China's Domestic Developers Lag Behind as $450 RSV 'Vaccine' Sparks Long Queues Nationwide

AstraZeneca
Pharmaceutical Technology Research and Development Provider
This year’s respiratory syncytial virus (RSV) season appears to be unusually prolonged, lasting from midsummer through the depths of winter.
Unlike in the past, when young children could only be protected through physical isolation, parents now have an additional option this year: administering a trendy vaccine priced at over 3,000 yuan per dose to reduce the risk of severe illness caused by RSV infection. However, this has also brought heightened anxiety. Despite its high cost, the vaccine is difficult to access. Currently, only a few community hospitals and private pediatric hospitals in China stock the vaccine, and appointments are typically required, with waiting times often exceeding one month.
This widely discussed “viral” vaccine is, in fact, nirsevimab, developed by Sanofi. Nirsevimab is essentially a direct monoclonal antibody therapy, rather than a traditional vaccine that requires activation of the body’s own immune system to combat viruses. It takes effect immediately upon administration and has minimal side effects. Nirsevimab was approved in China in late 2023. During the previous RSV season, its use was piloted primarily in several children’s hospitals in Shanghai. As RSV infections surged this year, nirsevimab coverage expanded to primary care vaccination sites in Beijing, Tianjin, Hubei, and other regions, sparking a wave of vaccinations.
Prior to this, nirsevimab had already generated billions of dollars in revenue across Europe and the United States. The originator, Sanofi, even stated that the drug’s market launch created an unprecedented situation of supply falling short of demand.
The Blockbuster Drug in Short Supply
Currently, RSV has become the leading cause of severe lower respiratory tract infections in infants and young children. Most children will contract RSV at least once before their first birthday; however, if infection occurs at a younger age, it can lead to severe conditions such as pneumonia and bronchiolitis, necessitating hospitalization. Data show that the hospitalization rate for infants aged three months and younger with RSV infection can reach 10%–20%, making this patient population one of the primary groups admitted to pediatric intensive care units during the winter and spring seasons each year.
At this stage,Prophylactic medications for RSV infection include vaccines and preventive monoclonal antibodies.Among them, RSV vaccines are represented by the well-known Arexvy and Abrysvo. However, RSV vaccines are primarily indicated for adults, while prevention in infants and young children relies mainly on prophylactic monoclonal antibodies. For more than two decades prior to the launch of nirsevimab, this field was long dominated by an older monoclonal antibody product, yet the overall effectiveness in prevention and control remained suboptimal.
In 1998, palivizumab, developed by MedImmune, was approved for marketing in the United States, becoming the world’s first prophylactic monoclonal antibody for the prevention of severe lower respiratory tract infections caused by RSV infection.However, the limitations of palivizumab are also evident, namely its narrow scope of indication. As required, palivizumab is indicated only for preterm infants younger than 6 months of age at the onset of the RSV season, or for children under 2 years of age with specific conditions such as bronchopulmonary dysplasia or congenital heart disease.In other words, palivizumab is not suitable for most infants and young children.
Even so, palivizumab rapidly gained market traction after its launch, generating substantial commercial value for MedImmune. In 2007, AstraZeneca acquired MedImmune for the hefty sum of $15 billion. Following its integration into AstraZeneca’s portfolio, sales of palivizumab soared. In 2008, palivizumab’s sales exceeded $1.2 billion, climbing to $1.35 billion the following year and earning it blockbuster drug status. Even in 2024, when faced with competition from the newly launched nirsevimab, palivizumab still achieved sales of $501 million. This underscores the strong market appeal of monoclonal antibodies for RSV prophylaxis.
Compared with palivizumab, the most significant advantage of nirsevimab is its applicability to healthy infants and young children. As indicated, nirsevimab can be used for neonates and infants entering or born during their first RSV season, including healthy infants and young children, as well as the population previously covered by palivizumab.
In 2022 and 2023, nirsevimab was successively approved in the European Union and the United States, and was launched in these markets just in time for the 2023 RSV season, instantly igniting market demand.According to news reports from that year, nirsevimab experienced high demand and supply shortages in multiple markets where it was launched.

Taking the U.S. market as an example, the U.S. Centers for Disease Control and Prevention (CDC) issued a specific health alert at that time, stating that the supply of nirsevimab was limited. It required healthcare institutions to adjust medication prioritization by stipulating that the 100 mg dose should be prioritized for infants under 6 months of age and high-risk infants with underlying conditions. Furthermore, it strictly prohibited administering two 50 mg doses to infants weighing 5 kg or more, thereby conserving medication for lower-weight infants. The CDC even suspended the use of nirsevimab in children aged 8–19 months who were eligible for palivizumab prophylaxis.
