Alzheimer's Disease: Drug Development Setbacks and Soaring Care Costs—Can Prediction Be the Solution?

Dr. Brain
Developer of AI-Powered Diagnostic Platform for Brain Science

iNEURO
Provider of Comprehensive Brain Science Medical Solutions
“We become ridiculous, incompetent, and comical. But this is not who we truly are; it is our disease that makes us so,” said Alice, a patient with early-onset Alzheimer’s disease, in *Still Alice*.
Alzheimer’s disease (AD) is prevalent in our communities, primarily affecting individuals aged 65 and older. Like many chronic diseases, while it may not appear as aggressive as cancer, the toll it takes on patients and their families is immeasurable. Witnessing loved ones regress along the journey of life—decades of wisdom gradually fading until only an aged shell remains—can be more terrifying than physical suffering.
As of 2015, the global number of Alzheimer’s disease (AD) patients had reached 46.8 million, with over 6 million cases in China. According to reports from the same year, a new symptom of AD emerges every seven years. More than a century has passed since AD was first identified, yet humanity has neither found an effective cure nor fully elucidated its pathology. This does not imply inaction; in fact, generations of scientists have relentlessly pursued solutions to this century-old challenge.
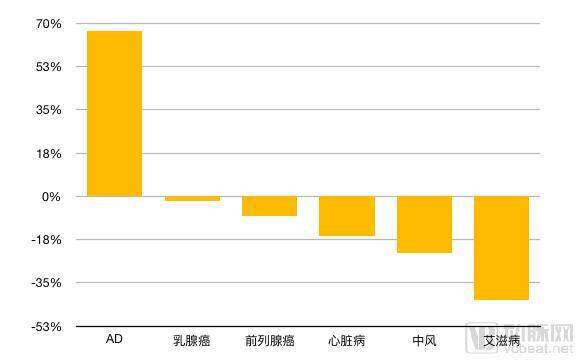
Percentage Change in Mortality Rates by Condition, 2000–2010
In June 1864, Alois Alzheimer was born in Bavaria, Germany. His affluent family provided him with a favorable environment for personal development. To enable the young Alzheimer to attend the Royal Humanities Gymnasium, his family relocated from Bavaria to Berlin, and he subsequently enrolled at the University of Würzburg to study medicine.
In 1901, Alzheimer lost his wife, Cecilie. The grief from this loss fueled his research. That year, he observed a 51-year-old female patient, Auguste Deter, at his private psychiatric hospital. Her puzzling symptoms, such as short-term memory loss, baffled everyone, and Alzheimer became fascinated with her case.
An interview record that has circulated to this day reflects the despair of Augustus, as well as that of many other patients with Alzheimer’s disease.
"Write a 5."
“A woman,” Augustus wrote.
"Write an 8."
“Augustus.” She wrote her name.
During the writing process, she kept muttering over and over again, “I have lost myself, so to say…”
Alzheimer’s disease is not a process of instantaneous memory loss. She is aware that she is gradually losing herself, yet feels powerless to stop it.
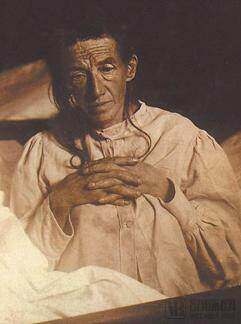
Augustus
In 1906, Auguste Deter reached the end of her life and donated her brain for scientific research. Alois Alzheimer brought her case records and brain to Munich for further study, where he discovered that a special substance had accumulated in her cerebral cortex and that much of the cortical tissue had undergone necrosis.
Using Bielschowsky’s staining technique, Alois Alzheimer discovered two abnormalities in her brain: amyloid plaques and neurofibrillary tangles, which later became hallmarks for diagnosing dementia. However, these findings did not attract significant attention from the medical community at the time. It was not until 1910 that his supervisor and research partner, Emil Kraepelin, formally named this peculiar disease “Alzheimer’s disease” in his book Handbook of Psychiatry.
