Regeneron's Eylea HD (Aflibercept 8mg) Becomes First Anti-VEGF Therapy Approved for Once-Every-Five-Months Dosing in wAMD and DME
Recently, Regeneron Pharmaceuticals, Inc. (“Regeneron”) announced that aflibercept 8 mg (Eylea HD) has received FDA approval to extend the dosing interval to once every five months (once every 20 weeks) for the indications of wet age-related macular degeneration (wAMD) and diabetic macular edema (DME). Patients with these conditions may extend their dosing interval after successfully completing one year of initial therapy. With this approval, Eylea HD becomes the first anti-VEGF ophthalmic therapy with a dosing interval of up to once every five months.
Fusion Protein, Enabling Longer Intraocular Half-Life
Aflibercept is a recombinant fusion protein composed of the extracellular domains of human vascular endothelial growth factor (VEGF) receptors 1 and 2 fused to the Fc domain of human IgG1. This structure is fundamentally different from that of conventional monoclonal antibody drugs.
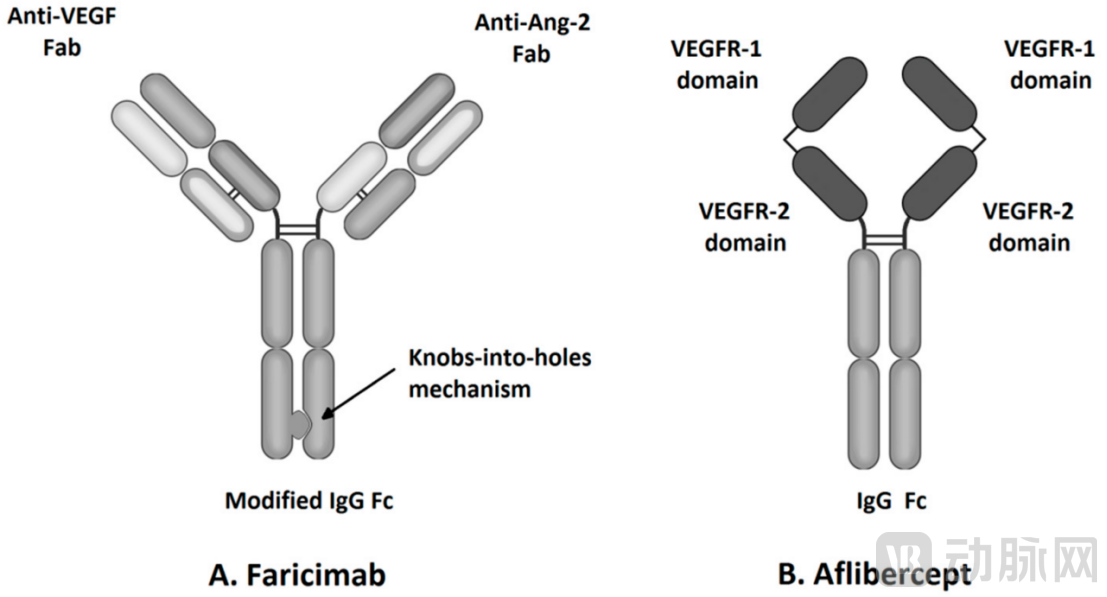
First, in terms of target coverage, aflibercept, as a VEGF receptor-Fc fusion protein, can bind to multiple ligands such as VEGF-A, VEGF-B, and placental growth factor (PlGF), whereas the first-generation anti-VEGF drug ranibizumab primarily targets VEGF-A. This broader target coverage theoretically enables more comprehensive inhibition of pathological angiogenesis.
Secondly, in terms of affinity, aflibercept exhibits a significantly higher binding affinity to VEGF-A (Kd ≈ 0.5 pM) than ranibizumab (Kd ≈ 19 pM) and bevacizumab (Kd ≈ 58 pM). High affinity implies that fewer drug molecules are required to achieve equivalent or even stronger biological effects.
More critically, the Fc fusion protein structure confers a longer intraocular half-life to aflibercept. According to literature reports, the half-life of aflibercept in the vitreous cavity is approximately 9–10 days, significantly longer than that of ranibizumab, which is about 3 days. This constitutes the molecular basis for aflibercept’s ability to support dosing every two months since its market launch, whereas ranibizumab requires monthly administration.
The development strategy for aflibercept 8 mg is more straightforward: while maintaining the original molecular structure, the drug concentration was increased from 40 mg/mL to 114.3 mg/mL, and the single-injection dose was raised from 2 mg to 8 mg. This four-fold increase in molar dosage further extends the duration of therapeutic effect within the eye, thereby supporting longer dosing intervals.
