Geron's First-in-Class Telomerase Inhibitor Rytelo (Imetelstat) Approved by FDA After Nearly 40 Years of Research, Projected to Reach $2.1 Billion in Sales

Geron
Cancer Treatment Product Developer
After nearly 40 years of persistent dedication, there is finally an echo.
On June 6, 2024, Geron Corporation (Nasdaq: GERN, hereinafter referred to as “Geron”) announced that imetelstat (brand name: Rytelo) had received FDA approval for the treatment of adult patients with lower-risk myelodysplastic syndromes (LR-MDS) who have transfusion-dependent anemia requiring four or more units of red blood cells within an 8-week period, and who are either unresponsive to, refractory to, or ineligible for erythropoiesis-stimulating agents (ESAs).
Low-risk myelodysplastic syndromes (LR-MDS) is a type of blood cancer. As the disease progresses, patients require increasingly intensive management of key symptoms such as anemia and fatigue, which often leads to dependence on red blood cell transfusions, thereby reducing quality of life and shortening survival. For patients who fail erythropoiesis-stimulating agent (ESA) therapy, current treatment options are limited to specific subpopulations; thus, there is an unmet clinical need for therapies that can provide sustained, long-term transfusion independence.
Rytelo is a “first-in-class” telomerase inhibitor that Geron has diligently developed over 33 years. It is also the first telomerase inhibitor approved by the U.S. FDA. Since the discovery of telomerase in 1984, the industry has finally welcomed its first telomerase-targeted therapy after nearly 40 years of waiting. Rytelo was listed by the industry media Evaluate as one of the top 10 potential blockbuster therapies of 2024.
“Life Clock” Telomerase
Strictly speaking, any mention of telomerase requires casting our minds back to the 1930s—the period when telomeres were first discovered. At that time, American genetics pioneers and two Nobel laureates, Barbara McClintock and Herman Muller, independently observed in their experiments that the chromosome ends in maize and Drosophila melanogaster were remarkably stable and did not undergo fusion following breakage. Like many scientists of the era who possessed a strong classical education, Muller coined the term “Telomere” for this distinctive structure, deriving it from the Greek words telos (end) and meros (part).
In 1961, a young scholar accidentally discovered that cells cultured in vitro could only undergo a limited number of divisions (50 ± 10 times), proposing the assertion that "cells are not immortal." This finding overturned the then-prevailing academic consensus on "cellular immortality," thereby accelerating scientific exploration into the microscopic realm of cells. A decade later, American researchers raised the issue of asymmetric DNA replication, predicting that each cell division would result in the loss of chromosomal fragments at the ends of one strand, thus introducing the concept of the "end-replication problem."
In 1984, following studies on unicellular organisms, molecular biologists discovered telomerase, an enzyme capable of maintaining telomere length, and elucidated its distinctive role in the human body: with the exception of human germ cells and certain somatic cells, telomerase is largely inactive in most other cell types; however, it maintains telomere length in cancer cells, thereby enabling their unlimited proliferation.
In 1990, scientists Calvin Harley, Futcher, and Greider jointly discovered that during in vitro culture of human fibroblasts, telomeres shorten with each cell division, and the accumulation of critically short telomeres ultimately triggers the “Hayflick limit.”
Simply put, the older a cell is, the shorter its telomeres; the younger a cell is, the longer its telomeres. Telomeres are associated with cellular aging. In senescent cells, some telomeres have lost a significant portion of their repetitive sequences. When telomere function is impaired, cellular senescence occurs; and when telomeres shorten to a critical length, senescence accelerates, bringing the cell closer to death.
Secondly, normal cells have relatively short telomeres. Cell division causes telomeres to shorten; with each division, they become slightly shorter, akin to the wear and tear on an iron rod. When only a residual fragment remains, the cell approaches senescence. With each cell division, approximately 30–200 base pairs (bp) of telomeric DNA are lost.
An enzyme capable of synthesizing telomeres is present in cells. Telomere replication cannot be catalyzed by classical DNA polymerases; instead, it is carried out by a specialized reverse transcriptase known as telomerase. Telomerase is undetectable in normal human somatic cells. Telomerase activity is also not detected in cells from certain benign lesions or in fibroblasts cultured in vitro. However, this enzyme tests positive in germ cells, testes, ovaries, placenta, and fetal cells.