Over the subsequent nearly 70 years, medical research on Alzheimer’s disease (AD) continued, but due to technological limitations, there were few significant breakthroughs. It was not until the 1970s that AD gradually entered public awareness. In 1974, the U.S. Congress established the National Institute on Aging (NIA) under the National Institutes of Health (NIH). In the same year, neuropsychiatrists Davies and Maloney proposed the cholinergic deficit hypothesis, which remains the primary mechanistic basis for pharmacological interventions aimed at slowing AD progression.
Here is another individual who dedicated himself to Alzheimer’s disease (AD) research due to his wife’s condition: Jerome H. Stone. The wife of this renowned businessman was first diagnosed with AD in 1970; despite his immense wealth, he was powerless against this incurable disease.
Ston was surprised by the scarcity of global information on Alzheimer’s disease (AD). From that point on, he began frequently communicating with numerous neurologists and attempted to organize relevant scholars. In 1980, the Alzheimer’s Association was established, with Ston serving as its first president. To this day, the association continues to exert significant influence in the field of mental health.
According to 1998 statistics, Alzheimer’s disease (AD) was the third most costly disease in the United States, surpassed only by cancer and cardiovascular diseases. The average daily cost per AD patient was three times that of an individual without the condition.
The AD drug market was valued at $5.8 billion in 2011, a figure projected to reach $14.5 billion by 2020. In 2014, the total long-term care costs for AD patients amounted to $214 billion, with an estimated increase to $1.2 trillion by 2050.
Data released by Alzheimer’s Disease International shows that in 2013, there were 44 million people worldwide living with dementia, 50%–75% of whom had Alzheimer’s disease (AD). In 2015, there were 9.9 million new cases of dementia globally, equivalent to one new case every three seconds on average. Worldwide, the total cost of care for dementia in 2015 was estimated at $818 billion, an increase of $214 billion compared with 2010.
So, which factors are significantly associated with AD?
Age is a significant factor influencing Alzheimer's disease (AD). One study indicated that patients under 65 years old account for 4% of the total AD population, those aged 65–74 constitute 6%, patients aged 75–84 make up 44%, and individuals aged 85 and older represent 46%. Meanwhile, the prevalence of AD in women is approximately twice that in men.
Secondly, genes are another important influencing factor. Three genes are currently known to be associated with early-onset Alzheimer's disease (AD): APP (amyloid precursor protein) on chromosome 21, PSEN1 (presenilin 1) on chromosome 14, and PSEN2 (presenilin 2) on chromosome 1. Late-onset AD is associated with CR1, PICALM, TREM2, and several SORL1 genes on chromosome 11.
To address these challenges, companies both in China and abroad have invested in Alzheimer’s disease (AD) therapeutics. VCBeat has compiled a list of recently funded enterprises, revealing several emerging trends.

Financing and Business Status of Select AD Companies (Excluding Large Pharmaceutical Companies)
If clinical treatment could delay the onset of Alzheimer’s disease by one year for all patients, the number of cases would be reduced by 9 million. In developed countries, the average annual cost per Alzheimer’s patient is $33,000. Early diagnosis and diagnostic intervention can significantly postpone institutional care placement, resulting in an average net savings of $10,000 per year. A five-year delay in onset would save $5 trillion over 30 years.
Historical AD detection involved lumbar puncture to extract cerebrospinal fluid for AβTesting for amyloid and tau proteins. This method requires prior administration of anesthesia, and lumbar puncture can cause severe neuropathic pain, making it often difficult for patients to accept.
Nowadays, the use of artificial intelligence for early screening and diagnosis of Alzheimer's disease (AD) is becoming increasingly mature, with many companies having implemented corresponding products in hospitals. This technology not only spares patients from the discomfort of invasive tests but also generates quantitative results within a short period of time.
Avalon AI, a UK-based company, predicts the future risk of developing Alzheimer’s disease (AD) using brain MRI scans. By leveraging deep learning technology to develop computer-aided medical imaging diagnostic tools, the company has currently achieved a 75% accuracy rate in effectively predicting dementia.
Beijing Yasen Technology Development Co., Ltd., a Chinese AI company, analyzes patients’ brain conditions by integrating clinical medical records, neuropsychological scales, electroencephalogram (EEG) data, and various imaging datasets. Leveraging multimodal and deep learning technologies, and based on a standard brain template for the Chinese population as well as a specialized Alzheimer’s disease (AD) database with five years of continuous follow-up data, the company has trained diagnostic and predictive models. These models enable dementia classification and five-year disease progression prediction for patients, while also generating structured reports.
