Juncell Therapeutics Advances GC101 TIL Therapy into Phase II Trial for Advanced NSCLC Following Promising Phase Ib Results
From March 25 to March 28, 2026, by2026 European Lung Cancer Congress (ELCC), Co-Organized by the European Society for Medical Oncology (ESMO) and the International Association for the Study of Lung Cancer (IASLC)To be grandly held in Copenhagen, Denmark.
AsThe Most Influential in the Global Lung Cancer FieldAs one of the leading international academic conferences, ELCC brings together top experts in the field of thoracic oncology from around the world, serving as a vital platform for exchanging cutting-edge scientific advancements, clinical data, and educational practices.
At this conference, JunSai Bio will officially announce“Autologous Natural Tumor-Infiltrating Lymphocyte Injection (GC101) for the Treatment of Advanced Non-Small Cell Lung Cancer (NSCLC)”Protocol for the Phase Ib Clinical Trial (MIZAR-005)
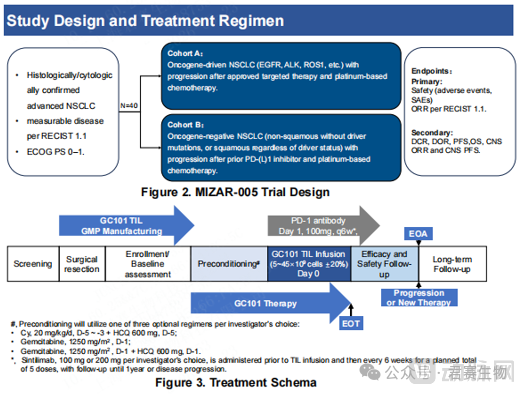
MIZAR-005 (NCT06473961) is a Phase Ib, open-label, single-arm clinical trial designed to evaluate the safety and efficacy of GC101 TIL cell injection in advanced non-small cell lung cancer (NSCLC). The primary endpoints are safety and objective response rate (ORR), while the secondary endpoints include key metrics such as disease control rate (DCR), duration of response (DOR), progression-free survival (PFS), and overall survival (OS).
● Abstract Number:#219eTiP
● Abstract Title:Trial in progress: A Phase Ib, Open-label, Single-arm Trial of Autologous Natural Tumor-Infiltrating Lymphocyte Injection (GC101) in Patients with Advanced Non-Small Cell Lung Cancer (NSCLC) (MIZAR-005)
● Principal Investigator:Prof. Lu Shun
● Key Research Institutions: Shanghai Chest Hospital, Affiliated to Shanghai Jiao Tong University
● Display Time:2026.3.25-3.28
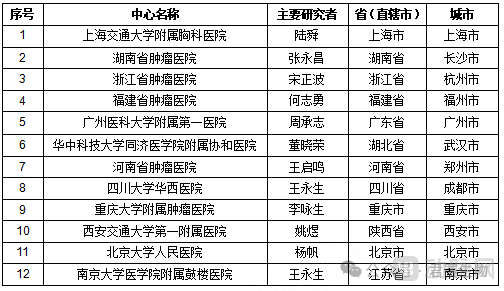
Based on the exploratory findings and safety validation from Phase Ib clinical trials, JunsaibioFormally Launching the Phase II Clinical Study of GC101 for the Treatment of Advanced NSCLC. The MIZAR-005 project is currently atLead Site: Shanghai Chest Hospital, Shanghai Jiao Tong University School of Medicine; Multiple Subsites Nationwide, Including Hunan Cancer HospitalLaunched in succession.
Lung Cancer Is the Malignant Tumor with the Highest Incidence and Mortality Rates in China[1,2]. Non-small cell lung cancer (NSCLC) accounts for 80%-85% of lung cancer cases, with approximately 70% of patients diagnosed at an advanced stage of the disease, and the 5-year survival rate is only 15%.[3]. Although TIL therapy has shown promising prospects in the treatment of solid tumors[4-7], but traditional TIL therapy relies onHigh-intensity lymphodepleting chemotherapy and high-dose IL-2 administration, with prominent adverse reactions[8-11]This is the core pain point constraining its widespread application.
To address the industry bottlenecks of TIL therapy, Junsaibio has independently developed the world’s firstNo high-intensity lymphodepleting chemotherapy or IL-2 administration requiredGC101, an innovative natural TIL therapy. This therapy has demonstrated excellent efficacy and a favorable safety profile in Phase I clinical studies.[12]: Data show that GC101 achieved in advanced-stage patients who had received a median of three prior lines of therapy,41.7% Objective Response Rate (ORR) and 66.7% Disease Control Rate (DCR), the 12-month overall survival rate was 66.7% (95% CI: 33.7%, 86.0%). The median follow-up time was 13.0 months (range: 1.5–31.1), and the median overall survival had not been reached.

