A $100B+ Medical Market Serving Nearly 200 Million Patients Remains Underpenetrated
“Endure it.”
This is the final decision that a patient diagnosed with endometriosis (hereinafter referred to as “endometriosis”) might make in early 2025.
This counterintuitive case stands out particularly starkly at a time when the generic drug market is characterized by cutthroat competition and concerns over an oversupply of innovative drugs are gradually emerging. In fact, patients with endometriosis do not lack pharmacological options: first-line treatments include oral contraceptives; gonadotropin-releasing hormone (GnRH) agonists, such as leuprorelin; and other hormonal therapies. As a last resort, surgical intervention remains available.
Endometrial tissue normally grows within the uterine cavity and is expelled from the body with menstrual blood each month. Endometriosis occurs when this endometrial tissue fails to be discharged normally during menstruation and instead implants in other parts of the body. Patients with endometriosis may experience severe, life-disrupting dysmenorrhea, dyschezia and/or dysuria, chronic pelvic pain, abdominal bloating, nausea, fatigue, and even infertility, depression, and anxiety. More distressingly, these symptoms can persist from menarche until menopause.
“Then why keep enduring it?”
The patient told VCBeat that during her medical consultations, the doctor had recommended goserelin acetate sustained-release implants. Initially, this injection was indicated for prostate cancer. Subsequently, the doctor advised her to opt for the more established procedure of inserting an intrauterine hormonal device, which involves surgically placing a T-shaped plastic frame that releases progestin into the uterus.
However, given the patient’s diagnosis of mammary hyperplasia (also commonly referred to as mammary adenosis, fibrocystic breast disease, or fibrocystic changes of the breast—a benign condition arising from dysregulated processes of breast development and involution) and the risk that hormone therapy could exacerbate this condition, the recommendation was put on hold. Furthermore, considering the patient’s proximity to menopause, a comprehensive assessment led to the decision to continue using conventional analgesics, thereby prioritizing the management of the primary clinical issue.
This is merely one case among the thousands of patients with endometriosis, and her symptoms remain within a tolerable range.
According to WHO and McKinsey statistics, endometriosis affects approximately 10% (190 million) of women of reproductive age worldwide. Currently, there is no cure; the condition is commonly referred to as “cancer that does not kill.” Existing treatment modalities primarily aim to control symptoms and include surgery and long-term pharmacological management. The postoperative recurrence rate has been rising year by year, reaching up to 50% within five years after surgery.
Etiology remains unclear, laying the groundwork for pitfalls from the diagnostic stage onward
“In recent years, the number of patients diagnosed with endometriosis has been increasing, with a significant proportion being young women,” a gynecologist at a top-tier tertiary hospital in Southwest China told VCBeat. The reasons for the growing patient population remain unclear, but it is speculated that they may be related to the overall delay in childbearing age among women, changes in dietary patterns, and the pressures of modern society.
Meanwhile, the other party noted that confirming a patient’s diagnosis requires navigating numerous hurdles along the way.
“Patients with dysmenorrhea often do not give it much thought, believing that they can simply endure the pain until it passes. As a result, they generally do not seek outpatient care, let alone pursue a definitive diagnosis.” Insufficient attention to dysmenorrhea is a major factor contributing to delayed diagnosis of endometriosis. As the most prevalent clinical manifestation of endometriosis, dysmenorrhea serves as a distress signal from the body, yet it has long been overlooked.
For patients with slightly more severe symptoms, a visit to the outpatient clinic often yields no definitive results despite undergoing various tests, including transvaginal ultrasound and a six-panel hormone assay. One physician even noted, “Some patients reported being misdiagnosed with ‘suspected polycystic ovaries’ or even ‘acute appendicitis,’ which delayed appropriate treatment.” A final diagnosis is often only reached during the family-planning stage: after discovering persistent infertility, patients seek care at multiple facilities before the underlying cause is finally identified.
If delayed diagnosis is strongly correlated with patient awareness and health education, then the delayed diagnosis of endometriosis is associated with the lack of effective non-invasive diagnostic methods. Clinically, diagnosis is typically made by directly observing intrauterine tissues (endometrial tissue) via laparoscopic surgery. Although this approach is regarded as the “gold standard” for diagnosing endometriosis, it is invasive and incurs high costs. Furthermore, while ultrasonography is one of the primary diagnostic tools for endometriosis, its accuracy is limited.
