FAMILY Trial: A Primary Care-Integrated Fall Prevention Program for Rural-Dwelling Older Adults in China
Falls may seem like a minor issue.But for older adults, a seemingly minor fall can alter the course of their lives—leading to fractures, disability, or even death.
Globally, more than 684,000 people die from falls each year, with over 80% of these fatal incidents occurring in low- and middle-income countries. In China, this issue is particularly severe. With the rapid growth of the elderly population aged 60 and above, now numbering 260 million, the age-standardized fall rate among older adults in China has risen significantly over the past three decades. However, there are very few fall-prevention interventions that can be scaled up and implemented sustainably.
This time, a research team led by Professor Tian Maoyi, Deputy Dean of the School of Public Health at Harbin Medical University, and Professor Wang Yongchen, Academic Leader of General Practice at the Second Affiliated Hospital of Harbin Medical University, in collaboration with multiple provincial Centers for Disease Control and Prevention and medical colleges, has decided to directly address this challenge. They areA Large-Scale Clinical Trial on Fall Prevention Was Conducted in Rural China, and published the research findings in the prestigious international medical journal JAMA (Journal of the American Medical Association) in August 2025.
(Source: JAMA)
The trial, named FAMILY (Fall Prevention for Rural Community-Dwelling Elderly), provides critical evidence for addressing the global challenge of falls associated with population aging. As Professor Tian Maoyi remarked, “Only by integrating scientific evidence into village doctors’ medical kits and embedding it into the daily routines of rural life can fall prevention truly take root and flourish in countless rural households.”
The Severity of Falls Among the Elderly in Rural China Is Often Underestimated.In these regions, medical resources are limited, and health literacy among the elderly is low; most people are unaware that falls are preventable, let alone know how to prevent them.
Currently, China’s National Basic Public Health Service Package does include fall prevention for community-dwelling older adults, but it primarily relies on primary healthcare workers to deliver health education. Although balance and functional exercises are recognized as effective strategies for reducing fall risk, such interventions have not been fully integrated into the existing healthcare system, particularly in resource-limited rural areas.
From September to November 2023, the research team at128 Villages in Heilongjiang, Shanxi, Hubei, and Guangdong ProvincesRecruitment efforts were launched. The selection of these study provinces was carefully considered—they represent diverse geographical locations and varying levels of socioeconomic development across China, thereby enhancing the representativeness of the study findings.
