiluminescence performs well in detecting biomarkers with relatively high concentrations in blood, such as Aβ40, Aβ42, t-tau, and NfL. However, its current sensitivity is insufficient for the accurate detection of low-abundance biomarkers like p-tau181 and p-tau217; achieving this will require the development of more sensitive antibodies.
Flow cytometry-based fluorescence technology offers the unique advantage of multiplex detection; however, current early screening for Alzheimer’s disease (AD) does not require multiplex testing.Currently, only a few blood-based early screening biomarkers for Alzheimer’s disease (AD) are widely recognized, such as p-tau217, making multiplex testing unnecessary. Moreover, the analytical performance of flow fluorescence immunoassay is comparable to that of chemiluminescence immunoassay, rendering it equally unsuitable for screening asymptomatic individuals in the early stages. In addition, flow fluorescence immunoassay suffers from drawbacks including lower levels of automation and longer reaction times.
Mass spectrometry demonstrates the best performance in precise quantification, but its clinical application is limited due to high costs and low instrument installation rates.The concentration of Alzheimer’s disease (AD) biomarkers in blood is extremely low. In addition to AD pathological biomarkers, peripheral blood contains interfering substances derived from other organs, such as liver-derived amyloid-beta (Aβ). Differentiating AD pathological biomarkers from other markers requires detection technologies capable of precise quantification. From a quantitative perspective, mass spectrometry is the most ideal method for blood-based AD testing, offering the highest accuracy and reducing the risks of misdiagnosis and missed diagnosis. In contrast, immunoassay techniques rely on antigen-antibody binding for detection; antibodies are susceptible to interference, resulting in poorer quantitative performance. However, mass spectrometry involves complex workflows, has a very low level of automation, and requires expensive instrumentation, keeping its clinical application in the early stages.
Single-molecule immunoassay technology demonstrates excellent sensitivity and specificity, meeting the needs for ultra-early screening.Biomarker levels in the blood of patients with early-stage Alzheimer’s disease (AD) are extremely low, making single-molecule immunoassays suitable for low-abundance detection. Single-molecule immunoassay is an ultra-sensitive ELISA technology, represented by Simoa. Simoa utilizes antibody-coated beads, fluorescently labeled detection antibodies, and digital readouts, achieving a sensitivity more than 1,000 times greater than that of conventional ELISA. With a limit of detection reaching the fg/mL level, it enables effective detection and quantification of ultra-low-abundance proteins, thereby ensuring the accuracy and reliability of early AD screening.
A comprehensive comparison of various technologies reveals that single-molecule immunoassays offer ultra-high sensitivity, enabling the detection of Alzheimer’s disease (AD)-related pathological biomarkers at very early stages and identifying asymptomatic individuals in the early phase. This confers an irreplaceable advantage for early AD screening.As simple, stable, and lower-cost single-molecule immunoassay technologies developed by domestic companies enter the market, equipment and reagent costs will further decrease, and the market share of single-molecule immunoassays in the early screening market for Alzheimer’s disease (AD) will rise rapidly. It is advisable to closely monitor the progress of single-molecule immunoassay companies in the AD early-screening segment.
In the single-molecule immunoassay market, Guangyu Shengwu adopts “"Single-Molecule Immunoassay with Chemiluminescence"strategy, has successfully developed a solution that combines bothHigh-Sensitivity, High-Automation, Low-Cost Single-Molecule Immunoassay Analyzer。
Traditional single-molecule immunoassay devices are characterized by high costs and prolonged detection times, posing significant challenges to instrument deployment and hindering the rapid clinical adoption of single-molecule immunoassays. To address these issues, Guangyu Biology has entered into a strategic partnership with Yingkai Technology. Leveraging its proprietary single-molecule immunofluorescence optical detection module and integrating it with Yingkai Technology’s fully automated chemiluminescence platform, Guangyu Biology has successfully developed a single-molecule immunoassay analyzer that combines high sensitivity, high automation, and low cost.
Currently, both parties are expanding the scope of their collaboration and continuing to develop integrated single-molecule luminescence analyzers. These integrated systems can perform specialized single-molecule immunoassays as well as routine chemiluminescence immunoassays. Leveraging this collaborative model, Guangyu Biology has effectively reduced instrument costs while accelerating market penetration through established chemiluminescence distribution channels, thereby opening new avenues for the clinical promotion and application of single-molecule immunoassay technology.
Leveraging its domestically produced single-molecule immunoassay platform, Guangyu Shengwu is collaborating with leading domestic hospitals in neurology to carry out1,500-Patient Exclusive Large-Scale Cohort Study in China。
No AD blood tests have been approved in the United States, while approved products in China are predominantly based on chemiluminescence assays.