“Targeted and immunotherapies for advanced non-small cell lung cancer (NSCLC) have made significant progress in recent years, but challenges remain, such as overcoming resistance mechanisms and addressing tumor heterogeneity. For advanced NSCLC, the benefits of immunotherapy and chemotherapy after first-line treatment failure are limited, and there is still an unmet clinical need for cell therapies with higher safety profiles and more durable efficacy.”
“Preliminary clinical trial data for Junsaibio’s GC101 have demonstrated promising efficacy, and we look forward to further uncovering the potential of TIL therapy in treating patients with non-small cell lung cancer (NSCLC). We hope this innovative TIL therapy will benefit more lung cancer patients and tangibly improve their quality of life.”
GC101 was developed based on Junsai Bio’s proprietary DeepTIL™ cell enrichment and expansion platform. It is the TIL therapy pipeline with the most advanced development progress at Junsai Bio, and alsoThe world’s first natural TIL therapy requiring neither high-intensity lymphodepleting chemotherapy nor IL-2 administration.
Clinical data show that GC101 has delivered long-term benefits to patients with advanced metastatic solid tumors who have failed multiple lines of therapy, includingMelanoma, Non-Small Cell Lung Cancer, Cervical Cancer, Endometrial Cancer, Glioma, Pancreatic CancerPatients with tumors of this type demonstrated objective response efficacy following treatment with GC101,The longest disease-free survival has exceeded 4 years.
Subject recruitment and screening for the MIZAR-005 clinical trial have been conducted at medical institutions including Shanghai Chest Hospital, Shanghai Jiao Tong University School of Medicine, and Hunan Cancer Hospital. The primary inclusion criteria are as follows:
■ Key Inclusion Criteria:
1. Aged 18–75 years, both males and females;
2. Patients with advanced non-small cell lung cancer (NSCLC) confirmed by cytology or histopathology;
3. Failure of targeted therapy and platinum-based doublet chemotherapy, or failure of PD-(L)1 inhibitor combined with platinum-based chemotherapy;
4. Presence of tumor lesions suitable for tissue harvesting to produce TILs, and the patient is able to undergo the relevant tissue procurement surgery;
5. ECOG performance status 0-1;
6. Adequate hematologic and end-organ function.
■ Major Exclusion Criteria:
1. Presence of severe underlying diseases;
2. Presence of a major infectious disease;
3. Pulmonary fibrosis, interstitial lung disease, acute lung disease;
4. Unstable brain metastases or those accompanied by clinical symptoms.
■ Contact Information:
Clinical Trials Email: clinicaltrials@juncell.com
Contact Number: 021-69990503
Teacher Zhang: 18019732895 (WeChat)
Teacher Cheng: 18001759113 (same as WeChat)
In the early-phase clinical trials of Junsaibio’s GC101 TIL therapy, multiple lung cancer patients have achievedPRand target lesionsCRits favorable efficacy is expected to drive a paradigm shift in lung cancer treatment from "prolonging survival" to "potential cure."
>>Lesion Clearance: GC101 TIL Therapy Delivers Sustained Benefits for Patients with KRAS-Mutant Lung Cancer
>>Again! Lung Cancer Patient’s Tumor Significantly Shrinks
>>Rapid Tumor Shrinkage in Lung Cancer Patients with KRAS Mutations
>> Advancing TIL Therapy: GC101 Leads to Sustained Tumor Shrinkage in Lung Cancer Patients
* References:
1. Chinese Medical Association. Zhonghua yi xue za zhi. 2023;103(27):2037-2074.
2. Xia C, Dong X, Li H, et al. Chin Med J. 2022;135(5):584-590.
3. Hong Y, Park S, Lee MK, et al. Sci Rep. 2022;12(1):13588.
4. Rosenberg SA, Lotze MT, Muul LM, et al. Surgery. 1986;100(2):262-272.
5. Chesney J, Lewis KD, Kluger H, et al. J Immunother Cancer. 2022;10(12).
6. Sarnaak AA, Hamid O, Khushalani NI, et al. J Clin Oncol.2021;39(24):2656-2666.
7. Schoenfeld AJ, Lee SM, Doger de Speville B, et al. Cancer Discov. 2024.
8. Betof Warner A, Corrie PG, Hamid O, et al. Clin Cancer Res. 2023;29(10):1835-1854.
9. Dutcher JP, Schwartzentruber DJ, Kaufman HL, et al. J Immunother Cancer. 2014;2(1):26.
10. Rosenstein M, Ettinghausen SE, Rosenberg SA, et al. J Immunol. 1986;137(5):1735-1742.
11. Martins F, Sofiya L, Sykiotis GP, et al. Nat Rev Clin Oncol. 2019;16(9):563-580.
12. Guo J, et al. J Immunother Cancer. 2022; 10:e004612.