China Launches First National Multi-Center Bone Mineral Density Database Tailored for Chinese Population, Aligning with Global Standards from Europe, the US, Japan, and Korea
On a bone mineral density report, the most prominent feature is always the T-score—indicating normal bone density, osteopenia, or osteoporosis. This value directly determines whether a patient requires intervention or pharmacological treatment, and even dictates the assessed level of fracture risk.
But few people ask: Who exactly is this T-value being compared against?
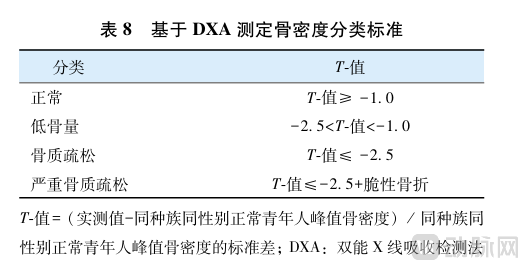
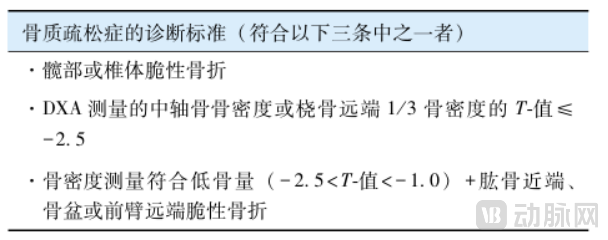
The “who” being compared is the true “invisible referee” in the field of bone mineral density testing—the reference database. According to the Guidelines for the Diagnosis and Treatment of Primary Osteoporosis (2022 Edition), the diagnostic criteria for osteoporosis in postmenopausal women and men aged 50 years and older are clearly based on T-scores: a T-score ≥ -1.0 is normal, -2.5 < T-score < -1.0 indicates osteopenia, and a T-score ≤ -2.5 indicates osteoporosis. The calculation of the T-score relies entirely on the reference database—No Database, No T-Score; No Accurate Database, No Credible T-Score。
Excerpt from the Guidelines for the Diagnosis and Treatment of Primary Osteoporosis (2022 Edition)
01
What Is a Database? The “Gold Standard” for Bone Mineral Density Testing
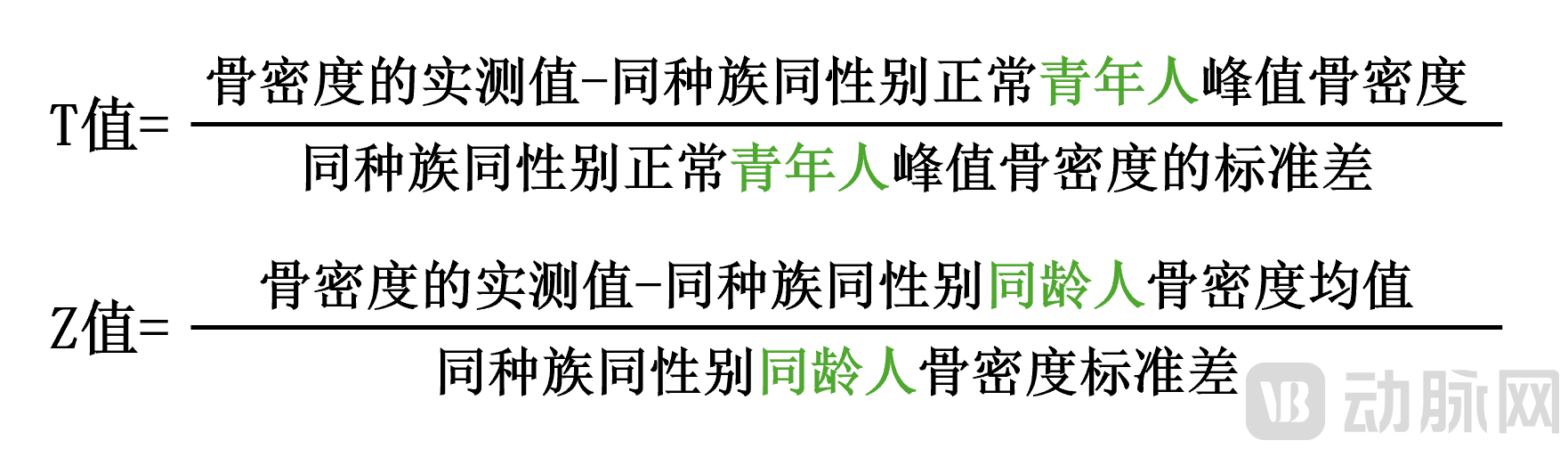
The essence of bone mineral density (BMD) testing is a comparison. Whether your BMD is high or low requires a reference frame. This reference frame is a database composed of BMD measurements from a large population of healthy individuals. Through these data, medicine can map the normal trajectory of skeletal changes with age and calculate the T-scores and Z-scores used in clinical practice.