Ultimately, 2,610 adults aged 60 years and older who had experienced at least one fall in the past year or expressed concern about falling participated in this trial. The median age of participants was 70 years, and nearly 60% were female. Notably, 62.1% of participants reported at least one fall in the previous year, 30.1% had sustained injuries from falls, and more than two-thirds expressed moderate to severe concern about falling.
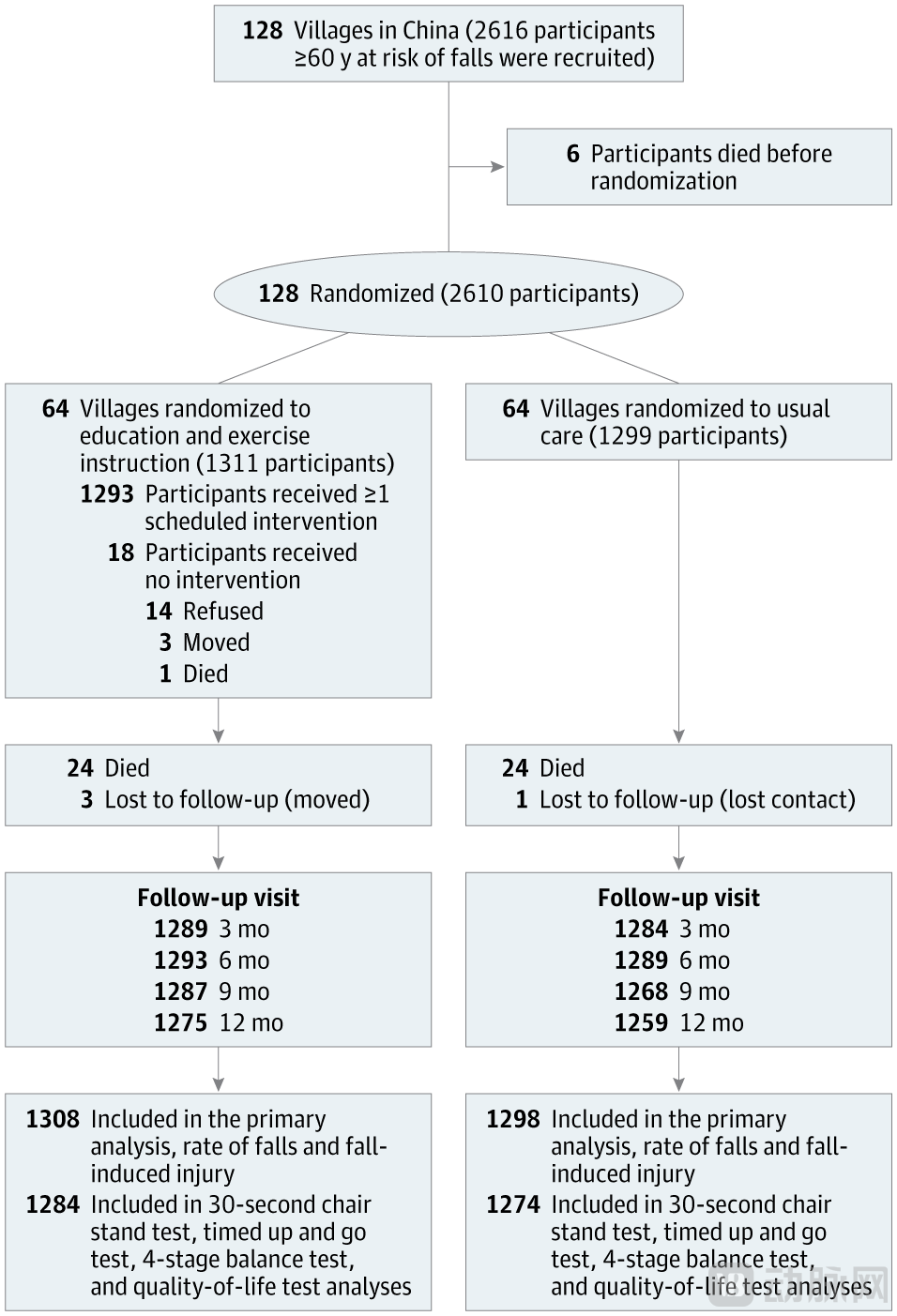
Figure: Flowchart of Participants in the FAMILY Trial (Source: JAMA)
This is a cluster randomized controlled trial, in which researchers randomly assigned entire villages (rather than individuals) to the intervention or control group.A total of 1,311 elderly individuals from 64 villages received fall-prevention interventions, while 1,299 elderly individuals from another 64 villages served as the control group., receiving only routine health education.
The most distinctive feature of this trial is the integration of the intervention into the National Basic Public Health Services Package, with village doctors leading its implementation.
Village doctors are a unique presence in China’s rural primary healthcare system. They typically have either completed three years of technical secondary education or have been practicing continuously in village clinics for more than 20 years, and are licensed by national health authorities to work exclusively at local village clinics.They are not physicians with medical school degrees, yet they are the most accessible and trusted healthcare providers for villagers.
Intervention measures consist of two core components:
1. Balance and Functional Exercises.Drawing inspiration from New Zealand’s renowned Otago Exercise Programme, the research team simplified and adapted it to suit the actual conditions of local older adults. They ultimately designed a set of seven structured exercises: two warm-up exercises, three lower-limb strength exercises, one upper-limb strength exercise, and one balance exercise.
These exercises are delivered through a combination of group sessions and home-based practice. Village doctors organize at least one group exercise session per month (approximately 40 minutes each), while participants are advised to practice independently at home at least four times per week, following pre-recorded videos.
Second, community-engaged health education.Each quarter, village doctors play pre-recorded educational videos during group exercise sessions, covering common risk factors for falls—from biological risks (such as polypharmacy and chronic diseases) to behavioral risks (such as footwear safety) and environmental risks (such as household obstacles).
