CRISPR Against Cholesterol: Gene Therapy Moves from Rare to Common Diseases
Imagine being able to say goodbye to daily lipid-lowering medication with just a single intravenous injection. With the latest breakthroughs in CRISPR gene-editing technology, this vision is gradually becoming a reality.
On November 8, The New England Journal of Medicine (NEJM) published striking results from a clinical trial: researchers successfully reduced cholesterol levels by approximately 50% in 15 patients with refractory hyperlipidemia using CRISPR-Cas9 gene-editing technology. This isGene editing technology has demonstrated significant potential in the field of cardiovascular disease, a common condition, marking the transition of this “future technology,” once reserved for rare genetic disorders, into mainstream clinical practice.
(Source: NEJM)
Cardiovascular disease is the leading cause of death globally, with high cholesterol being one of its major risk factors. Currently, hundreds of millions of patients rely on lipid-lowering therapies such as statins; however, these medications require daily, lifelong adherence. More critically, up to half of patients discontinue treatment within the first 12 months for various reasons, significantly compromising therapeutic efficacy. If gene editing can achieve a “one-time treatment, lifelong benefit” paradigm, it would fundamentally transform the prevention and management landscape of cardiovascular disease.
"Being able to achieve this would be revolutionary," said Luke Laffin, a preventive cardiology specialist at the Cleveland Clinic in Ohio and the principal investigator of the trial. "Conceptually,This is a brilliant idea: we can shift chronic therapies toward one-time treatments."
The success of this study stems from the inspiration scientists drew from nature.
Researchers have discovered that some individuals naturally carry loss-of-function mutations in the ANGPTL3 gene. ANGPTL3 is a protein primarily produced by the liver, which regulates the levels of fat molecules in the blood by inhibiting lipoprotein lipase and endothelial lipase. Individuals with loss-of-function variants in the ANGPTL3 gene maintain lower cholesterol and triglyceride levels throughout their lives, exhibit a significantly reduced risk of cardiovascular disease, and do not experience any apparent health issues.
This natural experiment has pointed scientists in the right direction:"If the ANGPTL3 gene could be artificially 'switched off,' would it achieve the same lipid-lowering effect?"ANGPTL3 has emerged as an ideal target for gene editing, not only because its expression is nearly exclusive to the liver, facilitating precise therapeutic intervention, but also because it simultaneously modulates two atherogenic lipoproteins: low-density lipoprotein (LDL, or “bad” cholesterol) and triglycerides. Currently, no available drug can significantly reduce both of these parameters concurrently.
To achieve precise gene editing within the human body, two critical challenges must be addressed: how to locate the target gene and how to deliver the “gene scissors” to the correct site.
CTX310, developed by the research team, is precisely such a sophisticated system. At its core lies CRISPR-Cas9 technology, where the Cas9 protein acts as molecular scissors that, guided by guide RNA, can accurately locate and cleave specific sites within the ANGPTL3 gene, thereby disabling its function. To deliver this "toolkit" into hepatocytes, researchers encapsulated messenger RNA encoding Cas9 together with guide RNA within lipid nanoparticles. These nanoparticles serve as miniature "delivery parcels"; after intravenous injection into the bloodstream, they are specifically recognized and taken up by hepatocytes, subsequently releasing the CRISPR components to complete gene editing within the cell nucleus.
Compared with other therapies,The greatest advantage of gene editing is that it offers a one-time, permanent solution.For example, evinacumab, a monoclonal antibody drug that also targets ANGPTL3, has been approved for the treatment of familial hypercholesterolemia but requires regular infusions. In contrast, once gene editing is completed, the edited hepatocytes persist, theoretically providing a permanent lipid-lowering effect.
This Phase 1 clinical trial was conducted at six research centers in Australia, New Zealand, and the United Kingdom, enrolling patients whose lipid levels remained difficult to control despite receiving the maximum tolerated dose of lipid-lowering therapy. The median age of the 15 participants was 53 years; 40% had atherosclerotic cardiovascular disease, and 40% were diagnosed with familial hypercholesterolemia.
The trial employed a dose-escalation design, with doses gradually increased from 0.1 mg/kg to 0.8 mg/kg. The results were encouraging:
Significant Lipid-Lowering Effect:Among the four patients who received the highest dose (0.8 mg/kg), LDL cholesterol levels decreased by an average of 48.9% and triglyceride levels decreased by an average of 55.2% after 60 days.
Target Protein Levels Drop Significantly:The reduction in ANGPTL3 protein levels in the high-dose group reached 73–80%, indicating widespread gene editing in hepatocytes.
Duration of Effect:All subjects completed at least 60 days of follow-up, with sustained lipid-lowering effects, and longer-term follow-up is ongoing.
