With Twice-Yearly, Near-100% Effective HIV Prevention Drug Lenacapavir Approved in China, Is an HIV Vaccine Still Needed?
On January 2, Gilead’s Class 5.1 new drugs (already marketed overseas), lenacapavir tablets and lenacapavir injection, received marketing approval from the NMPA and are poised to enter the Chinese market.Lenacapavir is an HIV-1 capsid inhibitor that primarily suppresses HIV-1 replication by interfering with multiple critical steps in the viral life cycle. It has previously been approved as a therapeutic agent in the European Union and the United States for use in combination with other antiretroviral drugs to treat adults with multidrug-resistant HIV infection.
As one of Science’s Top 10 Breakthroughs of 2024, lenacapavir has demonstrated exceptional efficacy and long-acting properties in prevention. Key Phase III trial data showed that lenacapavir was 100% effective in preventing HIV (human immunodeficiency virus) infection in women; 99.9% of participants remained HIV-negative, representing a 96% reduction in HIV incidence compared to the background HIV incidence rate (bHIV).
From this perspective, lenacapavir is also an HIV pre-exposure prophylaxis (PrEP) agent. Its striking 100% efficacy rate has significantly improved both the accessibility of PrEP medications for high-risk populations and adherence to dosing regimens.However, in the face of HIV prevention—a major global public health challenge—existing data remind us that relying solely on PrEP is clearly insufficient.
According to WHO data, by the end of 2022, 39 million people worldwide were living with HIV. It is estimated that 0.7% of adults aged 15–49 globally are infected with HIV. The African region remains the most severely affected, with nearly 1 in every 25 adults (3.2%) living with HIV, accounting for more than two-thirds of the global number of people with HIV.
A 2024 commentary published in The Lancet HIV indicated that although long-acting antiretroviral agents and monoclonal antibodies have advanced treatment and prevention strategies, emerging as the optimal interim approach in settings with low coverage and high HIV prevalence, these interventions are not progressing at the pace required to end AIDS by 2030.
Regarding PrEP, even lenacapavir, which has an exceptionally long half-life and requires only twice-yearly administration, still entails lifelong medication. For high-risk populations in African countries with lifelong prevention needs, this goal is difficult to achieve. Moreover, the reliance on payment systems involving NGOs and medical aid would impose a substantial burden on the global economy.From a practical implementation perspective, large-scale high-risk populations continue to face multiple challenges, including poor access to long-term medication, lack of continuity in care, and insufficient adherence. Furthermore, there is currently no evidence indicating that low-to-moderate risk populations and relevant payers are willing to initiate and sustain PrEP measures at the pace required for major public health interventions.
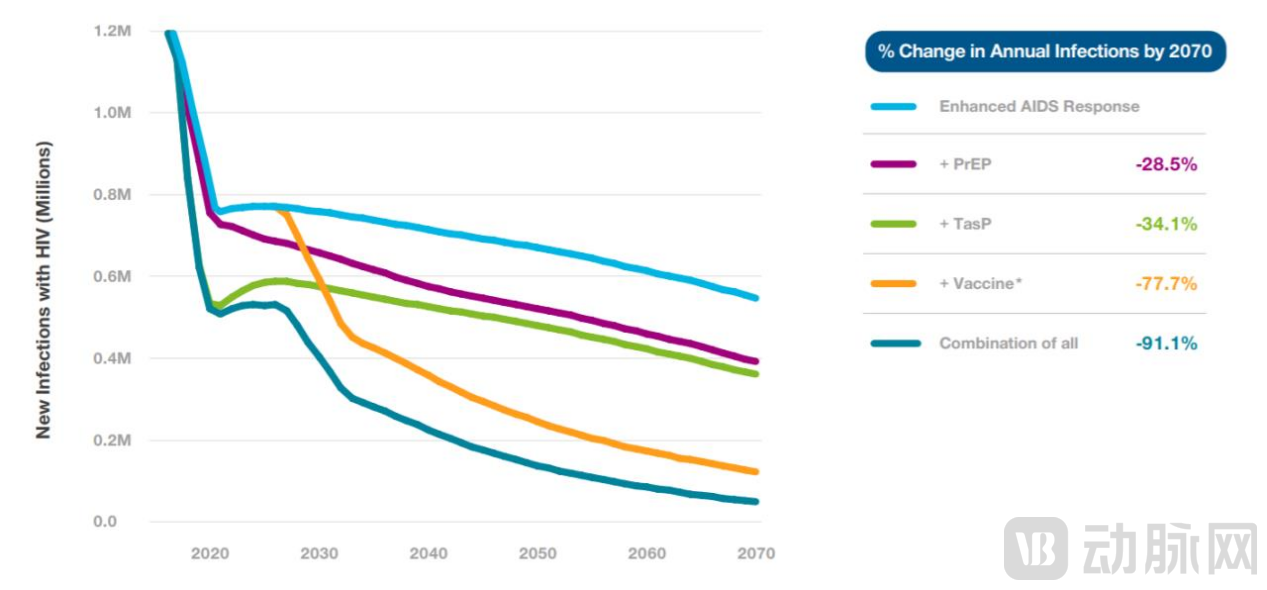
(Relative Effectiveness of Different Measures in Reducing New HIV Infections)
Therefore,To achieve sustained control of the HIV epidemic,A preventive vaccine or vaccine-like regimen that is acceptable and usable by the general population remains needed and can serve as a complement to preventive medications such as PrEP.According to an expert opinion by Anthony S. Fauci, Director of the National Institute of Allergy and Infectious Diseases, annual HIV infections are projected to decrease by 77.7% with vaccine interventions and by 91.1% with combination drug interventions by 2070.