These videos are thoughtfully designed. All content has been reviewed by experienced geriatricians or orthopedic surgeons,Recorded in the participants' local dialect. What is even more moving is,The video also intersperses real-life stories shared by elderly participants about their involvement in the intervention., fostering an atmosphere of peer support and turning fall prevention into a shared community endeavor.
In contrast, the control group received routine care—according to the standards of the National Basic Public Health Service Package, village doctors provided face-to-face verbal health education once every quarter, covering four aspects: healthy lifestyles, vaccination, osteoporosis prevention, and fall prevention, but without active community engagement.
To record fall incidents, the research team issued a specially designed calendar to each participant—This calendar ingeniously integrates the lunar and solar calendars, closely aligning with the usage habits of elderly people in rural China.At each quarterly follow-up visit, village doctors will remind participants to submit their calendars to the independent outcome assessment team. It is worth emphasizing that village doctors are not involved in any outcome assessments or data collection to ensure the objectivity of the study.
After a mean follow-up of 358 days, the results are encouraging:
The risk of falls is significantly reduced.In the intervention group, 29.7% of participants reported at least one fall during the 12-month follow-up period, compared with 38.3% in the control group. This indicates a 33% reduction in the risk of falls among older adults who received the intervention.
Reduced Fall Frequency and Injuries.The fall rate in the intervention group was 0.8 per person-year, compared with 1.4 in the control group; the proportion of participants reporting fall-related injuries was 15.2% in the intervention group versus 21.6% in the control group, representing a 35% reduction.
Improved functional mobility.The study employed three standardized tests to assess functional mobility. Although the 30-second chair stand test (assessing lower limb strength) and the Timed Up and Go test (assessing overall functional mobility) showed statistically significant differences, they did not reach the threshold for clinically meaningful improvement. In contrast, the Four-Stage Balance Test (assessing balance ability) demonstrated a significant improvement, with 33.7% of participants in the intervention group completing all four stages, compared to only 26.5% in the control group.
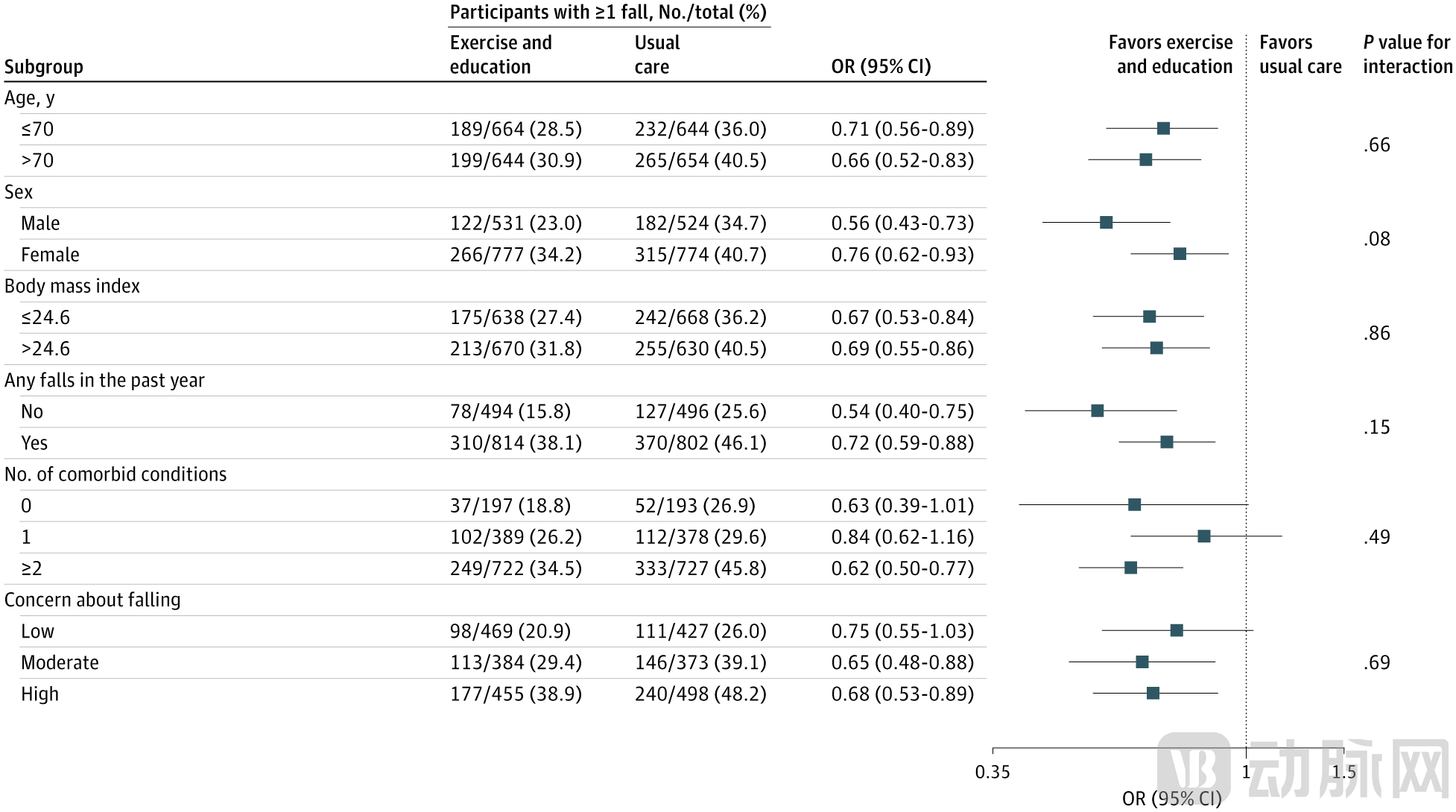
Figure: Effects of Exercise and Education on Fall Prevention Across Subgroups (Source: JAMA)
Improved Quality of Life.Health-related quality of life, measured using the EQ-5D-5L instrument, yielded a score of 0.89 in the intervention group and 0.85 in the control group, with an improvement magnitude that reached the minimal clinically important difference (0.03).