However, the market gap for nirsevimab remains substantial. During the 2024 RSV season, approximately 2.4 million infants in the United States were eligible for the medication, leading to a massive influx of patients into healthcare facilities and frequent shortages at clinics and hospitals. In fact, even before its launch, Sanofi had devised a supply plan for nirsevimab that far exceeded the scale of previous pediatric immunotherapeutic product launches, yet actual demand still significantly surpassed expectations.
According to the financial reports released by Sanofi, nirsevimab generated sales revenue of approximately $598 million in 2023. In 2024, amid a surge in demand, global sales of nirsevimab reached $1.829 billion. Within just two years of its launch, nirsevimab has joined the ranks of blockbuster drugs. In 2025, Sanofi prioritized expanding nirsevimab into markets outside Europe and the United States, making it the company’s primary driver of performance growth. Financial statements show that in the first three quarters of 2025, nirsevimab achieved sales of approximately $860 million, representing a year-on-year increase of 19.8%, and was the only product within Sanofi’s vaccine division to register positive growth. Notably, markets outside Europe and the United States witnessed explosive growth of 526.7%.
Sustained Surge in Demand
During the 2025 RSV season, the supply of nirsevimab remained tight.
This time, Sanofi prepared in advance by tripling the production capacity of nirsevimab compared to its initial launch volume and establishing numerous additional manufacturing sites. In early Q3 2025, Sanofi proactively initiated global distribution of nirsevimab, allocating a number of doses equivalent to the total annual supply in 2024. However, based on the current situation of vaccination queues in China, the increased supply of nirsevimab still falls short of meeting the substantial demand driven by the global outbreak.
Notably, the scarcity of nirsevimab stems from a surge in global demand for RSV prevention among infants and young children. Beyond nirsevimab, this demand is also causing shortages of other drugs in the same class.
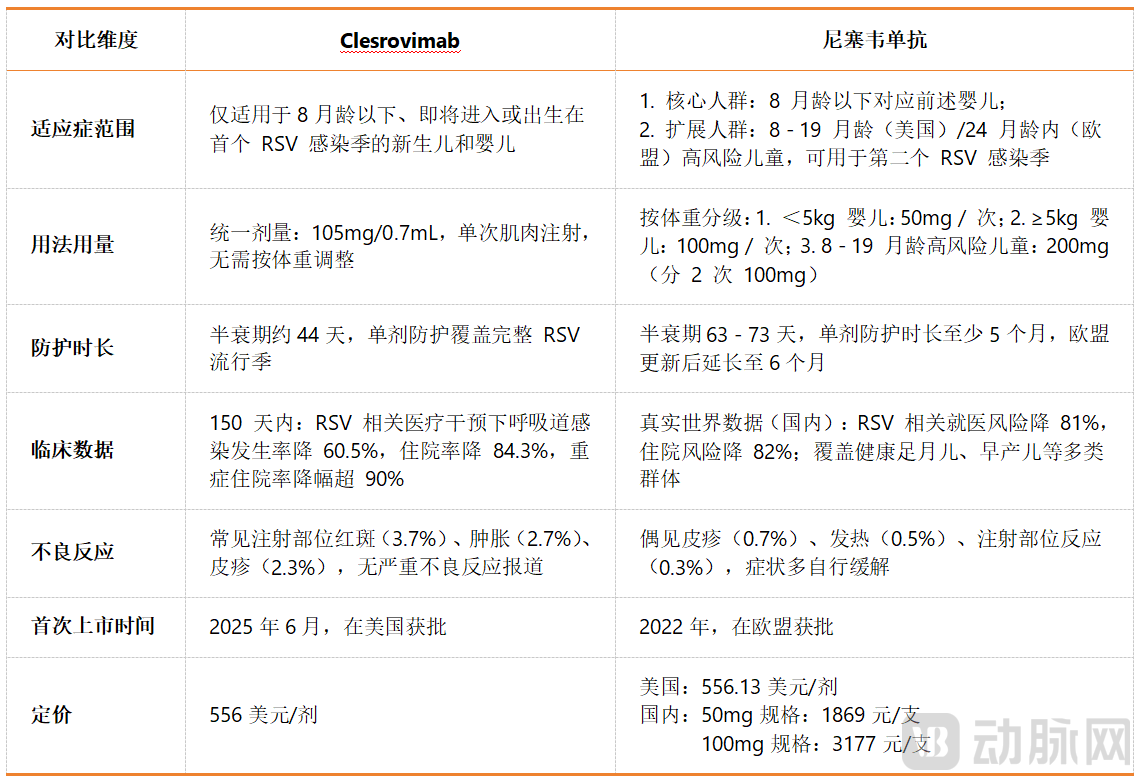
On one hand, the new RSV preventive monoclonal antibody became an instant bestseller upon its market launch.In June 2025, another monoclonal antibody for the prevention of RSV infection in infants and young children, Clesrovimab, was approved for marketing in the United States. Developed by Merck & Co., Clesrovimab is also indicated for the prevention of lower respiratory tract disease caused by respiratory syncytial virus (RSV) in neonates and infants born during or entering their first RSV season. During the 2025 RSV epidemic season, high expectations were placed on the newly launched Clesrovimab.