In an interview with VCBeat, Professor Lu Shan, founder of Worcester HIV Vaccine Company (WHV), stated: “The majority of populations at high risk for HIV infection worldwide are located in impoverished, underdeveloped, and remote areas with limited access to medical care and medications. Relying solely on PrEP is insufficient to achieve large-scale population-level prevention. Vaccines offer better accessibility; a regimen of just three to four doses could provide lifelong protection against infection, with the total cost potentially no higher than that of a single course of medication. This approach is also more likely to garner support from the international community, thereby extending protection to a broader range of at-risk populations.”

Professor Lu Shan is a tenured professor at the University of Massachusetts Medical School, one of the principal inventors of DNA vaccine technology, and a primary proponent of the heterologous prime-boost immunization theory. He has served as President and Chair of the Board of Directors of the International Society for Vaccines, and as a Senior Advisor to the China National Center for Infectious Diseases. In 2018, he founded Worcester HIV Vaccine Company (WHV) in the United States, dedicated to the development of novel HIV vaccines.
In May 2024, the WHV team published an article in *The Lancet HIV*, reporting that in the multicenter Phase I clinical trial HVTN 124, all subjects who received sequential vaccination with their multivalent DNA vaccine plus multivalent protein vaccine regimen exhibited broad-spectrum antibody responses, with antibody titers reaching levels in the tens of thousands.Another article published concurrently in Nature Communications noted that WHV isolated a monoclonal antibody from vaccine recipients, which was capable of neutralizing multiple HIV subtypes.
Looking back on the turbulent nearly four-decade journey of HIV vaccine development, the multiple breakthrough results emerging from recent human clinical trials of sequential vaccination have undoubtedly renewed confidence in this solitary and arduous long-distance race. VCBeat spoke with Professor Lu Shan, who shared his reflections on more than thirty years of vaccine research and development, as well as the past, present, and future of HIV vaccines. The following interview has been edited for clarity and readability.
1Will DNA Vaccines and Sequential Immunization Strategies Become the Breakthrough for HIV Vaccines?
VCBeat: Based on what R&D accumulation and opportunities did you choose to devote yourself to HIV vaccine research and development and establish WHV?
Lu Shan:Around 1990, I specialized in immunology in the United States and subsequently became a board-certified physician in the U.S. While engaged in clinical practice, I conducted research in the field of novel vaccines. At the laboratory of Harriet Robinson, one of the three earliest laboratories worldwide to investigate nucleic acid vaccines, I participated in the early discovery of DNA vaccines and the refinement of their foundational technical frameworks.
Traditionally, conventional vaccines have primarily relied on antigen recognition to activate immune responses and induce antibody production (an antibody activation strategy). DNA vaccines build upon this foundation by incorporating foreign target gene fragments into DNA plasmids. Upon delivery into the host, these plasmids express the target protein, thereby stimulating specific B-cell and T-cell responses and generating protective immunity. In simpler terms, DNA vaccines advance beyond merely increasing antibody levels to promoting the proliferation of key immune cells—such as T cells and B cells, which are responsible for antibody generation—thereby sustaining ongoing antibody production.