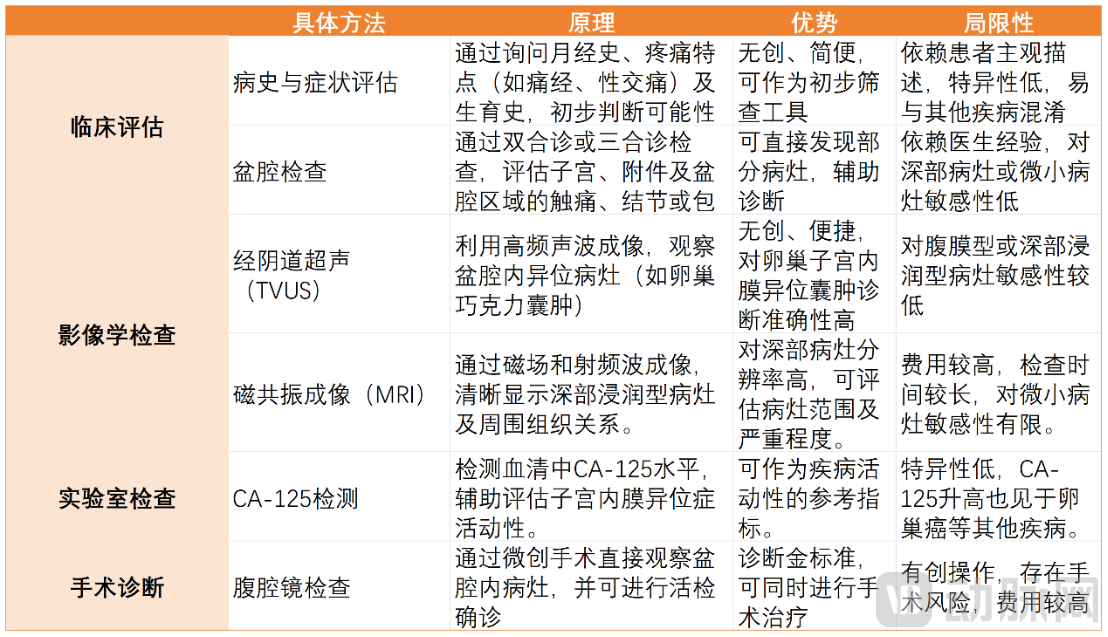 Current Diagnostic Methods for Endometriosis and Their Limitations, Chart Compiled by VCBeat
Current Diagnostic Methods for Endometriosis and Their Limitations, Chart Compiled by VCBeat
Another diagnostic approach is the gynecological physical examination (bimanual and rectovaginal examinations), which can accurately identify endometriosis based on the location of lesions, particularly deep infiltrating endometriosis. However, the findings are highly dependent on the physician’s experience and examination skills, and not every clinician has mastered these techniques. Consequently, whether an effective diagnosis is made can sometimes depend on the patient’s luck.
Therefore, the development of non-invasive, high-sensitivity biomarkers (such as miRNAs and proteomic markers), enabling early diagnosis through detection in blood, urine, or endometrial fluid, has emerged as a new direction for future early screening and diagnosis. Notably, this trend is more prominently reflected in the early screening of endometrial cancer or ovarian cancer.
The latest 2024 research from the University of Utah in the United States shows that, compared with women without endometriosis, women with any type of endometriosis have a 4.2-fold higher risk of developing ovarian cancer, while women with severe endometriosis have approximately a 10-fold higher risk. This study is expected to further guide market actions.
However, despite new insights into the diagnosis and treatment of endometriosis both domestically and internationally—emphasizing its nature as a chronic disease requiring early diagnosis and treatment, comprehensive management, and long-term care—key questions remain unresolved. Specifically, the academic community has yet to reach a definitive consensus on why endometrial tissue, which should be expelled from the body with menstrual blood, becomes ectopically implanted in extrauterine sites, and precisely how this ectopic implantation occurs.