Overseas, the FDA has not yet approved any blood-based diagnostic products for Alzheimer’s disease (AD) for market entry; however, products from Roche, Quanterix, and Fujirebio have received FDA Breakthrough Device Designation. In September 2024, Fujirebio announced that it had submitted a marketing application to the FDA for its Lumipulse® G pTau 217/β-Amyloid 1-42 assay kit, positioning it as a potential candidate to become the first FDA-approved blood-based diagnostic product for AD.
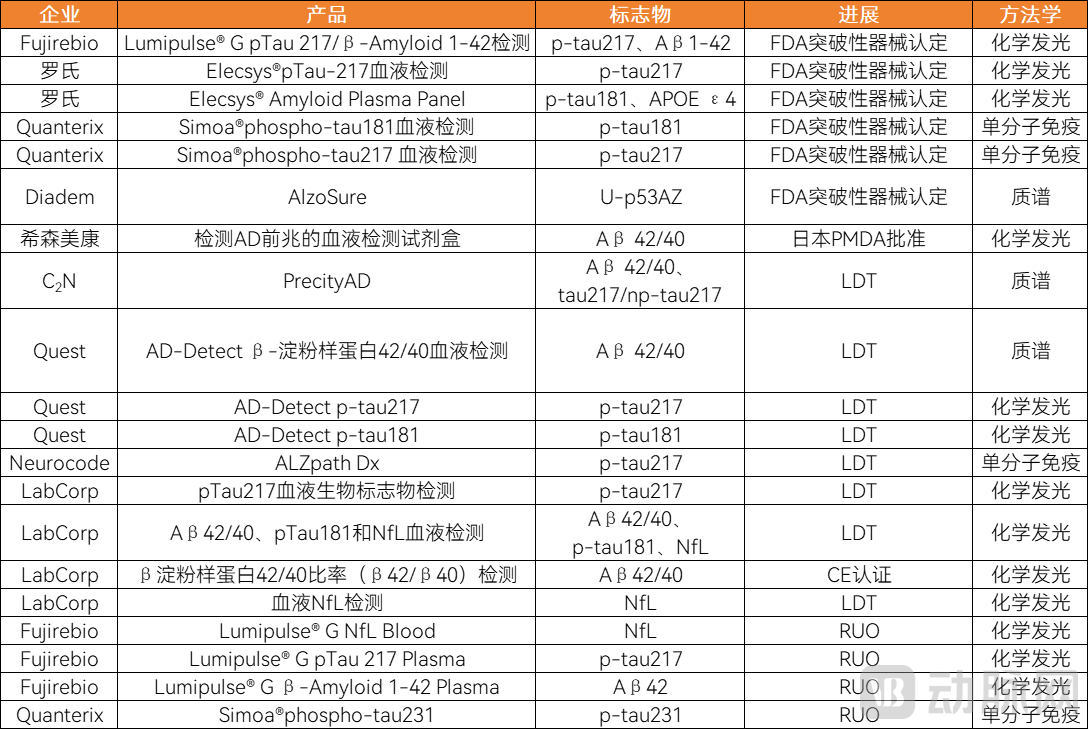
Global Companies’ Strategic Layout in the AD Blood Test Market
The number of AD blood test products approved in China far exceeds that approved by the FDA.According to VBInsight statistics, as of December 31, 2024, there were a total of 47 AD blood test kits approved by the NMPA in China.
Among the approved blood test kits for Alzheimer's disease (AD), those utilizing chemiluminescence technology are the most prevalent, with 24 products. Five kits employ enzyme-linked immunosorbent assay (ELISA) technology, while two each utilize single-molecule immunoassay and flow fluorescence technologies. Currently, no blood test kits based on mass spectrometry have been approved.
Chemiluminescence is one of the largest and most mature sub-segments in the in vitro diagnostics (IVD) market. Due to its convenient and rapid operation, it has the highest number of approved assay kits. Therefore, future attention should be focused on the performance of chemiluminescence in Alzheimer’s disease (AD) detection. Single-molecule immunoassay is an emerging technology with unique technical advantages. Although the number of currently approved products is limited, it holds considerable growth potential in the future.