Based on publicly available information, the two currently marketed RSV prophylactic monoclonal antibodies are highly similar in terms of indications, dosage and administration, target market, and clinical data. The primary difference lies in the fact that, following an expansion of its indications, nirsevimab can be used in children aged 8 to 19 months to protect against infection during their second RSV season. In the European Union, the upper age limit for this population has been extended to 2 years of age. Furthermore, unlike nirsevimab, which requires selection of different syringe specifications based on infant weight, clesrovimab is administered via intramuscular injection at a uniform dose regardless of infant weight. Regarding clinical trial data, clesrovimab demonstrates slightly superior protective efficacy compared to nirsevimab, whereas the latter exhibits a significantly lower incidence of adverse reactions.
Reportedly, Merck & Co., the originator of clesrovimab, has already felt market pressure. The company began accepting orders for clesrovimab the month after its approval and initiated shipments before the start of the 2025 RSV season. Currently, although Merck is officially maintaining normal ordering channels for clesrovimab, it has imposed supply restrictions. For instance, in accordance with the requirements of the U.S. Vaccines for Children (VFC) program, healthcare institutions ordering clesrovimab for the 2025 RSV season may be required to simultaneously order nirsevimab to alleviate supply pressures.
On the other hand, the former star RSV vaccine has overtaken its competitors by securing indications for infants and young children.In May 2023, Arexvy, developed by GSK, and Abrysvo, developed by Pfizer, were successively approved for marketing in the United States, causing a significant stir. As the only two RSV vaccines globally targeted at the elderly population, Arexvy and Abrysvo have filled a long-standing clinical gap.
GSK and Pfizer subsequently entered the fray in the RSV vaccine market. In its first year on the market, Arexvy leveraged its first-mover advantage as “the world’s first RSV vaccine” to generate $1.543 billion in sales, far outpacing Abrysvo’s performance during the same period. However, the growth momentum of both Arexvy and Abrysvo came to an abrupt halt in the second year. In June 2024, the U.S. Centers for Disease Control and Prevention (CDC) updated its RSV vaccination guidelines, recommending a single dose of RSV vaccine for all adults aged 75 years and older, as well as for high-risk individuals aged 60–74 years. This change significantly reduced the eligible population for both Arexvy and Abrysvo.
As a result, sales of both Arexvy and Abrysvo declined sharply in 2024. In particular, Arexvy’s sales dropped by more than half. The downward trend for these two blockbuster vaccines continued into 2025. However, a turning point emerged in the second quarter of 2025, when their sales trajectories diverged. The underlying reason was that in August 2024, Abrysvo received approval for use in pregnant women at 32–36 weeks of gestation to protect newborns from RSV infection. As Abrysvo expanded its reach to include the infant population, it immediately regained strong market demand. In the second quarter of 2025, Abrysvo’s sales surged by 155% year over year, thereby surpassing Arexvy.