96-Week Data Validate the Safety and Efficacy of Long-Acting Administration
This FDA approval to extend the dosing interval to 5 months is primarily based on 96-week data from two global Phase III clinical trials—PULSAR (wAMD) and PHOTON (DME).
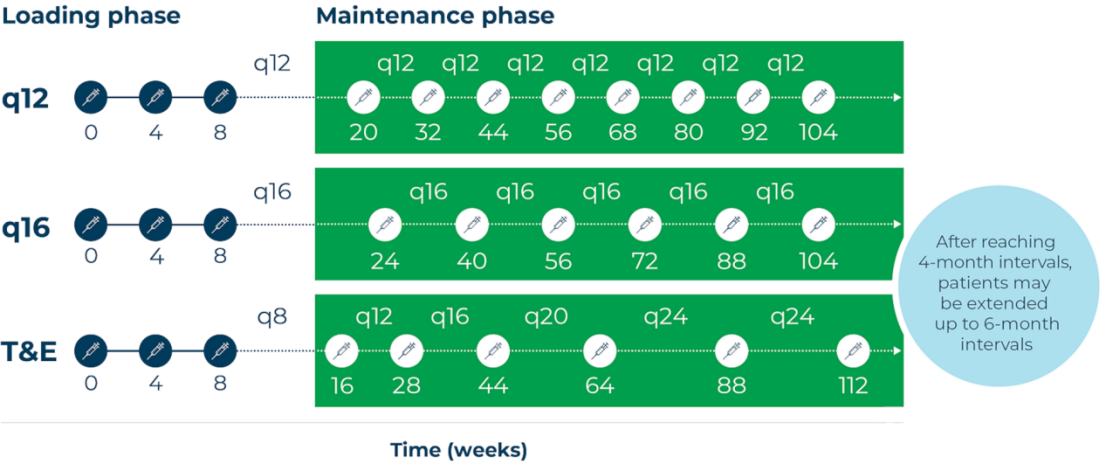
The PULSAR study enrolled 1,009 treatment-naïve patients with wet age-related macular degeneration (wAMD), who were randomized into three groups: aflibercept 8 mg every 12 weeks, aflibercept 8 mg every 16 weeks, and aflibercept 2 mg every 8 weeks. All patients initially received three monthly loading doses.
Key design features: Starting from Week 52, the dosing interval for patients in the 8 mg group may be extended based on predefined dose adjustment criteria, up to a maximum of once every 24 weeks (6 months). This allows investigators to explore the maximum extent to which injection intervals can be lengthened under an individualized treatment strategy.
At 96 weeks, the 8 mg group was comparable to the 2 mg group in terms of improvement in best-corrected visual acuity (BCVA). The mean changes from baseline in BCVA were +5.6, +5.5, and +6.6 letters in the 8q12, 8q16, and 2q8 groups, respectively, and the difference between the 8 mg and 2 mg groups met the prespecified non-inferiority criteria.
This means that, with fewer injections, patients in the 8 mg group did not experience any compromise in visual acuity benefits.
In terms of anatomical improvement, the 8 mg group demonstrated superior resolution of fluid accumulation. At Week 16 (i.e., after completion of three loading doses), the proportion of patients achieving a dry fovea was 63% in the 8 mg group, significantly higher than the 52% observed in the 2 mg group. This is a noteworthy signal—during the loading dose phase, the higher dose exerted a more rapid effect in suppressing vascular leakage.
The 96-week data from the PULSAR study demonstrated the feasibility of extending the dosing interval.
Among patients in the 8q16 group (randomized to the every-16-weeks arm) who completed 96 weeks of treatment, 78% ultimately had a dosing interval of ≥16 weeks, 53% achieved an interval of ≥20 weeks, and 31% reached 24 weeks.
In the PHOTON study of DME indications, 72% of patients achieved a dosing interval of ≥16 weeks at 96 weeks, and 44% achieved ≥20 weeks.