Current theories can only explain the mechanisms underlying some lesions. Among these, the implantation theory has long dominated the scientific literature, suggesting that certain lesions may be associated with the retrograde flow of menstrual blood through the fallopian tubes. In patients with endometriosis, endometrial cells attach to the peritoneum in an abnormal state. However, this theory currently fails to account for endometriosis in women with congenital absence of the uterus, adolescent girls, or the rare cases of male endometriosis. Clearly, endometriotic cells are not merely uterine cells transplanted to the abdominal cavity; the development of endometriotic lesions involves additional mechanisms.
Others may result from the transformation of normal cells (transitional cells) into endometriotic cells. This theory can explain the occurrence of endometriotic cysts in the ovaries and lesions in the pelvis.
According to Müllerianosis theory, other lesions may originate from embryonic remnants. This theory can explain why endometriotic lesions have a high incidence in the retro-uterine area and on the uterosacral ligaments, whereas their incidence is lower on the ovaries, sigmoid colon, appendix, or diaphragm. Furthermore, a recent theory emphasizes epigenetic changes occurring in normal endometrial cells, positing that such changes are responsible for the development of intraperitoneal endometriotic lesions.
In other words, the etiology of endometriosis remains unclear to date.
Billion-Dollar Molecules Take Their Seats, but the Blockbuster Drug Has Yet to Arrive
This has become a major challenge in the development of related novel therapies.
When the etiology remains unclear, targeted therapy becomes unfeasible. Currently, there is no known cure for endometriosis; therefore, treatment primarily aims to control symptoms. First-line therapy mainly consists of low-cost combined oral contraceptives (COCs), which offer moderate efficacy, with approximately one-third of patients showing non-response (potentially associated with progesterone receptor variants). Furthermore, although oral contraceptives have relatively fewer side effects, they still present limitations. Similar to glucocorticoids used in the treatment of systemic lupus erythematosus, which are inexpensive but carry significant adverse effects, these limitations have driven the industry to develop more advanced biologic agents.
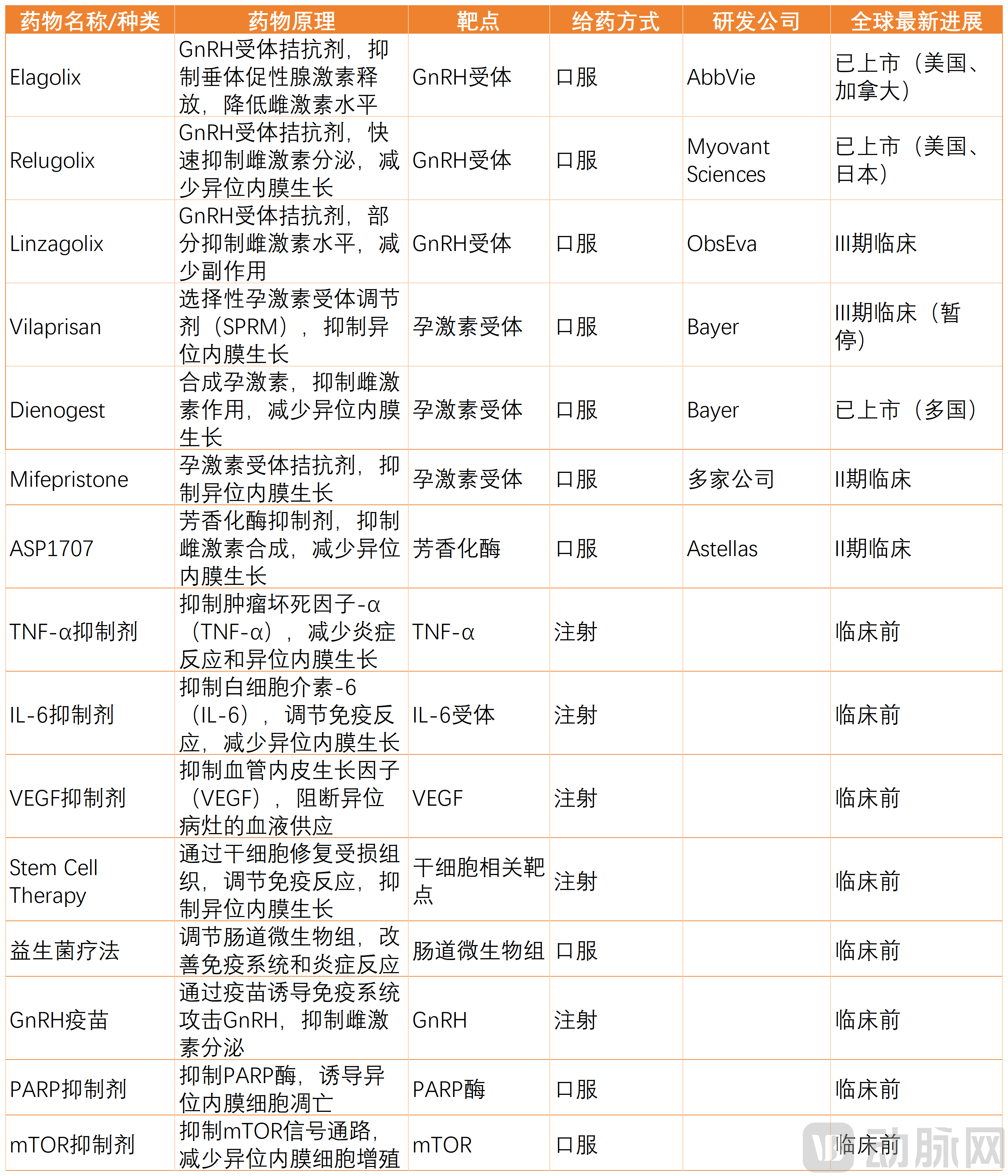