Since then, telomeres have joined the ranks of the “cellular life clock,” a metric for measuring lifespan and an unavoidable topic in discussions on aging.
Following the elucidation of telomerase composition, the world’s first telomerase-edited mouse model was developed in 1997 under the leadership of renowned Spanish scholar Maria A. Blasco, and it has since been widely utilized in numerous studies.
On October 5, 2009, the Nobel Committee at the Royal Swedish Academy of Sciences announced that the 2009 Nobel Prize in Physiology or Medicine had been awarded to Elizabeth H. Blackburn, Carol W. Greider, and Jack W. Szostak for their discovery of “how telomeres and the enzyme telomerase protect chromosomes.”
Specifically, Blackburn and Szostak discovered that a special DNA sequence in telomeres prevents chromosomes from degradation, while Greider and Blackburn identified the molecule that aids telomere synthesis—telomerase. Their findings elucidated the role of telomerase in stabilizing the length and structure of telomeres, thereby protecting chromosomes. Meanwhile, telomeres and telomerase are not only closely related to chromosomal characteristics and stability but also involved in cellular aging and damage, as well as cancer development.
Multiple Indications
In 1990, Geron was founded in Delaware by Michael West, a pioneer in stem cell, cellular senescence, and telomerase research, and Alex Barkas, a prominent venture capitalist and partner at Kleiner Perkins Caufield & Byers at the time. The company completed its Series A, B, C, and D funding rounds in 1992, 1993, 1994, and 1995, respectively.
In 1996, Geron successfully went public on the NASDAQ. The three laureates of the 2009 Nobel Prize in Physiology or Medicine, along with renowned American biologist Leonard Hayflick—who proposed the “Hayflick limit”—served as the company’s scientific advisors at that time.
Subsequently, like typical companies focused on translating scientific research into commercial applications, Geron also embarked on a path of mergers and acquisitions. In 1999, Geron acquired Roslin Bio-Med and its nuclear transfer technology; in 2002, the company acquired phosphoramidite chemistry IP assets from Lynx Therapeutics.
In 2003, Geron developed oligonucleotides that bind to the RNA template of telomerase and competitively inhibit its activity. In 2004, it obtained an exclusive license from Argos Therapeutics (formerly Merix Bioscience) to develop dendritic cell-based therapeutic cancer vaccines using telomerase as an antigen. In 2005, Geron enhanced the potency of this telomerase inhibitor through lipid modification, giving rise to Imetelstat. Thus, Imetelstat is essentially a lipid-conjugated 13-mer oligonucleotide.
Imetelstat binds to the RNA template region of human telomerase (hTR), thereby inhibiting telomerase activity and blocking telomere elongation. Studies have shown that telomerase activity and the RNA expression of human telomerase reverse transcriptase (hTERT) are increased in stem cells and progenitor cells in myelodysplastic syndromes and certain malignant tumors. Non-clinical studies have demonstrated that imetelstat treatment reduces telomere length, decreases the proliferation rate of malignant stem and progenitor cells, and induces apoptosis.
For a considerable period thereafter, while exploring imetelstat, Geron also diverted resources to enter the stem cell field. However, in 2011, as the company abandoned its stem cell therapy program for commercial reasons, imetelstat once again drew market attention. This time, however, imetelstat failed in Phase II clinical trials for breast cancer, causing the company’s stock price to plummet by 56%.
Timely loss mitigation became critical. Geron simultaneously halted a trial of imetelstat as a monotherapy in non-small cell lung cancer. The company specifically investigated tumor patients with shorter telomeres (the protective ends of chromosomes) and found that disease progression was slower in the subset of patients (19 in total) receiving imetelstat compared to those receiving placebo. This set the tone for subsequent development of imetelstat: as a monotherapy, it aims to inhibit the enzyme responsible for telomere elongation; by starting with short telomeres, the drug gains a strategic advantage, making it easier to kill tumor cells.
Clinical trials of imetelstat for non-small cell lung cancer, glioma, and other indications have all ended in failure. Geron needs to adjust its strategy in indication selection: to bring the product to market, Geron has decided to shift its R&D focus to hematologic malignancies. More importantly, however, is the need to secure a strong commercial partner.