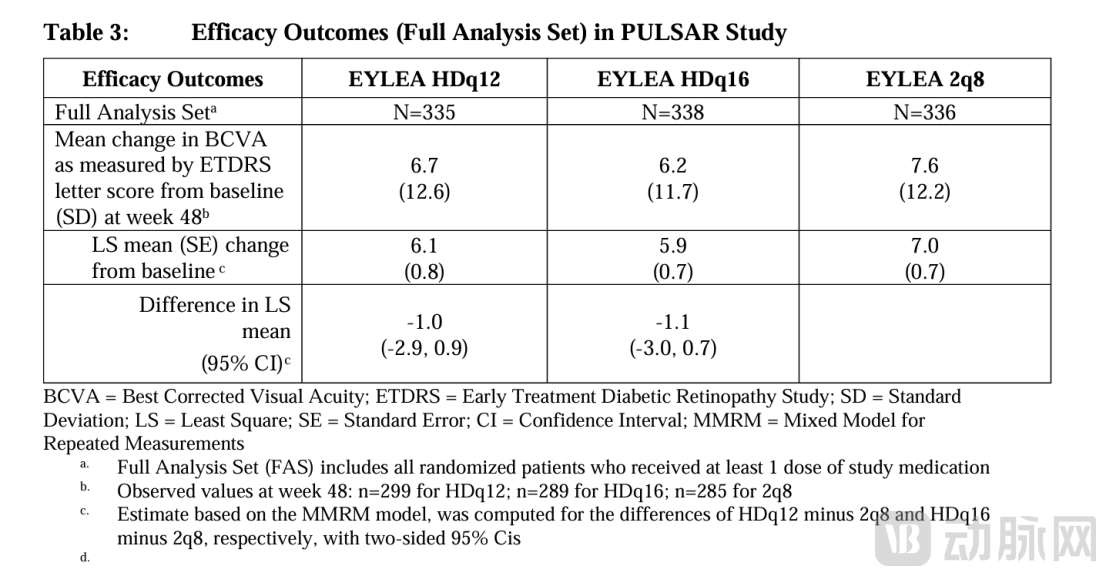 Efficacy Outcomes in the PULSAR Study
Efficacy Outcomes in the PULSAR Study
In terms of injection frequency, patients in the 8q16 group received an average of only 8.2 injections over 96 weeks, compared with an average of 12.8 injections in the 2q8 group. This indicates that the 8 mg regimen reduced the number of injections by approximately 36% over the 2-year treatment period.
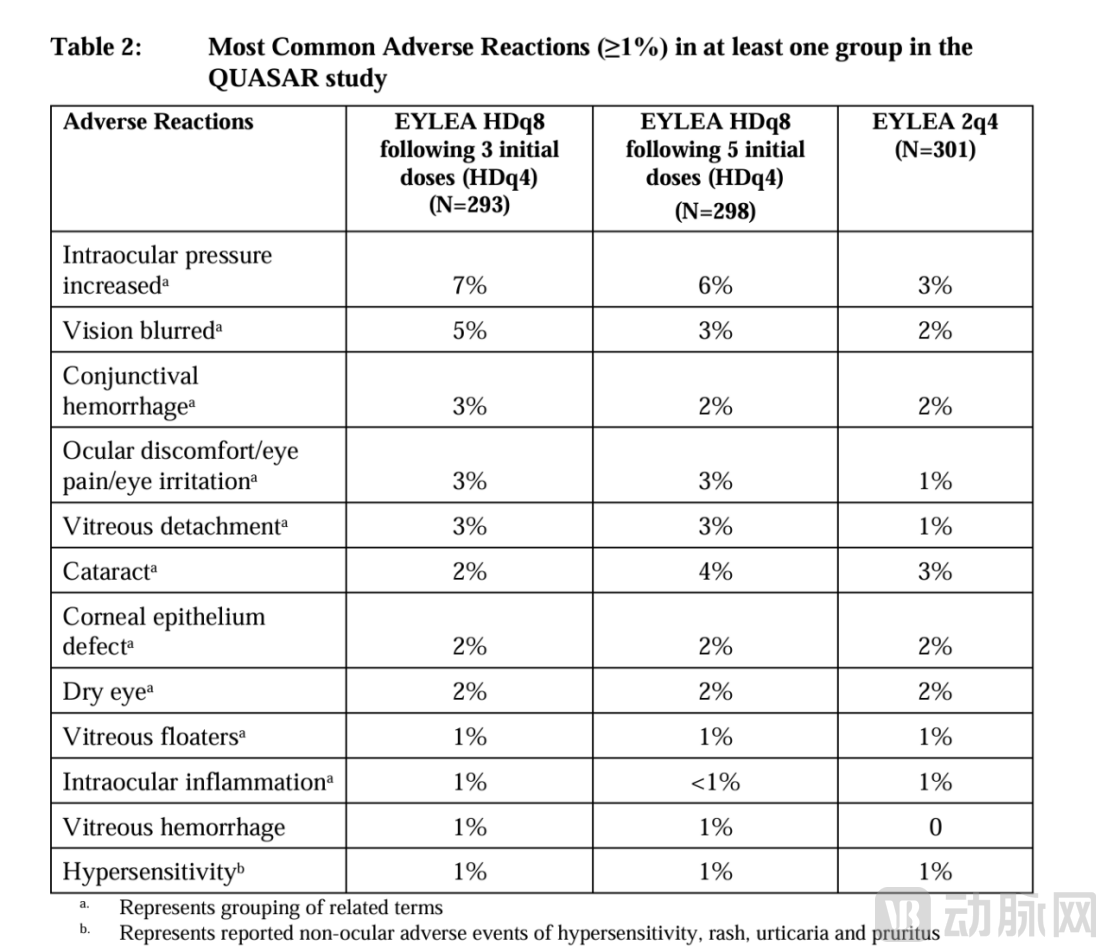
In both studies, the safety profile of aflibercept 8 mg was consistent with that of the 2 mg formulation, and no new safety signals were identified. The incidence of ocular adverse events was similar across all treatment groups.