In recent years, one of the most significant advancements in the global treatment of endometriosis has been the development of GnRH (gonadotropin-releasing hormone) antagonists. Notably, injectable GnRH agonists are regarded as the “gold standard” for pharmacological management of endometriosis in the Chinese Expert Consensus on Long-term Management of Endometriosis.
However, these medications are associated with side effects and can cause infertility during treatment. Furthermore, existing hormonal therapies carry additional risks, including cardiovascular complications, breakthrough bleeding, osteoporosis, and depression—particularly osteoporosis and depression. Recovery from osteoporosis is slow and, in some cases, irreversible; meanwhile, depression significantly impairs patients’ quality of life, contravening the principles of chronic disease management.
Representative among these is AbbVie’s elagolix sodium (Elagolix), the first GnRH antagonist approved in the United States in 2018 for the treatment of moderate-to-severe endometriosis. In addition, relugolix, an oral GnRH receptor antagonist developed by Pfizer/Myovant, has also achieved strong sales performance in the market. However, in the progestin segment, Visanne, although approved in China, Japan, and certain European countries, has not yet received FDA approval.
Meanwhile, the market share of these drugs remains significant. Taking leuprorelin as an example, its current global sales amount to approximately USD 2.5 billion. According to IQVIA’s sample-based statistical estimates, the terminal sales revenue of leuprorelin in China reached approximately RMB 4.66 billion in 2023.
Livzon Group Seizes the First-Mover Advantage in China. At the end of 2024, Livzon Group announced that its Leuprorelin Acetate Microspheres for Injection had passed the Consistency Evaluation of Quality and Efficacy for Generic Injectables. According to the company’s announcement, this is the first long-acting GnRH sustained-release formulation globally to gain approval after completing bioequivalence studies in accordance with the U.S. FDA’s product-specific guidance.
However, although the latest GnRH antagonists can effectively alleviate pain, they also suppress estrogen more severely, leading to more severe depression. Therefore, despite the relief of pain, patients' mood has not significantly improved. Meanwhile, due to a series of side effects, whether this type of drug can be used long-term remains questionable, and it is currently not covered by medical insurance.