Around 2008, I discovered that combining DNA vaccines with other vaccines yielded superior efficacy compared to their standalone use. Consequently, I proposed the strategy of heterologous prime-boost immunization, which involves priming with a DNA vaccine followed by boosting with a protein vaccine. This approach induces broad-spectrum, multifunctional antibody and cellular immune responses, demonstrating greater effectiveness than repeated administrations of a single vaccine.Following the COVID-19 pandemic, the concept of sequential immunization has gradually gained global acceptance, and this methodology is now employed in nearly all regimens involving the combined use of two different vaccines.
At that time, however, few people understood this highly novel concept after my review article was published. The leap from the success of a single vaccine to the combined use of two vaccines was substantial. To address this, I decided to develop the “most challenging” vaccine as proof of concept—an HIV vaccine. In 2018, WHV was established and secured exclusive licensing rights to the original HIV vaccine patents and global intellectual property through an agreement with the University of Massachusetts Medical School (UMass). Leveraging the heterologous prime-boost immunization methodology, we launched our second-generation HIV vaccine—optimized polyvalent antigens and adjuvants (PDPHV), comprising a polyvalent DNA vaccine combined with a polyvalent protein vaccine—and initiated the Phase I human clinical trial HVTN124.
VCBeat: What clinical breakthroughs were achieved with the Phase I clinical results of HVTN124?
Lu Shan:Results from the HVTN 124 trial, published in The Lancet HIV, indicate that all immunogenicity endpoints surpassed those of previous human HIV vaccine trials. The trial demonstrated high-titer and broad-spectrum immune responses, with antibody titers reaching the tens of thousands, reflecting durable immunity. This also representsFor the first time, an HIV vaccine has been shown to simultaneously induce multiple functional antibody-mediated immune responses and cellular immune responses, with no delayed-type hypersensitivity, vasculitis, or any serious clinical adverse events observed post-vaccination, demonstrating a favorable safety and tolerability profile.
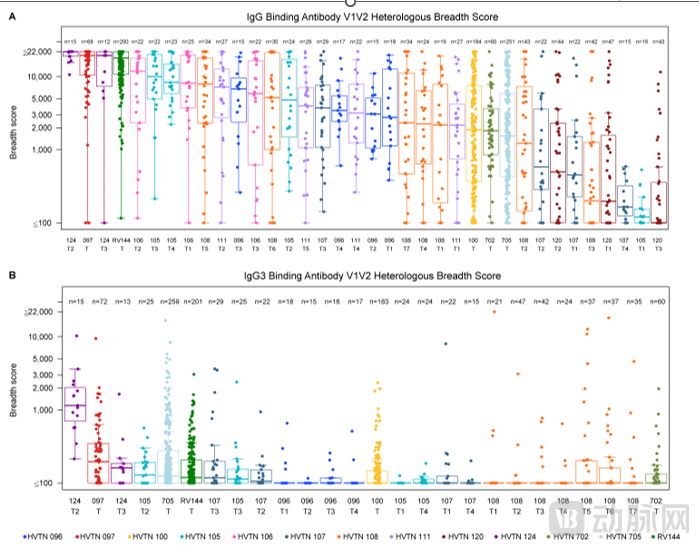
Specifically, compared with all historical HIV vaccines, HVTN124 has the best protection-correlated indicators:Antibody Responses to the V1 and V2 Regions of the Envelope Protein(negatively correlated with the risk of infection; V1V2 antibodies play a role in reducing the risk of HIV infection);HVTN 124 also induced functional antibodies with antibody-dependent cellular cytotoxicity (ADCC) activity, which has been confirmed to be associated with the protective efficacy of HIV vaccines.
Furthermore, all participants in HVTN 124 elicited high-level CD4+ T-cell immune responses. Previous trials have demonstrated that multifunctional CD4+ T cells are significantly associated with a reduced risk of HIV-1 infection.
Another article published in Nature Communications noted that we induced antibodies in volunteers capable of recognizing the CD4 binding site (CD4bs) of the HIV virus, which exhibited neutralizing antibody functions against multiple HIV subtypes, including several Tier 2 strains that are notoriously difficult to neutralize. This represents a long-sought goal in the field of HIV vaccine research.Excluding the Phase Ia HVTN 124 trial, our team completed the Phase Ib clinical trial WHV138 in December 2022 and is currently continuing to evaluate the immunogenicity results in subjects. A Phase II clinical trial is also under preparation.
VCBeat: Briefly speaking, what are the differentiated advantages of WHV multivalent DNA vaccine plus multivalent protein vaccine?
