Neuromodulation for Premature Ejaculation: 'Chinese Innovation' Leads Global Technological Revolution
Premature ejaculation is one of the most common sexual dysfunction concerns among men worldwide. Survey data indicate that over 30% of adult men have experienced diminished ejaculatory control at various stages of life. Although traditional oral medications (such as dapoxetine) offer some therapeutic benefit, they are often associated with adverse effects including dizziness, nausea, fatigue, and decreased libido, while their efficacy remains relatively limited. Data from numerous large-scale clinical studies show that dapoxetine only extends the intravaginal ejaculatory latency time (IELT) in patients with premature ejaculation from an average of 1 minute to 2–3 minutes. Consequently, many patients discontinue treatment within a few weeks, with relevant research indicating a one-year discontinuation rate for dapoxetine as high as 90%. Furthermore, delay sprays containing irritants such as alcohol and Sichuan pepper expose patients to various adverse effects, including numbness, redness, swelling, and loss of sexual pleasure, posing significant challenges to long-term adherence. Meanwhile, behavioral therapies, including Kegel exercises, essentially train muscles rather than directly intervening in the nervous system. Since ejaculation is governed by neural mechanisms, behavioral therapies face substantial challenges in terms of training efficiency and sustained improvement. Most men find it difficult to maintain consistent practice, resulting in suboptimal outcomes.
So, beyond oral medications, topical delay sprays, and Kegel exercises, are there any new therapeutic research directions? The answer is yes—and they are becoming increasingly mature. This article provides an in-depth overview of the research progress in neuromodulation techniques for the treatment of premature ejaculation worldwide.
Ejaculation is a complex neuroreflex process, coordinately controlled by the cerebral cortex, hypothalamus, and spinal ejaculatory centers (primarily located in the sympathetic ganglia at T12–L1 and the parasympathetic and somatic nerves at S2–S4). It is initiated by afferent signals via the dorsal nerve of the penis and completed by rhythmic contractions of structures such as the pelvic floor muscles and prostate, resulting in semen expulsion.
The core mechanism of neuromodulation technology involves applying external electrical signals to the afferent and efferent nerves involved in the ejaculatory reflex—such as the dorsal penile nerve, tibial nerve, and sacral plexus—to modulate neural excitability, alter nerve conduction velocity, or stimulate gating pathways. This ultimately raises the ejaculatory threshold and delays the initiation of the ejaculatory reflex. Techniques such as pulsed radiofrequency utilize non-ablative electric fields to remodel neural response sensitivity and central plasticity, gradually normalizing the "hypersensitive neural pathways" associated with premature ejaculation.
I. Low-Frequency Electrical Stimulation Technology: Impact on Neural Reflexes
Transcutaneous Posterior Tibial Nerve Stimulation (TPTNS): Modulating the Brain’s Ejaculatory Control Circuitry via the Tibial Nerve at the Ankle
A clinical study conducted by the Colombian scholar Uribe’s team demonstrated that transcutaneous posterior tibial nerve stimulation (TPTNS) has a significant delaying effect in patients with premature ejaculation.
● Treatment Plan: 3 times per week, 30 minutes each time, for 12 consecutive weeks
● Results: Intravaginal ejaculatory latency time (IELT) increased from a mean of 32.4 seconds to 156.7 seconds at Week 12, 223.9 seconds at Week 24, and 176.7 seconds at Week 48, representing a 4.8- to 6.8-fold improvement.
● Mechanism: The tibial nerve originates from the sacral plexus and is associated with the reflex/emission control centers of the pelvic floor, prostate, and seminal vesicles, achieving the effect of "reflex arc intervention" through remote modulation.
Transcutaneous Dorsal Penile Nerve Stimulation (TDPNS): Targeting the Most Direct “Conduction Nerves”
A 2022 case study on TDPNS (Transcutaneous Dorsal Penile Nerve Stimulation) was published in the *Asian Journal of Urology*:
The patient received surface electrical stimulation at 20 Hz with a pulse width of 200 μs for 30 minutes, continued for 24 weeks.
Ejaculation latency increased from 0.6 minutes to 4.8 minutes, with sustained efficacy at 9 months
● Advantages: Precisely targets the dorsal nerve of the penis to modulate the “afferent sensation” component of the ejaculatory reflex pathway, without drugs, anesthesia, or reliance on partner cooperation.
“Virility Medical’s Transcutaneous Electrical Stimulation (TES) Technology: A Technological Exploration from Israel”
The Virility Medical team in Israel applied transcutaneous electrical stimulation (TES) to the bulbocavernosus muscle, aiming to disrupt the rhythmic ejaculatory reflex through sustained partial muscle contraction.
● Results: Patients experienced an average approximate doubling of IELT.