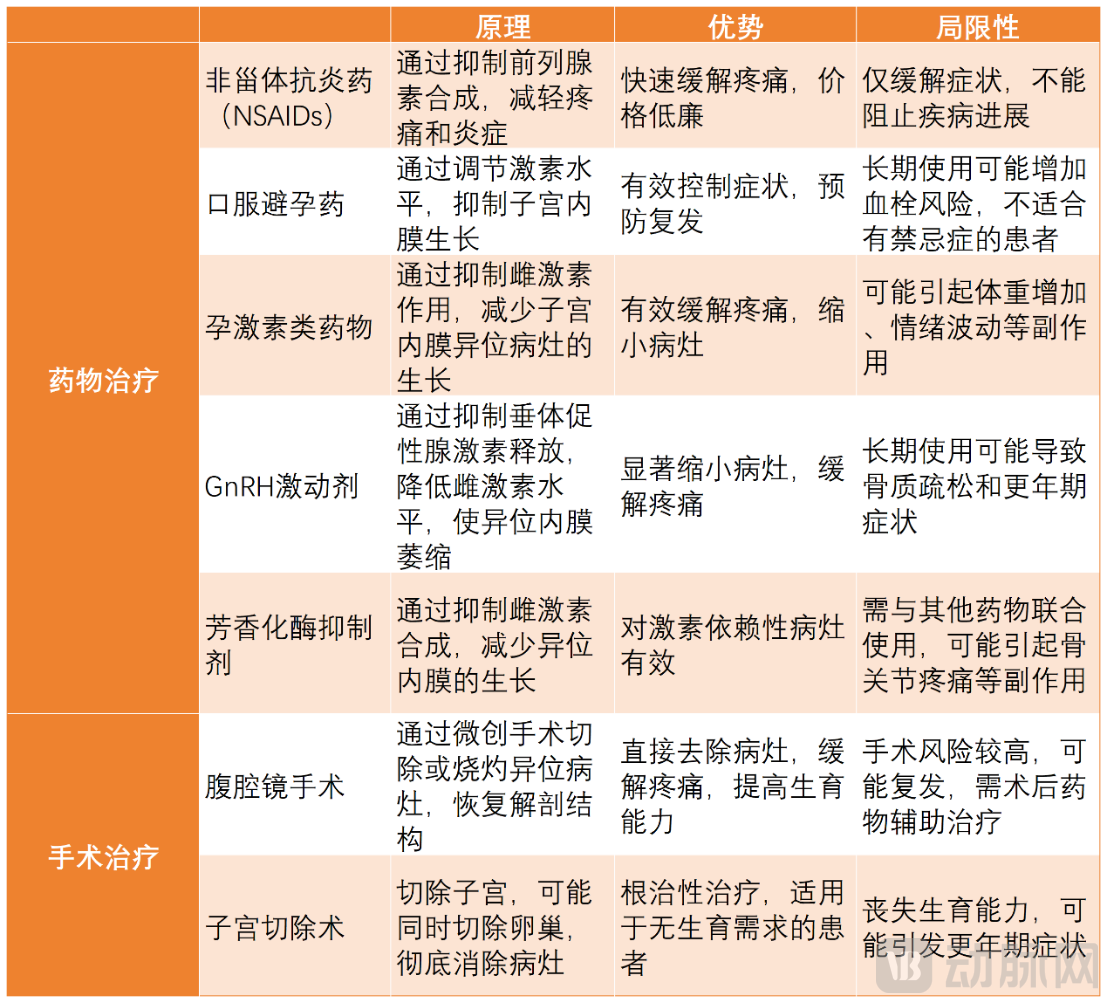
Current Main Treatment Modalities for Endometriosis and Their Limitations, Chart Compiled by VCBeat
MNCs “Retire,” Domestic Biotechs Step into the Ring
Issues such as suboptimal efficacy, impairment of daily living, difficulty in individualized dose adjustment, and adverse reactions from long-term use often lead patients to discontinue treatment, resulting in disease relapse and reduced quality of life. Taking injectable GnRH agonists as an example, the predominant administration routes are subcutaneous or intramuscular injections, typically required every four weeks; thus, patient convenience and accessibility have not yet met expectations.