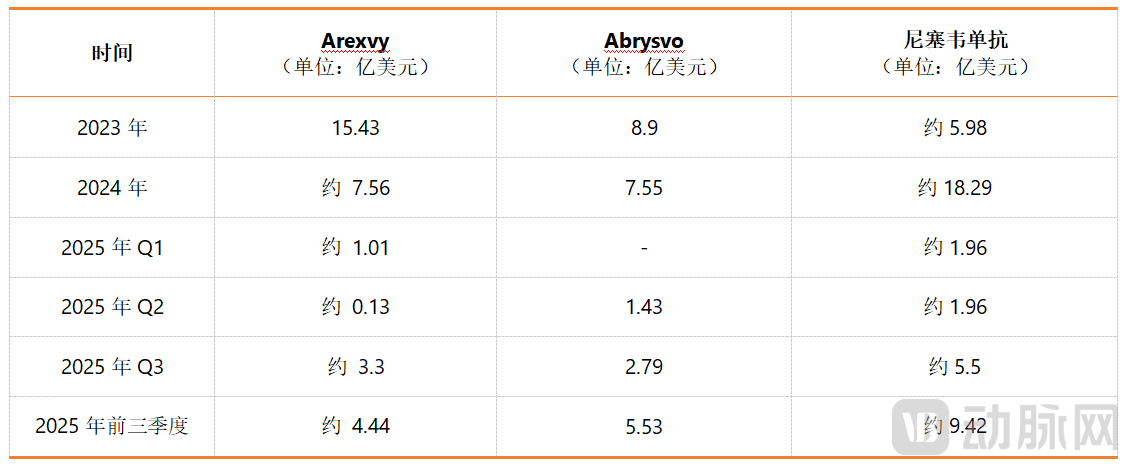
A comparison of the sales performance of Arexvy, Abrysvo, and nirsevimab makes the conclusion even clearer. These three drugs have similar launch timelines and indications, differing primarily in their target populations. Arexvy and Abrysvo, indicated for adults, initially generated greater commercial value but faced higher uncertainty, leading to a sharp decline amid policy fluctuations. In contrast, nirsevimab, indicated for infants and young children, has demonstrated stable performance. In the second quarter of 2025, Abrysvo also showed strong growth momentum after expanding its indication to include infants.
When will Chinese-made products follow suit?
Turning our attention back to the domestic market, despite promising sales prospects, the development of preventive monoclonal antibodies against respiratory syncytial virus (RSV) for infants and young children remains a niche sector in China. A search by VCBeat reveals that there are currently only four such candidates under development in China. Among them, TNM-001 from Tynovabio and RB0026 from Ruiyang Biologics are progressing more rapidly, with both having entered Phase III clinical trials.

Among these, TaiNuMab’s TNM-001 is the RSV preventive monoclonal antibody with the most advanced development progress in China. It was previously positioned as the third globally and the first domestically available long-acting monoclonal antibody indicated for both healthy and high-risk infants and young children. Phase IIb clinical trial results demonstrated that TNM-001 achieved 66.2% efficacy in preventing RSV lower respiratory tract infections requiring medical attention, and 82.3% efficacy in preventing related infections requiring hospitalization. These figures are closely comparable to those of Merck’s Clesrovimab, and even superior in terms of reducing the risk of hospitalization. Currently, TNM-001 has completed the collection of key data from its Phase III clinical trials.It is expected to hit the market as early as the 2027 RSV season.
Another long-acting monoclonal antibody against RSV, Rayno Biopharma’s RB0026, is currently undergoing Phase III clinical trials at approximately 60 centers across China, with the aim of securing market approval before the 2027 RSV season. Notably, to ensure post-launch supply, Rayno Biopharma plans to invest a total of RMB 785 million in building a production line with an annual capacity of 1.6 million doses, which is expected to commence operations in March 2026.
In other words, domestically produced RSV prophylactic monoclonal antibodies will not enter the market until at least the RSV epidemic season two years from now.The underlying reason is that,On one hand, the development of RSV-preventive monoclonal antibodies suitable for infants and young children is challenging and time-consuming.Due to the poor stability of the prefusion conformation of the RSV F protein targeted by prophylactic monoclonal antibodies against RSV, along with the significant challenges in manufacturing processes, the failure rate for developing such drugs is extremely high. Furthermore, selecting infants and young children as the target indication adds considerable complexity to clinical trial enrollment, safety and dose-finding studies, and endpoint design. The development of prophylactic monoclonal antibodies against RSV is by no means an easy path.
On the other hand, the development of RSV prophylactic monoclonal antibodies has seen relatively low interest in the primary market.The development of RSV prophylactic monoclonal antibodies is challenging, and their post-launch application potential is limited compared to RSV vaccines, resulting in a lower cost-effectiveness ratio. Consequently, substantial capital and resources have been directed toward RSV vaccines and small-molecule drugs. According to the VCBeat Orange Database, there are more than 10 RSV vaccine candidates under development in China. Among them, MicuRx Pharmaceuticals’ recombinant RSV vaccine has made the fastest clinical progress, having entered Phase III clinical trials. Other candidates, including Adagene’s ADC110, Afanabio’s mRNA RSV vaccine, and SinoCellTech’s SCT630, are currently in Phase II clinical trials. However, with the exception of Adagene’s ADC110, which targets children aged 6 months to 5 years, the pipeline is still predominantly focused on adult vaccines.
Long queues form for trendy vaccines priced at over 3,000 yuan per dose, yet few domestic developers are following suit, highlighting the supply-demand mismatch in niche pharmaceutical development. Balancing the feasibility analysis of new drug development with a thorough consideration of actual clinical needs undoubtedly tests the ingenuity of development teams.