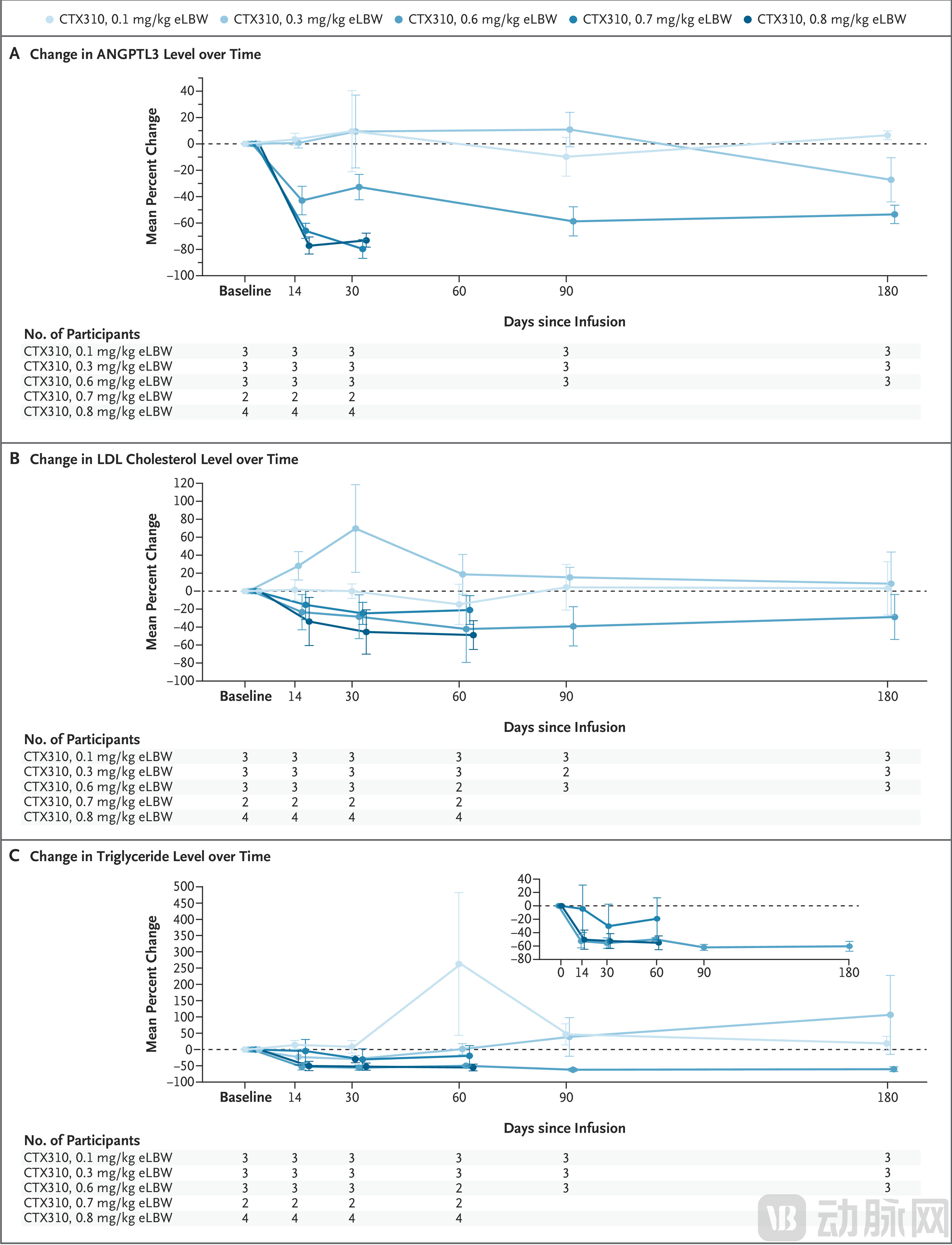
Figure: Changes in ANGPTL3, LDL cholesterol, and triglyceride levels over time after CTX310 treatment (Source: NEJM)
From a safety perspective, the trial results were generally manageable. Three subjects (20%) experienced infusion-related reactions, manifested as back pain and nausea; however, all participants successfully completed the treatment following temporary suspension of the infusion and symptomatic management. One patient with elevated baseline transaminase levels exhibited a transient increase in transaminases (reaching 3–5 times the baseline) after receiving the highest dose, which spontaneously returned to normal within 14 days without other signs of hepatic dysfunction.
It is worth noting that one patient receiving the lowest dose (0.1 mg/kg) died suddenly on Day 179 of the trial. Due to the extended follow-up period and the low dosage, researchers have not yet been able to determine whether this death was treatment-related. This case underscores the critical importance of long-term safety monitoring for irreversible therapies such as gene editing.