Extended Intervals: Strategic Defense Before the Patent Cliff
Aflibercept 2 mg (Eylea) is the flagship product of Regeneron and Bayer. In 2022, global sales of Eylea reached $9.647 billion, ranking it as the 10th best-selling drug worldwide. The U.S. market contributed $6.265 billion, while markets outside the United States contributed $3.383 billion.
However, the core active ingredient patent for Eylea has expired in multiple countries and regions. In 2020, the key active ingredient patent expired in China; patent protections in other countries and regions have also successively approached expiration. According to Yaozhi Data, more than 10 aflibercept biosimilars worldwide are currently in Phase III clinical trials or later stages, and Qilu Pharmaceutical’s biosimilar submitted its registration application in 2022.
In the face of competition from biosimilars, originator companies have essentially three strategic responses: expanding indications, extending patent protection periods, and launching next-generation products. Aflibercept 8 mg serves as the core vehicle for the third strategy.
The business logic of aflibercept 8 mg can be broken down into three levels.
First, extending the dosing interval itself constitutes a differentiated barrier. In the field of ophthalmic anti-VEGF therapy, dosing frequency is a key factor influencing patient choice. Aflibercept 8 mg, which enables a 5-month dosing interval, has established a clear advantage in convenience over competitors requiring monthly or bi-monthly injections. This convenience advantage helps maintain the premium pricing power and prescription preference for the originator product as biosimilars enter the market.
Second, the “dosage form upgrade” strategy extends product lifecycle. The progression from 2 mg to 8 mg is essentially a “dose escalation” strategy. Under this approach, the regulatory approval pathway for the new strength is relatively streamlined (leveraging existing safety and efficacy data), while market exclusivity can be prolonged through new patents (such as formulation patents and method-of-use patents). This is akin to the extended-release formulation iteration strategies commonly seen in the pharmaceutical industry.
Third, individualized dosing regimens can strengthen the bond between physicians and patients. The dose-adjustment protocol employed in the PULSAR study allows physicians to individually lengthen or shorten dosing intervals based on patients’ disease activity. This “treat-assess-adjust” model aligns closely with the Treat-and-Extend strategy widely adopted in clinical practice. Once physicians and patients become accustomed to such an individualized regimen, the switching costs associated with transitioning to alternative products increase significantly.
However, in the field of ophthalmic anti-VEGF therapy, aflibercept is not the only option for “extended dosing intervals.” Faricimab (Vabysmo), a bispecific antibody targeting VEGF-A and Ang-2 developed by Roche/Novartis, was approved in 2022 and enables dosing every four months. In 2024, global sales of faricimab exceeded $3 billion, demonstrating strong growth momentum.
The advantages of aflibercept 8 mg lie in its more mature molecular mechanism (fusion protein technology has been applied for over a decade), more robust safety data (over 85 million injections administered globally), and a dosing interval extending toward six months. However, faricimab is also advancing research on longer dosing intervals, and the “interval race” between the two continues.
Furthermore, aflibercept 8 mg (Eylea®®8 mg) was approved for marketing in China in May 2025 for the treatment of nAMD, with an initial regimen of once-monthly injections for the first three months, which can then be extended to once every four months. However, the five-month dosing interval recently approved by the FDA has not yet received approval in China. Given factors such as significant pressure on medical insurance payments, prominent issues with patient adherence, and intense competition from biosimilars in the Chinese market, the speed of implementation and pricing strategy for the five-month interval regimen will directly impact the product lifecycle of aflibercept in China.