Lu Shan:HIV’s envelope proteins exhibit low immunogenicity, making it difficult to induce high antibody levels in the human body within a short period after vaccination with traditional vaccine formulations. Furthermore, HIV’s rapid replication rate and the high error rate of its reverse transcriptase lead to a high mutation frequency and the continuous emergence of new viral strains. Therefore, an effective HIV vaccine must not only rapidly elevate antibody titers and elicit broadly neutralizing antibodies but also maintain a sufficient population of antibody-producing immune cells on long-term surveillance to achieve effective protection.
Under a sequential immunization strategy, DNA vaccines encoding HIV envelope protein antigens activate antigen-specific B cell responses while preserving the native structure of viral antigens, thereby inducing high-quality protective antibodies. Protein vaccines (used for booster immunization) employ corresponding recombinant HIV envelope proteins to stimulate and amplify B cell activity, resulting in the production of substantial amounts of HIV envelope protein-specific antibodies and sustaining long-term high-titer antibody levels.
First, HVTN 124 adheres to the DNA vaccine approach. Compared with other vaccine platforms, DNA (plasmid) vectors are highly purified empty carriers that carry only the vaccine antigen and do not elicit immune responses against vector antigens, offering significant advantages as a prime regimen.Taking the failed Ad5 (replication-defective type 5 adenovirus) HIV vaccine as an example, human clinical trial results showed that the vaccine increased the risk of infection. This occurred because the immune response to the adenovirus stimulated the production of more CD4+ T cells, which are precisely the target cells for HIV infection. In the absence of robust protective antibodies, a higher number of these T cells actually exacerbated HIV infection.
Second, both the prime and boost antigens used in HVTN 124 are screened, broadly reactive, and cross-reactive antigens, without any modification to the antigen genes.Previous HIV vaccine studies have reached Phase 2b/3 trials, but they often relied on heavily modified versions of the native HIV surface antigens rather than the unmodified native antigens themselves, depended solely on T-cell immunity, or employed chimeric surface antigens. Our team has spent over a decade analyzing tens of thousands of HIV viral strains to carefully select optimal antigens, ultimately achievingThe envelope antigen in the DNA vaccine is an exact match to the envelope protein antigen in the protein vaccine, which can maximize the prime-boost effect.
Third, a globally first-of-its-kind, previously unachieved quadrivalent HIV envelope protein antigen component that can induce broad-spectrum responses.We believe that the functional antibodies induced by HVTN 124 are expected to cover more than 95% of the 16 major HIV subtypes and circulating recombinant forms worldwide.
2MNCs Exit in Succession: What Is Missing from the Repeatedly Failing HIV Vaccine Track?
VCBeat: What technological iterations has HIV vaccine development undergone globally?
Lu Shan:First-generation HIV vaccines followed classic vaccine strategies, aiming to induce neutralizing antibodies and elicit humoral immunity against HIV. These HIV envelope protein vaccines were developed based on the technological approach used for Merck’s hepatitis B surface antigen vaccine (genetically engineered). In 2003, VaxGen, the company employing this method, announced that its Phase III clinical trial had ended in failure. The only HIV component capable of inducing an immune response is the envelope glycoprotein located on the viral surface; however, the quality of the induced antibodies and the resulting humoral immunity were insufficient to provide population-level immune protection.
Second-generation vaccines focus on recombinant viral strategies targeting cellular immunity, largely employing viral vector technologies. Merck and the U.S. National Institutes of Health (NIH) inserted HIV genes into Ad5 (a replication-defective type 5 adenovirus). The HIV genes in the vaccine are expressed and translated to synthesize antigens identical to those of HIV, thereby stimulating the generation of cytotoxic T cells, but without eliciting protective antibodies. Human clinical trials demonstrated that this vaccine not only failed to prevent HIV infection but also increased the risk of infection.
Third-generation vaccines combine multiple protective antibodies with cellular immunity. A viral vector vaccine plus protein vaccine, jointly developed by an HIV research institute and the pharmaceutical giant Sanofi, achieved partial protection in human trials for the first time during the Thailand RV144 clinical study. This demonstrated the feasibility of an HIV vaccine, reducing the overall risk of HIV infection by 31.2%, and also validated the effectiveness of a sequential immunization strategy.