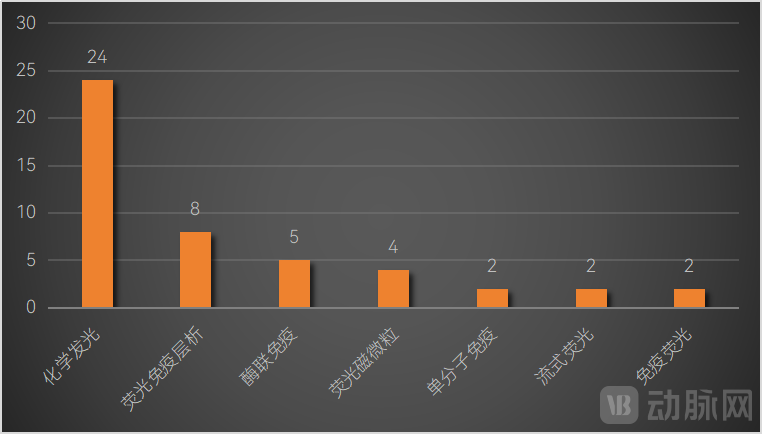
Technologies Used in Approved Blood Test Kits for Alzheimer’s Disease
The biomarkers detected by the approved kits are primarily core biomarkers of Alzheimer’s disease (AD), including plasma Aβ42/Aβ40, p-tau181, p-tau217, and p-tau231.
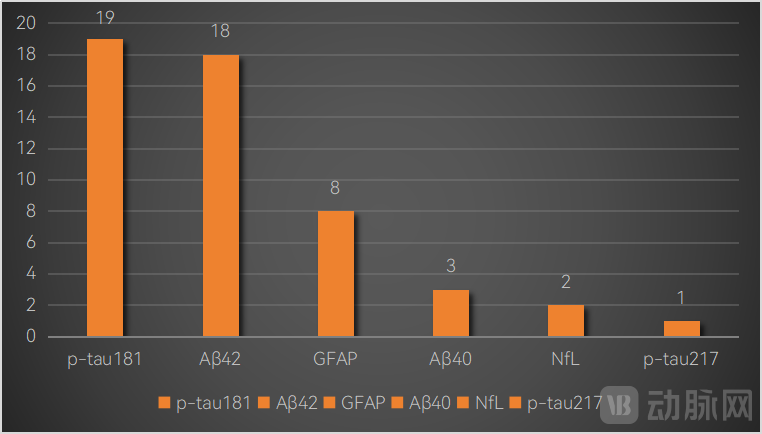
Biomarkers Involved in Approved Blood Test Kits for Alzheimer’s Disease
In the future, for blood tests for AD to be widely applied in clinical practice,The issue of positive expression rate needs to be addressed first.. The positive expression rate is correlated with accuracy and specificity. According to current research findings, the positive detection rate of plasma p-tau217 is largely consistent with that of cerebrospinal fluid testing, ranging from approximately 89% to 98%. However, its specificity remains to be further evaluated. Since the progression and clinical manifestations of Alzheimer’s disease (AD) are influenced by a variety of congenital and acquired factors, the specificity and uniqueness of blood-based test results still require further improvement and enhancement.
Secondly, the issue of standardizing blood tests for Alzheimer's disease (AD) needs to be addressed.According to clinical feedback, there are significant discrepancies in the test results of blood-based diagnostic kits for Alzheimer’s disease (AD) from different manufacturers, which has directly hindered the widespread clinical adoption of AD blood testing. It is reported that domestic manufacturers in China currently utilize diverse technical platforms, resulting in vastly different reference ranges. Consequently, test results across different platforms are not mutually recognized, and each manufacturer has independently established its own reference ranges and traceability systems. It is hoped that, in the future, multi-center studies will be accelerated in China to standardize the detection process of biomarkers. By standardizing pre-analytical factors, unifying testing methods and tools, and introducing automated analysis technologies, a unified standard for positive reference values can be established, thereby improving the accuracy of blood-based biomarkers in distinguishing between healthy individuals and patients.
The application scenarios for early screening of Alzheimer's disease (AD) are diverse, including in-hospital settings, health examination centers, public welfare programs, insurance sectors, and home-based testing.

Characteristics of Different Application Scenarios for Early Screening of Alzheimer's Disease
In-hospitalThis represents the most stringent entry barrier scenario for early screening of Alzheimer’s disease (AD). In this setting, AD blood-based diagnostic products follow the traditional pathway for in-hospital sales of in vitro diagnostic (IVD) devices, requiring completion of regulatory registration, large-scale clinical trials, and pricing approval, among other steps. The in-hospital setting imposes the highest requirements on products; if the performance of AD blood tests fails to surpass that of conventional diagnostics, they risk being excluded from hospital formularies. Therefore, manufacturers of AD blood-based diagnostics must place significant emphasis on clinical evidence by conducting large-scale prospective clinical studies to enhance product robustness and clinical utility. Concurrently, sustained academic promotion is essential to gain acceptance among clinicians.
InHealth Checkup ScenariosUsers tend to prefer non-invasive and convenient testing methods, and blood tests align well with this preference. Furthermore, cost control is a key consideration for health examination centers; compared to cerebrospinal fluid testing and PET imaging, blood tests are more cost-effective and easier to incorporate into routine health check-up packages. Additionally, since the core philosophy of health examination centers focuses on prevention and early screening, which aligns with the positioning of Alzheimer’s disease (AD) blood test products, these centers demonstrate greater acceptance of AD blood testing than other settings and are willing to rapidly introduce and promote this technology.