The highlight of Yasen Technology’s AD diagnostic prediction system lies in its ability to assist clinicians in making diagnoses, with data that is evidence-based and traceable. It enables precise disease subtyping for patients, including normal age-related decline, amnestic mild cognitive impairment (aMCI), dysexecutive mild cognitive impairment (dMCI), and Alzheimer’s disease (AD), thereby enhancing the effectiveness of treatment strategies. For patients not yet presenting with severe symptoms, the system provides early warnings to facilitate timely and effective interventions. Precise subtyping also holds significant importance for new drug development and clinical trials, as it helps identify the extent of differential expression of various biomarkers across different patient subtypes.
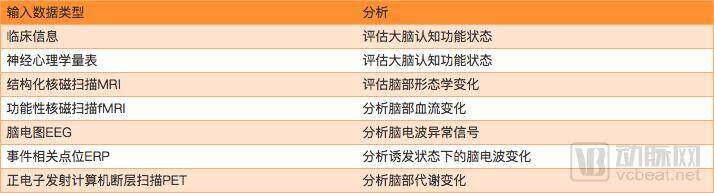
Yasen Technology Multimodal Data Analysis
Cognitive assessment at the early stages is highly effective in managing dementia-related disorders. In China, many patients have already progressed to the stage of dysexecutive mild cognitive impairment (dMCI) or Alzheimer’s disease (AD) by the time they undergo diagnostic evaluation. Therefore, early screening is essential. For dementia-related conditions, only timely detection and appropriate intervention can delay the onset of AD.
Another Chinese company, iNEURO, has also made progress in predicting Alzheimer’s disease (AD). The iNEURO AI-based EEG analysis system addresses the challenge of interpreting electroencephalogram (EEG) readings, enabling EEG examinations to serve as a preliminary screening tool prior to other diagnostic tests (such as imaging). Furthermore, it facilitates comparative validation studies in conjunction with blood tests and imaging modalities.
iNEURO is currently focusing on optimizing algorithms for epilepsy and Alzheimer’s disease (AD). In a July interview with VCBeat, its founder, Dai Shenyi, stated that the company plans to expand into various EEG-related neurological disorders in the future. “EEG devices can be applied across multiple medical departments. Currently, we are using epilepsy as our entry point because the demand for EEG in epilepsy diagnosis is the most rigid, with EEG serving as the gold standard and no other more effective diagnostic methods available at present. Of course, we will not limit ourselves to epilepsy; rather, we aim to use it as a breakthrough to establish a pathological database. Once the database is established, we can enter any medical specialty requiring EEG testing, including AD.”
Yiwei Medical Technology Co., Ltd., established in 2017, has also set its sights on the large market for Alzheimer’s disease (AD). Its Brain Doctor Intelligent Diagnosis Cloud Platform is...system, leveraging AI technology for early screening and diagnosis of Alzheimer's disease (AD), has already undergone clinical trials at multiple Grade A tertiary hospitals, achieving an accuracy rate of 85%.
The Dr. Brain system has independently established a neuroimaging database of the Chinese population by collecting large-scale brain MRI data, thereby enabling precise detection and evaluation of morphological data for each subject. Through collaborations with multiple top-tier hospitals across China, it has acquired tens of thousands of high-quality, standardized medical imaging cases.
The initial therapeutic approach introduced for Alzheimer’s disease (AD) was not pharmacological treatment, but rather a method known as reminiscence therapy, which treats patients through psychological suggestion.
Hsieh et al. conducted a 12-week randomized controlled trial involving 61 patients with mild-to-moderate dementia in nursing homes in Taiwan. Psychiatric nurses developed a structured intervention protocol, under which the intervention group received weekly group reminiscence therapy sessions based on life review, each lasting 40–50 minutes. Participants were encouraged to share their personal stories using old photographs, records, and other meaningful materials.
The results indicated that post-intervention assessments using the Geriatric Depression Scale and the Apathy Evaluation Scale showed significant improvements in depressive mood, behavioral apathy, and cognitive apathy symptoms in the intervention group. Additionally, depression scores on the Neuropsychiatric Inventory were significantly reduced. Therefore, it is concluded that group reminiscence therapy can effectively treat apathy and depressive symptoms in elderly patients with mild to moderate dementia.