What is even more gratifying is that,The intervention group demonstrated an adherence rate of over 80% to the monthly group exercise sessions.——This represents a remarkably high level, quite rare in studies of behavioral interventions requiring long-term adherence.
In its coverage of this study, Nature noted that the intervention trial’s success was likely attributable to improvements in participants’ lower-limb muscle strength and balance, as evidenced by results from the 30-second sit-to-stand test and the four-stage balance test.
Improvements in muscle strength and balance are key to preventing falls.Both the World Health Organization’s (WHO) “Steady On Your Feet” technical package and the U.S. Preventive Services Task Force (USPSTF) strongly recommend exercise interventions as an effective strategy for preventing falls among community-dwelling older adults. The USPSTF considers exercise interventions to have a moderate net benefit, while the WHO gives a strong recommendation for gait, balance, and functional training.
The seven exercises in the FAMILY trial are a simplified version of the Otago Exercise Program. This simplification was designed to better accommodate the reality of lower educational attainment and health literacy among rural populations. Notably, more than half of the participants already engaged in some level of physical activity at baseline; nevertheless, this targeted fall-prevention exercise program still significantly reduced their risk of falling, demonstrating that specialized balance and functional training indeed offers unique value.
Integration into the Existing Healthcare System
The European Geriatric Medicine Society recently issued a call to action, emphasizing that effective fall prevention strategies must be integrated into broader healthcare systems. The FAMILY trial does precisely this. Rather than creating a “laboratory-style” intervention separate from existing systems, it embeds fall prevention measures within the national basic public health service package, implemented by village doctors already working in rural communities. This design is grounded in prior research findings—multiple studies have demonstrated that village doctors can play a significant role in the prevention and management of non-communicable diseases without relying on the limited and heavily demanded resources of specialist physicians.
Although there are many successful cases worldwide (including in low- and middle-income countries) of mobilizing village-level healthcare workers to assume public health responsibilities, the FAMILY trial uniquely demonstrates the potential for preventing falls among older adults in resource-limited settings.
Cultural Adaptability and Community Engagement
Village doctors, serving as trusted cultural intermediaries, played a pivotal role in this trial. They bridged the formal healthcare system and rural populations, developing interventions tailored to the local cultural context. More importantly, they fostered sustained participant engagement not merely by providing services, but by cultivating interpersonal trust.