Livelihood ProjectsAs a critical application scenario for early Alzheimer’s disease (AD) screening, this sector is demonstrating significant growth potential, driven by strong government support. Through government-funded procurement, companies can rapidly acquire sufficiently large sample sizes and collect rich clinical data. This not only helps validate product feasibility and efficacy but also facilitates product promotion, enhances brand awareness, and further expands penetration into primary care markets. Currently, local governments across various regions are investing in AD early-screening initiatives to varying degrees, with an increasing number of public welfare projects emerging nationwide.
InsuranceAt this level, insurance coverage for Alzheimer’s disease (AD) is gaining increasing attention from insurers. AD-specific insurance products are being launched successively, and the integration of early AD screening services into insurance offerings is becoming a powerful tool for customer acquisition and marketing, claims reduction, and differentiated competition.
Home CareScenario: Although latent demand is strong, the home-based early screening scenario for Alzheimer’s disease (AD) remains immature, facing multiple challenges including the lack of point-of-care testing (POCT) products for blood tests, low willingness to pay, trust issues, and high customer acquisition costs.
Overall, blood-based early screening products for Alzheimer’s disease (AD) are still in the early stages of application across various scenarios. Only a few companies have initiated market exploration, resulting in low market concentration. It is anticipated that, in the future, products tailored to the specific needs of different settings—such as hospitals, health checkup centers, public welfare programs, insurance schemes, and home care—will pioneer successful commercialization pathways.
The user base for early Alzheimer’s disease (AD) screening is highly fragmented. In the short term, companies should leverage their product features and channel advantages to implement differentiated strategies. Hospital-based settings and health check-up scenarios are expected to be the key focus areas for AD early-screening enterprises in the near future. On one hand, hospital settings can be used to validate the clinical value of products, facilitating academic promotion and market education; on the other hand, health check-up scenarios can generate cash flow, providing financial support for product R&D and marketing efforts. As market awareness matures and willingness to pay increases, companies can gradually expand into additional scenarios.
In the long term, deploying across multiple application scenarios is the prevailing trend. Covering diverse commercial channels can meet screening needs in various settings, thereby enhancing the accessibility and convenience of screening services. This requires enterprises to continuously strengthen their competitiveness in product innovation, service quality, pricing strategies, and channel management.
The above is an excerpt from the white paper. The overall framework of the report is as follows:
Chapter 1: Aging Population, New Drug Approvals, and Policy Guidance Drive Strong Demand for Early Alzheimer’s Disease Screening
1.1 The pathogenesis of AD remains unclear; as staging becomes increasingly refined, early screening has become a focal point
1.2 China Has a Large Population of AD Patients, a Heavy Disease Burden, and an Urgent Need for Early Screening
1.3 Innovative drugs primarily target patients in the early stages, necessitating the earliest possible diagnosis of Alzheimer’s disease (AD)
1.4 Policy Orientation: Early Screening for AD Has Become a Core Issue in the Healthcare Sector
Chapter 2: Blood Testing May Be the Most Suitable Technology for Large-Scale Early Screening of Alzheimer’s Disease
2.1 Public Awareness and Early Screening Technologies Both Need Improvement
2.2 Neuropsychological assessment techniques are relatively mature, but it is difficult to detect early-stage asymptomatic patients
2.3 PET Imaging Is the Diagnostic “Gold Standard,” but Its High Cost Hinders Widespread Adoption
2.4 Cerebrospinal Fluid Testing: Highly invasive, poor patient compliance; only Roche has received approval in China
2.5 Blood tests offer distinct advantages, as they can detect early-stage patients and be implemented on a large scale
Chapter 3: Commercialization in Its Early Stages, with Blood Tests Poised for Rapid Growth in Health Checkup Settings
3.1 All scenarios are in the early stages of application, with commercial pathways not yet established
3.2 Short-term focus on in-hospital and health checkup scenarios, with multi-scenario deployment as a long-term trend
Chapter 4: Industry Reshaping Underway, with Ecosystem Building and Industry Standardization Issues Yet to Be Resolved
4.1 Niche and Fragmented Industrial Ecosystem: Need to Establish a Complete Industrial Closed Loop
4.2 Standardization of AD Blood Tests Is Challenging but Imperative
4.3 The payment system for early screening of Alzheimer's disease (AD) is inadequate, with some items lacking fee schedules and not being covered by medical insurance
Please scan the QR code to add the assistant and obtain the full report. If you have already added the assistant, please proactively reach out.