The 2022 guidelines explicitly state that bone mineral density (BMD) measurement is the gold standard for diagnosing osteoporosis, and BMD values obtained via dual-energy X-ray absorptiometry (DXA) must be compared with reference databases of healthy individuals matched by ethnicity, sex, and age. This definition inherently implies a key premise: the accuracy of the reference database directly determines the accuracy of the diagnosis.
02
Building a Qualified Database: Three Levels of Scrutiny and National Standards
A database that can truly guide clinical practice is by no means a simple aggregation of population data. According to relevant studies, a qualified reference database must undergo three rigorous screening criteria:
■ Stage 1: Population Representativeness
Skeletal development is closely related to genetic background, living environment, and dietary habits. There are significant differences in the normal values of bone mineral density among people of different races and regions. An important review published in "Skeletal Radiology" in 2024 clearly pointed out:Using bone mineral density reference databases from European and American populations to calculate T-scores for East Asian populations leads to systematically lower results, thereby overestimating the prevalence of osteoporosis.
This study further demonstrates that multiple databases are currently used concurrently across East Asia, including in mainland China, Taiwan, Japan, South Korea, and Singapore.AsianDatabaseorU.S. and European NHANES III Database. This lack of standardization directly affects the accuracy and comparability of diagnoses.
The NHANES III database, fully named the “NHANES III Reference Database,” is a bone mineral density reference database established during Phase III of the National Health and Nutrition Examination Survey (NHANES). Constructed primarily from data on healthy non-Hispanic white individuals in the United States, this database has long served as a reference standard for the diagnosis of osteoporosis in many countries worldwide. However, this practice has fundamental limitations:The NHANES III database reflects the patterns of skeletal development and peak bone mass levels among Caucasian populations in Europe and America. However, significant differences exist across ethnic groups in terms of normal bone mineral density (BMD) values and rates of bone loss. Applying the NHANES III database to East Asian populations is akin to using a “standard ruler” derived from European and American skeletons to measure Chinese individuals. Since Caucasian populations generally exhibit higher peak bone mass and a wider range of normal BMD values, this approach systematically lowers T-scores in East Asian populations, thereby overestimating the prevalence of osteoporosis.This is precisely the fundamental reason why the academic community has called for the establishment of race-specific reference databases.
Based on robust epidemiological evidence, the research team strongly advocates that race- and sex-specific bone mineral density reference databases must be used for the diagnosis of osteoporosis in Asian populations.
■ Level 2: Data Purity
Individuals included in the database must undergo rigorous screening—excluding those with any conditions that may affect bone metabolism (such as hyperparathyroidism, chronic kidney disease, and diabetes), those on long-term use of medications affecting bone metabolism (such as glucocorticoids and anticoagulants), and those with a history of fractures. Meanwhile, the measurement process must be subject to strict quality control to eliminate interference from motion artifacts and measurement errors.