But even more detrimental are its unpredictable side effects. Upon binding to GnRH receptors, GnRH agonists initially trigger a transient surge in the release of FSH and LH, leading to a rapid rise in estrogen levels. This exacerbates patients’ symptoms in the short term, a phenomenon known as the “flare effect.” For patients, the first hurdle in using GnRH agonists is enduring this initial worsening of symptoms and waiting patiently for several weeks before therapeutic effects take hold.
After 2–3 weeks of administration, receptors become desensitized to GnRH agonists due to saturation or depletion, leading to suppressed estrogen levels. However, women with normal menstrual cycles typically require approximately three months after discontinuation to resume ovulation. Therefore, patients attempting to conceive need a longer waiting period for pituitary function to recover. Meanwhile, the profoundly low estrogen levels can cause significant perimenopausal symptoms, including hot flashes, vaginal dryness, mood instability, and sleep disturbances.
Therefore, the strategy for new drug development has gradually become clearer.
To sustain deep engagement in the field of GnRH receptor antagonists, address clinical pain points, and emerge as a strong competitor, efforts must focus on eliminating the flare effect, achieving rapid onset of action, facilitating swift recovery of pituitary function, and ensuring convenient administration. Chinese biotech companies are actively advancing in this arena.
Linzagolix, a GnRH receptor antagonist exclusively licensed by Baozheng Pharma, has enrolled its first patient in the Phase III clinical trial for endometriosis. It is the world’s first orally administered small-molecule GnRH antagonist with adjustable dosing. Its distinct mechanism involves competitive binding to GnRH receptors, directly inhibiting the hypothalamic-pituitary-gonadal axis and rapidly reducing follicle-stimulating hormone (FSH) and luteinizing hormone (LH) levels after administration. Unlike GnRH agonists, GnRH antagonists can be administered at any time during the follicular phase, exert an immediate suppressive effect, and allow pituitary function to recover within 2 to 4 days after discontinuation.
Another approach bypasses traditional treatment regimens to seek entirely novel solutions.
Given the limitations of existing medications, top experts in China—including authorities in the field of endometriosis research such as Academician Lang Jinghe, Honorary Director of the Department of Obstetrics and Gynecology at Peking Union Medical College Hospital and member of the Chinese Academy of Engineering, and Academician Chen Zijiang—have all pointed out that an innovative non-hormonal therapy is urgently needed.
Meanwhile, in China, fertility is a major concern, making treatment regimens that do not compromise conception particularly important.
HMI-115, Herui’s monoclonal antibody targeting the prolactin (PRL) receptor, was launched precisely in line with this approach.
Prolactin (PRL), also known as lactotropin or luteotropic hormone, is a protein hormone secreted by the acidophilic cells of the anterior pituitary gland. Its primary functions include promoting mammary gland development and growth, stimulating and maintaining lactation, and stimulating the generation of luteinizing hormone (LH) receptors in ovarian follicles. The main mechanism of action of HMI-115 lies in blocking prolactin receptors, thereby inhibiting the prolactin signaling pathway. Notably, HMI-115 is not required during pregnancy and breastfeeding. If pain recurs after the lactation period (i.e., after weaning), treatment with this medication can be initiated, thus perfectly avoiding the periods of lactation and most of the pregnancy.
Notably, both Baozheng Pharma and Heqirui have emphasized a dual-drive strategy combining independent R&D with license-in acquisitions. Heqirui’s HMI-115 is based on Bayer’s intellectual property, marking the only time in Bayer’s 160-year history that it has granted global rights to a Chinese biotech company.
One reason is that, despite having the financial resources to invest in R&D for new endometriosis drugs, these MNCs have seen returns fall short of expectations.
Over the past decade, the FDA has approved two products for the management of endometriosis-associated pain: AbbVie’s Orilissa in 2018, and Pfizer’s Myfembree, developed in partnership with Myovant Sciences, in 2022. However, both Orilissa and Myfembree cost approximately $1,000 per month, do not address the underlying cause of the disease, and are limited to a maximum treatment duration of two years due to the risk of reduced bone mineral density. Consequently, sales of Orilissa and Myfembree have been lackluster, a outcome that has inevitably influenced the subsequent strategic decisions of multinational corporations (MNCs). In this context, divesting pipeline assets has emerged as a viable option.