The storytelling approach (delivered in local dialects) used in health education transforms fall prevention into community-driven action, fosters a sense of collective responsibility, and enhances mutual support within the community through shared experiences, thereby improving adherence. This cultural adaptability is reflected in numerous details: the use of calendars combining the solar and lunar systems, videos in local dialects, and peer-shared stories. These seemingly minor design elements are, in fact, key to narrowing health literacy gaps and strengthening stakeholder engagement and accountability.
Scalable and Sustainable
The successful implementation of this trial also depended on several factors: strong collaborative partnerships with multiple institutions, adequate staffing of researchers, and robust training, which ensured the successful recruitment of participants and implementation of the intervention within three months. Furthermore, shared community responsibilities—such as leveraging the cultural competence of village doctors and using culturally appropriate calendars—were key to the successful implementation of the program.
Such socioculturally appropriate community engagement activities bridge health literacy gaps, promote stakeholder participation and accountability, and enhance adherence to interventions.and makes it possible to promote community-engaged interventions within the primary healthcare system—This remains a significant gap in most low- and middle-income countries.
Both the research team and Nature’s reviewers candidly acknowledged certain limitations of this study:
First, although a cluster randomized design was adopted, the study could not completely rule out residual confounding from unmeasured factors. Nevertheless, the well-balanced baseline characteristics between the two groups indicate that randomization was robust.
Secondly, the observed baseline prevalence of falls was higher than hypothesized. This can be attributed to the lack of large-scale, representative fall data in China and variations among different target populations.
Third, although the study implemented various measures to minimize bias (such as using culturally appropriate fall calendars, regular reminders from village doctors, and an independent data collection team), self-reported outcomes by participants may still underestimate the incidence of falls. A commentary in Nature pointed out that collecting calendars every three months could introduce recall bias. Furthermore, both participants and the village doctors delivering the interventions were aware of which intervention was assigned, which may have influenced the results (performance bias).
Fourth, caution is warranted when applying these findings in settings without village doctors or similar healthcare workers, such as nursing homes or hospitals, given that the intervention was delivered by village doctors.
Fifth, the study was unable to distinguish the individual effects of each intervention component (exercise or health education). However, improvements in lower limb muscle strength and balance suggest that balance and functional exercises may be the most effective components of the intervention.
Finally, the Nature commentators also pointed out that the study did not use the Template for Intervention Description and Replication (TIDieR) checklist to report intervention components, nor did it provide detailed information on intervention fidelity, class attendance, exercise dosage, and progression. Furthermore, the lack of significant improvement in the Timed Up and Go test may indicate that the intensity or progression of the exercise was insufficient to enhance overall functional mobility. The study also failed to describe how harms and their severity were measured.
Despite these limitations, the overall model of the FAMILY trial—a low-cost education-plus-exercise intervention—is easy to implement in resource-limited settings and in low- and middle-income countries.
Reviewers at Nature emphasized that the significance of this clinical trial lies not only in its scientific rigor—adhering to CONSORT standards, employing a cluster design, and featuring a large sample size—but also in itsAddressing a Major Global Health Burden. The FAMILY trial integrates simple adjustments into existing care, rather than introducing entirely new treatment pathways,It demonstrates that evidence-based medicine can provide accessible, affordable, and acceptable services to people in rural areas.
Integrating such models into the healthcare system could transform preventive care and optimize healthy aging for older adults. As recognized by the WHO,Strengthening Primary Healthcare Is Key to Achieving Universal Health Coverage,including fall prevention—especially in countries with rapidly aging populations, limited medical resources, and inadequate accessibility to healthcare services.
The FAMILY trial provides evidence for adaptable and scalable fall prevention strategies in China and other low- and middle-income countries facing rapid population aging and constrained healthcare resources. It supports recommendations for exercise-based fall prevention measures and highlights the potential for implementing such programs in these settings.
This study, published in JAMA,More than just an academic paper, it is a practical response to the global challenge of aging.It tells us:Even in the most resource-constrained rural areas, we can bring about tangible improvements to the health and safety of older adults by integrating existing healthcare systems, mobilizing grassroots healthcare workers, and adopting culturally appropriate, simple interventions.
For China’s 260 million elderly population, and for the many other countries worldwide facing similar challenges, the FAMILY trial has lit a beacon of hope—preventing falls is not only possible but also feasible.