However, the protective efficacy observed in the RV144 clinical trial lasted only for a short period and waned over time. Subsequently, following this approach, the Johnson & Johnson-sponsored HVTN 702, 705, and 706 studies, supported by the U.S. and South African governments and the Bill & Melinda Gates Foundation, failed to replicate the protective efficacy of RV144 and were declared unsuccessful in succession.As previously mentioned, viral vector defects, viral antigen competition, and suboptimal selection of corresponding antigens can all lead to the clinical failure of third-generation vaccines.
VCBeat: Missing Success by a Narrow Margin Multiple Times—What Are the Underlying Issues Behind the High Failure Rate of HIV Vaccine Development?
Lu Shan:Over the four decades since the discovery of HIV, scientists worldwide have continuously devoted themselves to drug development and disease research. Today, long-term survival for HIV patients has been achieved through a breakthrough known as “cocktail therapy,” or Highly Active Antiretroviral Therapy (HAART), which involves the combined use of three or more antiretroviral drugs. However, in the field of HIV vaccine development, we have witnessed numerous failures by major pharmaceutical companies. Large global pharmaceutical firms have made substantial investments in HIV vaccines at various times.But it was not until Johnson & Johnson shut down its Infectious Diseases and Vaccines division in 2023 that, to date, virtually no major pharmaceutical companies have been betting on HIV vaccines.
The reasons for failure were multifaceted, such as the simple viral origin of antigens in first-generation vaccines, neglect of differences between antigens, and viral mutations during the cultivation process. While these failures were understandable, the near-complete abandonment of early antibody-based vaccines had a profound psychological impact and severely undermined confidence within the academic community. Major pharmaceutical companies gradually scaled back their HIV vaccine pipelines, reflecting an absence of industrial perspective and product-oriented thinking. Meanwhile, scientist-led vaccine research became fragmented into numerous schools of thought, predominantly concentrated in universities and research institutes.
This has led to significant challenges in vaccine development: debates in basic science have spilled over into the product stage, influencing the selection of technological pathways. Meanwhile, the sector lacks pharmaceutical industry teams, creating difficulties in product translation and hindering progress through GMP-compliant manufacturing and clinical stages, or resulting in a disconnect from real-world applications.
Furthermore, broadly neutralizing antibodies (bNAbs), which are highly sought after in HIV prevention, have become the sole benchmark for developing an AIDS vaccine. Scientists from multiple countries have isolated a series of bNAbs targeting multiple epitopes of the HIV-1 envelope protein from patients with chronic HIV infection, hoping to develop new monoclonal antibody drugs, such as VRC01, which was identified in a small number of HIV-infected individuals. The application of antibody therapeutics and gene therapy for long-term prevention represents a pioneering approach in HIV vaccine research; however, in practical implementation, the high costs are unsustainable, gene therapy technology remains immature, and its population-wide applicability and efficacy still require further validation through clinical data and other evidence.
Meanwhile, the AMP trials, which aimed to prevent HIV infection using broad-spectrum monoclonal antibodies, failed several years ago. In Phase III clinical trials, a single broadly neutralizing antibody (bNAb) was unable to protect volunteers against mutated viral strains. This setback once again dealt a blow to the HIV research community. It serves as a warning that it is highly dangerous for any scientific field to be dominated by a single approach while lacking diverse perspectives. Such homogeneity can easily lead to repeated failures and erode confidence in the field. Therefore, it is essential to encourage open dialogue and pursue various differentiated R&D pathways.
Yet funding remains a major hurdle—major pharmaceutical companies have suffered successive setbacks and, driven by commercial considerations, have repeatedly trimmed their pipelines; meanwhile, biotech investors find it difficult to assess the risks and prospects of such projects. As a result, the HIV vaccine landscape is becoming increasingly narrow, with players hesitant to deviate from mainstream, consolidated approaches. Nevertheless, even in this challenging environment, we have observed sustained interest from venture capitalists in China and the United States in vaccine products, along with active investment efforts aimed at propelling clinical development forward by a significant leap.
3How Should We View the Future of HIV Vaccines?
VCBeat: How is the global development of HIV vaccines progressing in terms of R&D funding and payment mechanisms?
Lu Shan:The U.S. National Institutes of Health (NIH) has long supported global HIV vaccine research, and we at WHV are among the recipients of this support.In terms of R&D progress, the WHV pipeline is currently in a globally leading position, as the only investigational vaccine pipeline worldwide on the verge of entering Phase II clinical trials. It has received over $50 million in funding from the NIH, with nearly $10 million in capital investment.