Recently, a U.S. companySmart Brain AgingLaunched a virtual online product similar to reminiscence therapy, its Brain U Online platform provides users with over 20,000 exercises related to various cognitive skills online, focusing on processing speed, memory, and attention. Hundreds of these exercises can be redesigned for mobile internet use through the application. Additionally, the program includes a virtual classroom where users can participate in social activities and engage in conversations with others. Based on data provided by the company, this product reduces the negative cognitive impacts of Alzheimer’s disease by 45% and delays its progression by 2.5 years.
Although reminiscence therapy can effectively intervene in mild to moderate Alzheimer's disease (AD), it ultimately proves insufficient for patients who have already manifested severe AD symptoms.
In 1978, the National Institute on Aging (NIA) collaborated with Warner-Lambert Pharmaceutical Company (now Pfizer) to initiate the first recorded clinical trial of a drug aimed at treating the symptoms of Alzheimer’s disease (AD). It was not until 1993 that the U.S. Food and Drug Administration (FDA) formally approved tacrine, the first medication for the treatment of AD.
A significant cause of Alzheimer's disease (AD) is acetylcholine deficiency, which leads to memory decline, disorientation, and changes in behavior and personality. Tacrine can inhibit cholinesterase, promote the release of acetylcholine in the brain, and increase its levels. However, this drug has a very short half-life, requiring daily administration, and it causes significant liver damage.
Over the next decade, representative drugs for improving cholinergic neurotransmission—Aricept, Exelon, and Galantamine—were successively approved by the FDA. Meanwhile, researchers also attempted to develop numerous drugs through other channels, including agents that improve cerebral blood circulation and brain cell metabolism; calcium antagonists used to reduce neuronal damage or death caused by calcium ion influx; and hormonal medications employed to alleviate patient symptoms.
In 2015, a team led by Professor Jürgen Götz at the University of Queensland discovered a promising new approach for treating Alzheimer’s disease (AD). Their research demonstrated that repeated exposure to scanning ultrasound effectively opened the blood-brain barrier in AD mice without causing ischemic injury or neuronal degeneration. This facilitated drug delivery into the brain, leading to efficient clearance of amyloid-beta (Aβ) proteins and subsequent restoration of memory function.
In recent years, many large pharmaceutical companies have launched new drug development programs aimed at curing Alzheimer’s disease (AD). However, due to the slow progression of AD and the high costs of research, some companies have had to announce the abandonment of their respective studies.One lesson from the experimental failure is that patients did not undergo brain scans before entering the trial. Without distinguishing between different types of dementia or even confirming a diagnosis, many patients would not respond to the drug.
In January 2018, Pfizer announced the closure of its R&D programs for Alzheimer’s disease and Parkinson’s disease drugs. Roche’s new drug also suffered a devastating failure in clinical trials, with similar outcomes seen at other companies. Therefore, to date, we still cannot speak of a “cure”; instead, we must pin our hopes on early detection to delay disease progression.
On June 24, 2018, a study published in the journal *Neuron*, under the Cell Press imprint, employed big data methodologies to reveal an astonishing potential etiologic factor—viral infection. This finding suggests that amyloid-beta, the primary research focus of the past several decades, may have little relevance to the treatment of Alzheimer’s disease (AD).
In this study, scientists first analyzed 944 brain samples, including 622 from patients with Alzheimer’s disease (AD) and 322 from healthy donors. They conducted two tests: the first involved DNA analysis to identify differences in genetic information between the two groups, and the second involved RNA analysis to determine whether their gene expression levels were consistent.
The results indicate that patients exhibit distinct gene expression patterns compared to healthy individuals. In brain samples from patients, researchers observed significantly elevated levels of two types of human herpesviruses, which were positively correlated with Alzheimer’s disease (AD) symptoms. Scientists found that these viruses can affect the expression of “classic” AD-related genes, such as BACE1, PSEN1, and APBB2, within brain cells. In other words, many of the observed symptoms may simply be consequences of viral infection.