The 2022 edition of the guidelines, when elaborating on bone mineral density measurement techniques, particularly emphasized the importance of quality control, pointing out that measurement personnel must undergo rigorous training, equipment must be calibrated daily, and the measurement process must adhere to standardized operating procedures. These quality control requirements also apply to the database construction process—Only by ensuring that each data point truly represents the physiological status of “healthy individuals” can the database hold clinical reference value.
■ Stage 3: Sample Size and Device Consistency
The sample size must be sufficiently large to minimize random error and ensure statistical stability. If multi-center data collection is involved, the models, calibration, and operating procedures of all equipment must be highly standardized to ensure data comparability and poolability.
Professor Cheng Xiaoguang of Beijing Jishuitan Hospital once led a team to conduct a nationwide, multicenter DXA bone mineral density study, providing strong supporting evidence. The study fully demonstrated that in multicenter studies,Standardizing device brands, unifying quality control standards, and harmonizing data calibration are fundamental prerequisites for ensuring data comparability and statistical stability.If device models differ and calibration standards vary, even extensive data collection cannot achieve effective integration; indeed, the confounding of systematic errors may lead to erroneous epidemiological conclusions.
03
The Clinical Cost of Using the Wrong Database: An In-Depth Analysis Based on Guidelines and Evidence-Based Medicine
What are the consequences of using a mismatched reference database? The 2022 guidelines explicitly state that the diagnosis of osteoporosis is based on bone mineral density (BMD) measurements, and the T-score reference database used in the diagnostic criteria directly affects prevalence statistics and individual diagnostic classification. Numerous studies have confirmed the clinical significance of this issue. Due to the long-standing lack of nationwide epidemiological studies on osteoporosis prevalence in China and the absence of diagnostic benchmarks tailored to the skeletal characteristics of the Chinese population, standardized diagnosis and treatment of osteoporosis in China face significant challenges. At the core of this issue is the appropriateness of the reference database.
Excerpted from the "Guidelines for the Diagnosis and Treatment of Primary Osteoporosis (2022 Edition)"
In the article “Addressing Differences in Lumbar Spine and Proximal Femur Bone Mineral Density Measurements Across Different DXA Manufacturers: Analysis of Measurement Data from a National Epidemiological Survey Population Using Hologic and GE-Lunar DXA,” Professor Yu Wei of Peking Union Medical College Hospital clearly stated:Bone densitometers manufactured by different vendors incorporate distinct reference databases, leading to systematic discrepancies in results even when measuring the same population.Significant discrepancies in measurement results exist between the two mainstream devices, Hologic and GE-Lunar, when using their respective manufacturer-specific databases. This leads to frequent occurrences of "false-negative" or "false-positive" diagnoses of osteoporosis, severely compromising the consistency of clinical diagnosis and the accuracy of fracture risk assessment.This study further corroborates the critical importance of establishing unified reference standards and developing bone mineral density databases tailored to the Chinese population for enhancing diagnostic homogeneity. International academic attention to this issue continues to intensify.