As previously discussed, major pharmaceutical companies have been slashing their HIV vaccine pipelines, driven by a fundamentally simple business logic:Similarly, despite the high R&D expenditures, HIV drugs entail long-term or even lifelong treatment, whereas vaccination represents a “short-term business.” However, we must not view the future of HIV vaccines through this single lens.
The World Health Organization (WHO) has pointed out that HIV remains a major global public health issue, requiring countries worldwide to jointly implement the Global HIV Strategy to achieve the goal of ending the HIV epidemic by 2030. Over the past two decades, providing aid and drug donations to severely affected regions in Africa based on community services has become a mature model. For example, the AIDS Healthcare Foundation (AHF), a non-profit organization based in Los Angeles and one of the largest providers of HIV/AIDS medical services globally, has provided treatment and related support services to 2.029 million people living with HIV in 46 countries around the world.
Whether it is the decline in mortality rates, the reduction of social burden, or the long-term boost to GDP, I believe that an HIV vaccine will never lack payers. This is because HIV prevention does not fit any ordinary commercial healthcare model; ultimately, it will rely on a public health-dominated payment model.For example, international organizations and charities such as UNICEF, the WHO, and Gavi, the Vaccine Alliance, which have long been invested in HIV/AIDS prevention and control, will actively pay for truly effective HIV vaccines.
Certainly, we also look forward to innovations in payment and business models. Recently, I co-authored a commentary with the International AIDS Society (IAS), which mentioned thatAdvancing the Global R&D of HIV Vaccines Through Biotechnology Companies. Biotech firms possess immense potential in innovation and development capabilities, with their primary challenges being funding and resources.—Venture capital, private investment, and foundations should be deeply integrated with non-public-welfare organizational models, government-led models, and others, thereby supporting greater potential for innovation in the future.This is an opportunity for everyone to make money while working together to drive development.
VCBeat: What are your plans and expectations for WHV in the near future?
Lu Shan:In terms of short-term development strategy, we aim to demonstrate the vaccine’s efficacy and protective effect with minimal cost and maximum speed.WHV has obtained the FDA’s pre-IND approval, the vaccine required for clinical trials has been manufactured, and the Phase 2a clinical trial of WHV238 is also expected to commence within the year.The objective of WHV238 is to confirm the immunogenicity and safety of the vaccine in a larger population. Meanwhile, the Phase 2b efficacy trial will be conducted in South Africa.In China, we are also actively engaging with relevant authorities and HIV/AIDS research institutions, aiming to facilitate the practical application of our technologies and collaborate with domestic scientists on product development.
We hope to see the deployment of HIV vaccines in Africa within the next five years, allowing us to observe their effectiveness in population-level prevention. This is an ambitious goal; the key challenge lies not in technical hurdles, but in the coordination and communication required for global collaboration, organization, and resource allocation. However, this is precisely where our team’s strengths lie, bolstered by a powerful Scientific Advisory Committee that includes Professor Stanley Plotkin, known as the “Godfather of Vaccines”; Michel De Wilde, former Global President of Sanofi’s Vaccine Division; and Zak Huang, former Head of Product Registration and Clinical Development at Merck/CSL. At the same time, we welcome additional funding, resources, and support from more partners to join us in this endeavor that benefits all of humanity.
VCBeat: How should we view the future of HIV vaccines?
Lu Shan:For a long time, many professionals in the biological, academic, and industrial sectors held a pessimistic view of HIV vaccines, believing them to be unattainable due to lack of understanding or focusing solely on past failures. I believe this mindset is even more disheartening than the scarcity of teams dedicated to vaccine development. In fact, over the past 40 years, few HIV vaccine candidates have advanced to Phase II or III clinical trials. However, based on more than a decade of research into HIV vaccines, scientists worldwide have enhanced their understanding and application of vaccine technologies, which have since been applied to the development of vaccines for COVID-19 and other diseases.
Before results emerge, no one can predict “zero-to-one” breakthroughs. Yet without laying the groundwork through painstaking efforts, such breakthroughs would not occur. If multiple teams worldwide engage in HIV vaccine development, we may see even greater and more substantial progress. Therefore, by opening up technological pathways and accumulating population-level data, we call on the community to adopt diverse strategies and technical approaches to jointly advance HIV vaccine research and development.
Scientific advancement is boundless, and science alone cannot precisely quantify commercial returns or market profits. However, by adhering to the essence of scientific inquiry, employing rigorous and pragmatic methodologies, and maintaining an objective and self-reflective mindset in research and development, we are confident in creating products that deliver superior clinical data while balancing social and economic value.