Based on the above results, researchers cannot conclusively state that AD is caused by viral infection; further validation of the findings is required.
Even though Phase III clinical trials may cost up to $1 billion, and despite it having been 15 years since the last Alzheimer’s disease (AD) drug reached the market—with potentially another 15-year wait for the next one—numerous industry giants continue to press forward in this field.
As public awareness of Alzheimer’s disease (AD) and disease prevention grows, an increasing number of people believe that treatment should not wait until after a formal diagnosis. At present, early prediction and prevention are key to improving quality of life. Some pharmaceutical companies have already begun testing drugs in populations at high risk for AD who have not yet developed symptoms. Thus, we can look forward to a future where establishing a connection between one’s “past self” and “future self” rests firmly in human hands.
Appendix: AD-Related Timeline
On November 3, 1906, the first case of AD was confirmed by Alois Alzheimer.
In 1910, psychiatrist Emil Kraepelin coined the term “Alzheimer” in a medical textbook.
In 1932, Schottky first reported cases of autosomal dominant hereditary AD.
In 1940, Van Bogaert, and in 1946, Essen-Moller, successively reported on the pathology of familial Alzheimer's disease (AD).
In 1963, electron microscopy revealed that neurofibrillary tangles are composed of double-helical filamentous structures.
In 1974, the U.S. Congress established the National Institute on Aging (NIA) as part of the National Institutes of Health (NIH).
In 1976, Dr. Robert Katzman declared that Alzheimer’s disease (AD) is the most common form of dementia and a major public health challenge. This sparked widespread attention to AD and led to the launch of numerous brain-related initiatives through the National Institutes of Health (NIH).
In 1978, the NIA partnered with Warner-Lambert Pharmaceutical Company (now Pfizer) to initiate the first clinical trial of a drug aimed at treating AD symptoms.
In 1979, Jerome Stone and other members of the AD family met with the NIA.
In 1980, the Alzheimer's Association was established, originating from meetings held in 1979. Stone served as the first chairman.
In 1984, beta-amyloid protein was discovered as the primary substance in Alzheimer's disease (AD).
In 1986, tau protein was discovered and identified as a major component in Alzheimer's disease (AD).
In 1986, reminiscence therapy was introduced by Norris into the care of dementia.
In 1990, St George-Hyslop discovered the genetic heterogeneity of AD.
In 1991, Goate et al. identified missense variants in the APP gene in cases of familial genetic disorders.
In 1993, the FDA formally approved the first cholinesterase inhibitor, Tacrine. Four additional Alzheimer's disease (AD) drugs were approved in the following decade.
On November 5, 1994, former U.S. President Ronald Reagan was diagnosed with Alzheimer's disease.
In 1995, Games et al. established the APP transgenic mouse model.
In 1999, Vassar et al. positionally cloned β-secretase. Active immunotherapy led by Schenk et al. achieved success in animal studies. Petersen et al. proposed the concept of "mild cognitive impairment."
In 2003, genetic research commenced, with the Alzheimer’s Association and the NIA beginning to enroll participants in the federally funded National Alzheimer’s Disease Genetic Study.
In 2017, AI technology was applied to the detection of Alzheimer's disease (AD), with companies such as Yasen Technology and Dr. Brain developing related products.
In January 2018, Australian and Japanese scientists developed a blood test capable of detecting Alzheimer’s disease-associated proteins in the blood.
June 23, 2018: New Discovery—Viral Infection May Lead to AD
References:
1. Tapan Kumar Kham.Biomarkers in Alzheimer’s Disease.
2. Fan Huiying. Progress in the Application of Reminiscence Therapy in Patients with Dementia.
3. Guokr. Ultrasound Therapy: Sounding the Challenge to Alzheimer’s Disease.
4. Chen Shengdi. Alzheimer's Disease: Yesterday, Today, and Tomorrow.
5. http://www.sohu.com/a/237476616_749000
6. https://www.europsy-journal.com/article/0924-9338(96)88643-3/abstract
7.http://www.chicagotribune.com/news/obituaries/ct-jerome-stone-obituary-met-20150105-story.html
8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2927892/
9. https://www.healthline.com/health/alzheimers-history
10. https://jamanetwork.com/journals/jamaneurology/fullarticle/787136