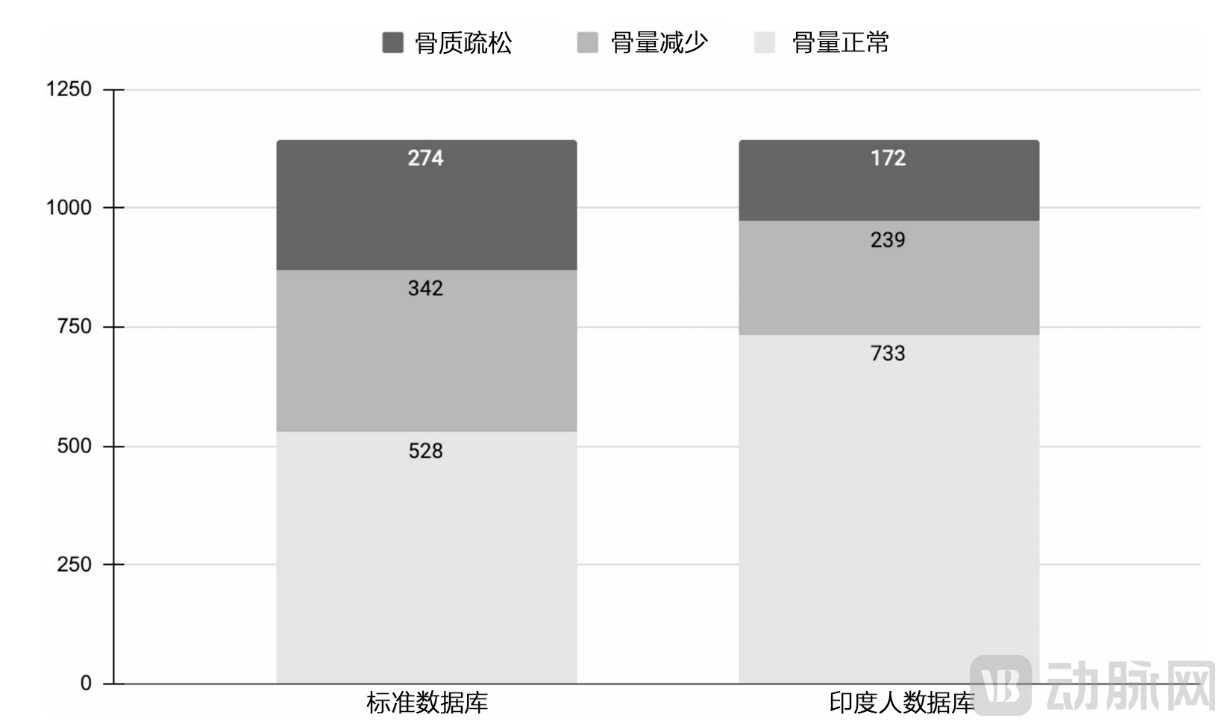
A review published in Skeletal Radiology in 2024 systematically examined the consequences of applying Western databases to East Asian populations: using bone mineral density reference data from Western populations to assess East Asians leads to systematically lower T-scores, thereby overestimating the prevalence of osteoporosis. Similar findings have been validated in Indian populations—a study published in BMC Musculoskeletal Disorders in 2025 showed thatAfter using an India-specific reference database, the prevalence of osteoporosis decreased from 16.8% to 7.1% in men and from 26.6% to 18.0% in women.
Excerpted from “Estimation of T scores with Hologic using Native vs. Caucasian data in Indians (ETHNICA): a single-center retrospective study.” Specifically, this systematic bias leads to:
Risk of False Positives:Misclassifying healthy individuals as having osteopenia or osteoporosis leads to unnecessary examinations, treatments, and psychological burden.
Risk of False Negatives:Missing Patients Who Truly Require Intervention, Missing the Window for Prevention and Treatment
Distorted Epidemiological Data: Prevalence Rates Based on Flawed Criteria Fail to Accurately Reflect Disease Burden
The 2022 edition of the guidelines places particular emphasis in the “Diagnosis and Treatment Algorithm for Osteoporosis” that accurate bone mineral density (BMD) measurement is a prerequisite for diagnosis, and such accuracy relies on reliable reference standards. If the “ruler” itself is inaccurate, all subsequent diagnostic and therapeutic decisions will be based on erroneous foundations.
04
National Mission: The Birth and Strategic Significance of the Reference Database for Bone Mineral Density in the Chinese Population
It is precisely in recognition of the urgency of this issue that a national-level research task has been officially launched.