● Innovations
Low-Frequency Neuromuscular Electrical Stimulation (Research by Anhui Medical University)
A Randomized Controlled Trial by Anhui Medical University on Patients with Premature Ejaculation Due to Penile Hypersensitivity:
Low-frequency stimulation used alone (5–6 times per week for 3 months) demonstrated efficacy comparable to that of lidocaine spray;
The combination of low-frequency stimulation and anesthetics demonstrated the most significant efficacy, with marked improvements in IELT and nerve evoked potentials.
● Note: Electrical stimulation may not only improve neural response thresholds but also reshape central reflex mechanisms.
In summary, the treatment process for premature ejaculation using low-frequency electrical stimulation is relatively cumbersome, often requiring 2–3 months to take effect, and faces significant challenges in maintaining long-term efficacy. Therefore, this field has struggled to achieve industrialization.
II. Minimally Invasive Pulsed Radiofrequency: A Mature Neuromodulation Technology in Hospitals
In hospitals, minimally invasive pulsed radiofrequency (PRF) has been widely used for nearly 30 years in the treatment of conditions such as chronic pain, neural hypersensitivity, and nerve entrapment. Supported by robust evidence-based medicine and recommended by numerous domestic and international treatment guidelines, it is one of the common fundamental therapies in the field of pain management. In Europe and the United States, andrology specialists have been employing minimally invasive PRF neuromodulation technology to treat premature ejaculation for over 15 years. Its basic principle involves modulating the conduction and excitability of the dorsal penile nerve through a low-heat pulsed electric field, thereby achieving a "soft modulation" therapeutic effect rather than a destructive one.
Pulsed Radiofrequency Therapy for Premature Ejaculation: A Summary of Three Key Published Studies from Europe:
● 2010 Turkish study: IELT increased from 18 seconds to 139 seconds
● 2021 study (Al-Syaad): increased from 33.4 seconds to 188.4 seconds
● 2023 Russian Study (Yakov B. Mirkin): Average extension of more than threefold
Technical Limitations: Despite its proven efficacy and favorable safety profile, its application is limited due to the need for local puncture and operating room procedures; currently, in Europe and the United States, it is reserved only for severe cases of premature ejaculation that have failed all other therapies.
III. Non-Invasive Pulsed Radiofrequency: Bringing Hospital-Grade Technology into the Home
——Dianjile, a home-use physical trainer based on the principle of pulsed radiofrequency (PRF)
Addressing the aforementioned issue that “minimally invasive pulsed radiofrequency therapy for premature ejaculation is safe and effective but inconvenient,” the scientific research team at Guangzhou Aoxiang Medical has, through years of development, innovatively transformed traditional large-scale, surgery-requiring minimally invasive pulsed radiofrequency equipment used in hospitals into a non-invasive, compact, home-use physical training device sized like a lighter. This enables users to independently perform nerve desensitization training at home with privacy.