In the realm of domestically developed innovative drugs, the trend of shifting toward license-out deals in oncology and autoimmune diseases has not extended to the therapeutic area of gynecological disorders, represented by endometriosis. An investor who has long focused on the women’s health sector told VCBeat, “Global attention remains far insufficient, and this ‘insufficiency’ is multidimensional. There is limited patient awareness, inadequate market education, and a lack of sufficient etiological research for many gynecological conditions, making precise diagnosis difficult. These factors have collectively led to a gap in innovative drug R&D. Furthermore, the high barriers to drug development demand substantial source innovation, meaning that typically only multinational corporations (MNCs) are willing to commit the necessary funding. In the primary market, capital tends to flow more readily into digital health companies focused on women.”
Next Step: Expand the Overall Market Size
However, patients are not satisfied with merely the digital management of their own symptoms.
This investor told VCBeat that with the surge in popularity of topics such as reproductive health and medical aesthetics, the market has already validated the purchasing power of women in consumer healthcare. However, when this demographic becomes patients with gynecological diseases and seeks care at hospitals, they find a scarcity of effective medications, leaving substantial clinical needs unmet. She stated that viewpoints such as “the domestic innovative drug market is prosperous and saturated, or even oversupplied” do not apply to this field.
Fortunately, patient-side feedback is drawing new investors’ attention to this sector.
Liu Yabo, Chief Medical Officer at Hairong Capital, stated that he first learned about Herui’s novel drug for the treatment of endometriosis through Professor Xiao Ruiping’s appearance on CCTV’s program “Voice,” which subsequently drew his attention to related reports. “Although McKinsey’s 2024 report estimates the global market size for endometriosis at approximately $200 billion, limited disease awareness and prioritization may lead to an underestimation of the market potential in this field by the capital markets.”
Meanwhile, he also hopes that relevant companies can demonstrate their market potential to attract investment. Currently, most domestic biotech firms are in the R&D stage, with immature business models. Companies that have advanced to Phase II or III clinical trials still need to establish clear commercial and profitability models to showcase their future earnings expectations to the capital markets.
In fact, addressing gynecological conditions such as endometriosis, or other sex-specific diseases, can yield substantial returns. Consider this: when Viagra for erectile dysfunction was first launched in 1995, it was estimated to affect 152 million men. Within the first three months of its U.S. market debut in 1998, it generated $400 million in sales revenue. By 2012, global sales had reached a record $2.1 billion. Given the prevalence of diseases like endometriosis and the significant unmet medical needs, the market potential for innovative therapies is enormous.
Liu Yabo also pointed out the competitiveness that investors look for in relevant innovative drugs.
First is the innovative mechanism of action, which focuses on whether a drug possesses a unique and novel mechanism. For instance, HMI-115 from Hermed Medical Inc. targets the prolactin receptor rather than following traditional pathways such as those targeting estrogen. This innovative mechanism may enable more precise and effective treatment while minimizing interference with other physiological systems.
Non-hormonal therapies offer certain advantages. Non-hormonal agents can avoid side effects associated with hormonal therapy, such as weight gain, mood swings, and bone loss, thereby improving patients’ quality of life and medication adherence. For patients with contraindications to hormone use or concerns about hormonal side effects, non-hormonal therapeutic options are highly appealing.
In terms of clinical data, key considerations include the symptom relief rate (such as the extent and speed of pain relief, including dysmenorrhea and chronic pelvic pain, as well as the improvement in physical signs like pelvic masses and nodules), the disease recurrence rate, and any impact on fertility function.
Furthermore, for endometriosis patients requiring long-term medication, the long-term safety profile of the drug and a more convenient route of administration are also advantageous.
The predicament facing the R&D landscape for endometriosis may well be just the tip of the iceberg among myriad diseases. Guidance from investors could help emerging players entering this field avoid common pitfalls. After all, with nearly 200 million patients suffering from a lack of effective therapies, the immediate priority is to provide patients with as many treatment options as possible.
“The allure of innovative drugs lies in the fact that competition never ceases, yet the race in the endometriosis therapeutic area has not even begun.” In addressing the treatment of such conditions, the optimal strategy is always to first expand the overall market.