Innary Medical, as a participating enterprise in the National Major Science and Technology Special Project,Jointly applied for the National Major Project on the "Four Major Chronic Diseases" in collaboration with institutions of varying tiers, including the Sixth People's Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, the Shanghai Institute of Nutrition and Health of the Chinese Academy of Sciences, and the Second Xiangya Hospital of Central South University.Establish the Development of a Bone Mineral Density Reference Database for the Chinese Population as a National Health Strategic Initiative.With the successful installation of China’s first dual-photon platform bone densitometer (DXA) at Shanghai Jiao Tong University School of Medicine Affiliated Sixth People’s Hospital, the database construction project has officially been launched.A five-year plan is in place to collect bone mineral density data from 100,000 healthy individuals, while actively integrating existing large-scale natural population cohort studies (e.g., the “Kunshan Bone Health Ten-Year Protection Program Study”)., to establish a gold standard for the diagnosis of osteoporosis in Chinese people based on X-ray bone densitometry, aiming to end the current reliance on standards derived from other ethnic groups.INNO S “Zhenxing” and INNO E “Fuxing” from Innary Medical are the first to translate the achievements of the National Major Science and Technology Projects into clinical tools, establishing China’s own “national team” standard for bone health assessment.

Key Elements of Study Design:
Geographic Coverage: Starting with the Yangtze River Delta, radiating nationwide, and covering major regions across China
Age Range: Sampling across all age groups to ensure sufficient sample sizes for each age bracket
Gender Balance: Construct Sex-Specific Reference Curves for Males and Females Separately
Strict Quality Control: Uniform Equipment Models, Unified Calibration Standards, Standardized Operating Procedures, and Consistent Exclusion Criteria
Sample Size: 100,000 valid health population data points to ensure statistical stability
Data Integration: Integrating genomic phenotypic analysis with clinical diagnosis and treatment data to provide a scientific basis for disease prediction.
Ensuring the Purity of Data Collection:
All participants underwent detailed questionnaires, physical examinations, and laboratory tests to exclude diseases and medications affecting bone metabolism. Measurements were performed by uniformly trained professionals with real-time quality control, and any results with artifacts or deviations were excluded.

05
Clinical Significance: Returning Diagnosis to Authenticity, Aligning Standards with Clinical Practice
Establishment of a Reference Database for Bone Mineral Density in the Chinese Population Holds Multiple Strategic Implications for Clinical Practice:
First, more accurate diagnosis.By leveraging the specific skeletal development patterns, living environments, and genetic backgrounds of the Chinese population, T-score calculations now have a truly applicable reference framework, significantly reducing the risk of systematic misdiagnosis. This directly aligns with the 2022 guidelines’ fundamental requirement for “same-ethnicity, same-sex” reference databases.
Second, the standards are more authoritative.Supported by the National Science and Technology Major Project, and led by China’s top orthopedic hospitals with participation from multiple centers across the country, this initiative ensures robust data quality and scientific rigor. Diagnostic criteria based on data from the Chinese population can more accurately reflect the skeletal health status of people in China.
Third, data is traceable.Every case included in the dataset has complete clinical data and quality control records, making the database itself a traceable and verifiable scientific research achievement. This provides a reliable data foundation for subsequent clinical research and evidence-based medical practice.
Fourth, promote the independent research and development of domestically produced medical devices.By establishing bone mineral density diagnostic criteria specific to the Chinese population, this project helps break foreign technological monopolies, promotes the research and development of domestically produced medical devices, and achieves self-reliance and controllability in the field of bone health.
06
Conclusion: Precision Diagnosis Begins at the Data Source
The accuracy of bone mineral density testing depends not only on the hardware performance of the equipment but also, more critically, on the underlying reference standards.
An excellent bone densitometer equipped with a database unsuitable for the target population is akin to a precise ruler marked with the wrong scale—no matter how accurate the measurement, the comparative results will be incorrect. This underscores the core significance of the “same ethnicity, same sex, and same age” reference standards repeatedly emphasized in the 2022 guidelines.
The establishment of a reference database for bone mineral density in the Chinese population is precisely aimed at addressing this fundamental issue. It represents a scientific output of the National Major Science and Technology Project, the culmination of a nationwide multicenter collaboration led by Shanghai Sixth People’s Hospital, and a foundational initiative to restore authenticity and precision to bone health assessment in China.Only by relying on data from the Chinese population can we truly ascertain the prevalence of osteoporosis in China and provide a reliable basis for clinical diagnosis and treatment.