A Plagued Journey, Rebounding from the Depths
On November 13, 2014, Geron and Janssen Biotech, Inc. entered into a joint research and license agreement to develop and commercialize imetelstat for oncology indications worldwide, including hematologic malignancies and other human therapeutic uses.
On November 13, 2014, Geron and Janssen Pharmaceuticals, a subsidiary of Johnson & Johnson, entered into a global strategic collaboration for imetelstat, with a total potential value of up to $935 million, aimed at jointly advancing its development and commercialization. During the partnership, Phase 2 studies of imetelstat were conducted separately for myelodysplastic syndromes (MDS) and myelofibrosis (MF). However, Janssen’s involvement failed to reverse the clinical outcomes. As the results of both studies did not meet Johnson & Johnson’s expectations, the two parties terminated the collaboration in 2018.
In January 2023, Geron reported positive top-line results from the IMerge pivotal Phase 3 clinical trial, which evaluated the efficacy of imetelstat in patients with transfusion-dependent lower-risk myelodysplastic syndromes (TD LR-MDS). The company noted that the trial met its primary and key secondary endpoints, and the study results were published in *The Lancet* in December 2023.
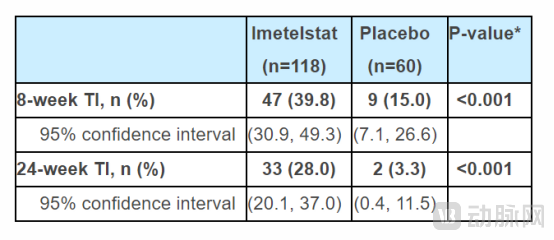
This randomized, double-blind, placebo-controlled clinical trial evaluated the efficacy and safety of imetelstat in patients with lower- and intermediate-risk myelodysplastic syndromes (MDS) who were transfusion-dependent and refractory or intolerant to erythropoiesis-stimulating agents. The results showed that at 8 weeks of treatment, 39.8% of patients in the imetelstat group maintained transfusion independence, compared with 15.0% in the placebo group (Rytelo: 39.8%, 95% CI: 30.9–49.3; placebo: 15.0%, 95% CI: 7.1–26.6; p<0.001). At 24 weeks, 28.0% of patients in the imetelstat group maintained transfusion independence, compared with 3.3% in the placebo group (Rytelo: 28.0%, 95% CI: 20.1–37.0; placebo: 3.3%, 95% CI: 0.4–11.5; p<0.001).
In an exploratory analysis of patients treated with Rytelo who achieved red blood cell transfusion independence (RBC-TI) for ≥8 weeks, the median increase in hemoglobin was 3.6 g/dL in the Rytelo group versus 0.8 g/dL in the placebo group. Clinically meaningful efficacy outcomes were observed across key MDS subgroups, regardless of patients’ ringed sideroblast (RS) status, baseline transfusion burden, or International Prognostic Scoring System (IPSS) risk category.
In the IMerge trial, Rytelo demonstrated a favorable safety profile, with thrombocytopenia and neutropenia observed in patients being generally manageable and of short duration.
Overall, imetelstat demonstrated significantly higher rates of red blood cell transfusion independence (RBC-TI). RBC-TI was durably maintained in patients treated with Rytelo, with median durations of approximately 1 year for 8-week responders and 1.5 years for 24-week responders.
However, this answer has not satisfied all those following the field of telomerase.
Foremost among the concerns, the FDA briefing document raised questions regarding the approvability of imetelstat for the treatment of myelodysplastic syndromes.
First, regarding secondary endpoints, the Phase 3 IMerge clinical trial did not demonstrate any benefit of imetelstat on other secondary endpoints, including complete response, partial response, overall survival, and improvements in erythroid hematologic parameters. The FDA stated that these findings do not support Geron’s claim that the telomerase inhibitor imetelstat can improve the condition.
Secondly, imetelstat still has efficacy limitations. Of particular concern are two cases of elevated liver enzymes that met the laboratory definition of Hy’s Law, indicating a risk of fatal drug-induced liver injury in patients. Furthermore, the time to response and potential toxicity raise additional concerns regarding the market approval of imetelstat.