More than a decade ago, Kiran Musunuru, a cardiologist at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia, conceived a bold idea:Can the newly emerged CRISPR-Cas9 technology be used to prevent or treat cardiovascular diseases, the world’s leading cause of death??
He enthusiastically pitched the concept to several venture capitalists, but the responses he received were disheartening.“No one is interested at all.”Musunuru recalled. At that time, investors focused solely on rare genetic diseases, believing that although the market for common diseases was large, the technical challenges and regulatory risks were too high.
"Ten years on the east bank, ten years on the west."Nowadays, Musunuru says he knows of aboutA Dozen Companies Are Leveraging Gene-Editing Technology to Tackle High Cholesterol. CRISPR Therapeutics, a biotechnology company based in Zug, Switzerland, which is also the sponsor of this cholesterol trial, has even begun developing therapies forTreatment of Hypertensiongene-editing therapies. Other cardiovascular programs also include the treatment of rarer diseases such as transthyretin amyloidosis.
“This is fertile ground,” said Musunuru, who is also the co-founder of a company pursuing similar therapies.
This shift,Marking the transition of CRISPR technology from rare diseases to common conditions, from the laboratory to clinical practice, and from niche markets to public health. The maturation of technology, the gradual clarification of regulatory pathways, and the early success in treating rare diseases have all paved the way for this transition.
Despite the promising prospects, there remains a long and cautious path from small-scale trials involving 15 participants to truly benefiting millions of patients.
First,Off-Target EffectsIt is the Sword of Damocles hanging over gene editing.
“As the number of treated patients increases, the cumulative probability that you will encounter a patient carrying a specific variant rises, and such variants may lead to novel off-target activities,” said Shengdar Tsai, a gene-editing researcher at St. Jude Children’s Research Hospital in Memphis, Tennessee. The good news is that scientists’ ability to predict how an individual’s genome sequence influences off-target effects is improving.
"We haven’t reached that level yet," said Krishanu Saha, a biomedical engineer at the University of Wisconsin–Madison, "but it appears we are moving in that direction."
Long-Term Safetyis another critical issue. The irreversibility of gene editing is a double-edged sword; while it offers durable therapeutic effects, it also means that any adverse events cannot be “reversed.” Current guidance from the U.S. Food and Drug Administration (FDA) recommends up to 15 years of follow-up for patients receiving in vivo gene editing therapies.
Furthermore, the trial itself has obvious limitations:Sample size of only 15 participants, the limited racial and ethnic diversity of the enrolled population, along with the small number of female participants, restricts the generalizability of the results. Researchers also acknowledge that there is considerable variability in patient responses to the same dosage, which may be associated with hepatic steatosis, inflammatory status, and individual genetic and metabolic characteristics; these factors warrant further investigation.
There is another unavoidable practical issue: cost.The research, development, and manufacturing costs of gene-editing therapies are extremely high, and the final pricing may be prohibitive for most patients. Striking a balance between incentivizing innovation and ensuring accessibility is a challenge that the entire industry must confront.
Faced with these challenges, both researchers and regulatory agencies have opted for a strategy of cautious advancement.
CRISPR Therapeutics'The next step is to expand the scale of clinical trials,However, recruitment will remain strictly limited to patients with extremely high cholesterol or triglyceride levels that cannot be adequately controlled by existing treatments such as statins.
These patients face an extremely high risk of cardiovascular events, for whom the potential benefits of gene editing clearly outweigh the risks. This is particularly true for patients with familial hypercholesterolemia, for whom a one-time gene editing therapy is especially attractive.
As for expanding gene-editing therapies to a broader population, Musunuru stated that it "may take more than a decade."
But Raffin is optimistic about this long-term vision: “The idea is to be able to tell people in their thirties or even twenties, ‘You have a strong family history: everyone in your family had heart attacks in their forties. Can we just give you this treatment so you no longer have to worry?’”
From patients with rare diseases to those with common critical illnesses, and then to high-risk young populations, this is a path that takes decades to traverse. Each step requires large-scale safety studies, rigorous regulatory approval, and continuous technological optimization.
In a sense, the value of this clinical trial,Not only does it demonstrate lipid-lowering efficacy, but more importantly, it represents a paradigm shift.
From the emergence of CRISPR-Cas9 technology in 2012, to the approval of the first CRISPR-based therapy in 2023 for the treatment of sickle cell disease and beta-thalassemia, and now to the ongoing exploration of its application in cardiovascular diseases—a field affecting hundreds of millions of people—gene editing has achieved a leap from proof-of-concept to clinical translation in just over a decade.
Although CTX310 has only taken the first step in a long journey, moving from an initial trial involving 15 patients to truly benefiting millions will require more data, longer follow-up, and more rigorous validation. Nevertheless, this study has already revealed a promising possibility.