Innovations of the Dianjile-10KHz Non-Invasive Pulsed Radiofrequency Physical Trainer:
* Utilizes 10 kHz non-invasive pulsed radiofrequency technology, with the electrode making non-invasive contact with the treatment area to modulate the sensitivity of the subcutaneous dorsal penile nerve at the contact site through the electric field effect of pulsed radiofrequency;
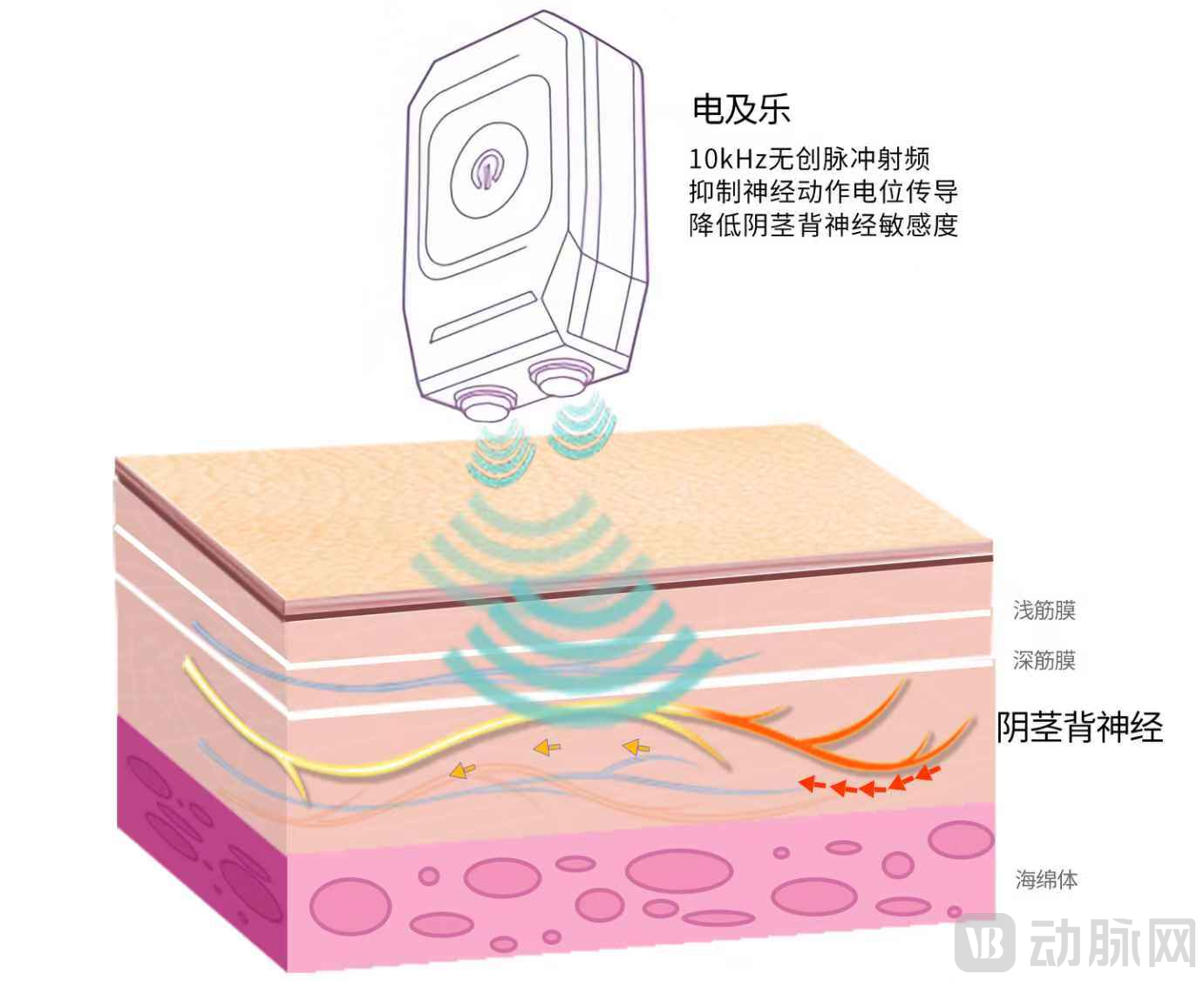
* The training method is similar to fitness exercises. Using a handheld device, keep the electrode head in close contact with the middle part of the penile shaft for 3 minutes to complete one session. The process is painless, with only a very slight tingling sensation, offering convenience and privacy.
Observational data from a cohort of 100 male patients, selected by clinical experts, with most having an intravaginal ejaculatory latency time (IELT) of less than 1 minute and having failed various existing therapies, after a two-month trial use of Dianjile:
1. Users train twice daily at home, with each session lasting 3 minutes. After 2 weeks, over 70% of users reported a significant increase in duration, with some improving from 30 seconds to more than 6 minutes. After 2 months, the intervention demonstrated a 90% efficacy rate, among whom approximately 60% achieved an increase of 3–5 minutes, and 30% achieved an increase of 6–10 minutes.
2. No medication, no anesthesia, and no side effects; it does not affect sexual pleasure or physical health.
3. Supports long-term cumulative training, with each session lasting 3 minutes for progressive strengthening; alternatively, it can be used for a short 10-minute session prior to sexual activity for immediate readiness.
4. Broad applicability: Suitable for both men with premature ejaculation (lasting around 1 minute) and those seeking to prolong intercourse to the 10-minute range, all of whom can benefit from continuous neural training.
IV. Conclusion: Neuromodulation Will Become One of the Core Technologies for the Future Treatment of Premature Ejaculation
Neuromodulation is no longer confined to high-end operating rooms; it is gradually transitioning “out of the hospital” toward home-based, wearable, and everyday applications. From minimally invasive pulsed radiofrequency surgical devices to non-invasive home training equipment, the treatment of premature ejaculation is entering a new era where science and technology converge.
For men who struggle with long-term medication, are unwilling to tolerate the numbing side effects of sprays, and desire a safe, private, and sustainable approach to delay training, innovative non-invasive physical training products such as Dianjile offer new hope.
References (Excerpt):
[1] Uribe O.L. et al. Transcutaneous Posterior Tibial Nerve Stimulation for PE, 2018
[2] Moussa M. et al. Transcutaneous DPN stimulation, *Asian Journal of Urology*, 2022
[3] Shechter A. et al. TES for PE, *IJIR*, 2019
[4] Chen Si. Study on Low-Frequency Neuromuscular Electrical Stimulation for the Treatment of Premature Ejaculation with Penile Hypersensitivity. Master's Thesis, Anhui Medical University, 2023
[5] Yakov Mirkin. Pulsed RF for PE, *Vestnik Urologii*, 2023