In a dramatic turn of events, on March 14, 2024, the U.S. Food and Drug Administration (FDA) convened a meeting of the Oncologic Drugs Advisory Committee (ODAC) to review imetelstat based on the results of the Phase 3 IMerge clinical trial. The committee ultimately voted 12–2 in favor of the conclusion that the clinical benefits of imetelstat outweigh its risks. Following the announcement, Geron’s stock price surged by 92% the next day. On June 6 of the same year, RYTELO (imetelstat) received successful approval, 10 days ahead of the previously scheduled PDUFA date. This confirms that the FDA determined the overall benefits of imetelstat to outweigh its risks.

According to the prescribing information, Rytelo for injection is a preservative-free white to off-white or pale yellow lyophilized powder, supplied in single-dose vials of 47 mg and 188 mg. The recommended dosage of Rytelo is 7.1 mg/kg per patient, administered via intravenous infusion over 2 hours every 4 weeks.
According to Visible Alpha estimates, Rytelo’s sales could peak at $2.1 billion by 2035.
Other Possibilities of Telomerase Drugs
In addition to low-risk myelodysplastic syndromes (MDS), Geron is also developing imetelstat for the treatment of other myeloid hematologic malignancies, such as myelofibrosis (MF). Statistics indicate that there are approximately 13,000 MF patients in the United States, with around 3,000 new cases reported annually. Approximately 70% of these patients are classified as intermediate-2 or high risk. For patients who are refractory to or have developed resistance to JAK inhibitors, no drugs have been approved for subsequent therapy, resulting in a significant unmet medical need.
Geron’s Phase 3 IMpactMF clinical trial is evaluating imetelstat for the treatment of patients with intermediate-2 or high-risk myelofibrosis (MF) who have relapsed after or are refractory to JAK inhibitor therapy, referred to as relapsed/refractory MF patients. The study uses overall survival (OS) as its primary endpoint. In August 2024, the trial completed enrollment of approximately 70% of patients. Based on current assumptions regarding patient enrollment and event rates (mortality), Geron anticipates that the interim analysis of OS in the IMpactMF study may be conducted in early 2026, with the final analysis potentially taking place in early 2027.
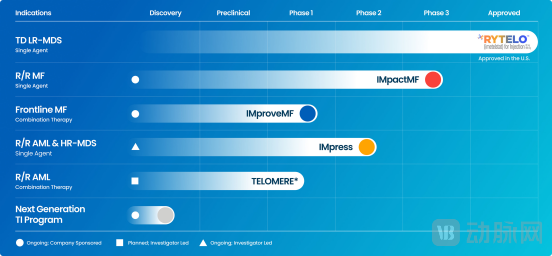
Geron's Pipeline
Globally, in addition to Rytelo, multiple other investigational drugs targeting telomerase are in preclinical and clinical development, each addressing different indications.

Global Telomerase R&D Pipeline, Incomplete Statistics by VCBeat
Among them, Ultimovacs ASA (hereinafter referred to as “Ultimovacs”), which has made the fastest progress, announced the top-line results of its FOCUS Phase II clinical trial (NCT05075122) evaluating UV1 in patients with head and neck squamous cell carcinoma (HNSCC) on August 6, 2024. However, the data showed that the study failed to meet its primary and secondary endpoints.
This may further underscore the significant importance of Rytelo’s market launch.
“For patients with lower-risk myelodysplastic syndromes (MDS) accompanied by anemia who are transfusion-dependent, treatment options are limited, and existing therapies are often used in rotation. The approval of imetelstat may change our practice,” said Dr. Rami Komrokji, a co-investigator at Moffitt Cancer Center, in Geron’s approval announcement. “Imetelstat provides benefits regardless of ring sideroblast status or high transfusion burden, including sustained and durable transfusion independence (TI) and increased hemoglobin levels, with a manageable safety profile. The treatment goal for patients with this condition is to achieve transfusion independence, which was unattainable for many patients prior to the approval of imetelstat.”
More importantly, after a 40-year wait, the industry has finally welcomed the first telomerase-targeted therapy, and the pioneer can pave an entirely new path for many followers.