Clinical Practice Guideline: Diagnosis and Management of Allergic Rhinitis in Children

Bayer
Pharmaceutical Product R&D Developer
Pediatric Allergic Rhinitis (AR), also known as pediatric atopic rhinitis, is a non-infectious inflammatory disease of the nasal mucosa triggered by allergen exposure and primarily mediated by immunoglobulin E (IgE). It is one of the most common allergic disorders. Pediatric AR has become a major respiratory inflammatory disease in children, with a high incidence rate. The prevalence of AR among children in China is 15.79% (95% CI: 15.13–16.45), with regional variations as follows: Central China, 17.20%; South China, 15.99%; Northwest China, 15.62%; Taiwan, 15.33%; Southwest China, 15.07%; North China, 14.87%; and East China, which has the lowest prevalence at 13.94%. The prevalence has been increasing year by year.
Allergic rhinitis (AR) symptoms in children significantly impact their quality of life. Because the symptoms of pediatric AR are easily confused with those of the common cold, many affected children fail to receive timely and accurate diagnosis and treatment after onset. Therefore, standardized diagnosis and treatment of pediatric AR, as well as mitigation of its impact on children’s quality of life, are of particular importance. In recent years, clinical guidelines related to AR have been published both domestically and internationally; however, there are few guidelines specifically targeting children, and non-standardized practices in the diagnosis and treatment of AR, particularly in infants and young children, persist in clinical practice. Accordingly, the Pediatric Otorhinolaryngology Professional Committee of the Chinese Medical Doctor Association’s Pediatric Branch has developed the Clinical Practice Guidelines for the Diagnosis and Treatment of Pediatric Allergic Rhinitis, tailored to national conditions. These guidelines are based on domestic and international AR diagnostic and therapeutic guidelines, recent advances in clinical research, and the clinical expertise of senior specialists in pediatric otorhinolaryngology and pediatric pulmonology. The guidelines outline standardized approaches to the diagnosis and treatment of pediatric AR and aim to provide corresponding guidance to pediatricians, otorhinolaryngologists, and especially primary care physicians.
1 Pathogenesis
Pediatric Allergic Rhinitis is a Type I hypersensitivity reaction primarily mediated by IgE. Its main pathological mechanism involves antigens entering sensitized individuals, triggering the release of inflammatory mediators and the accumulation of inflammatory cells, thereby leading to a series of symptoms.
Most allergens are inhaled allergens, with house dust mites and pollen being the most common. Studies have found that allergic rhinitis (AR) caused by house dust mite allergy can occur in infants as young as 18 months of age. When allergens enter the mucosa, they bind to high-affinity IgE receptors (FcεRI) aggregated on the surface of mast cells in the nasal mucosa, triggering the release of inflammatory mediators (such as histamine and leukotrienes) from mast cells. These mediators stimulate sensory nerve endings and blood vessels in the nasal mucosa and activate the parasympathetic nervous system. This process, known as the early-phase reaction, ultimately leads to symptoms such as nasal itching, sneezing, and watery rhinorrhea. The release of inflammatory mediators, including histamine, induces vascular endothelial cells and epithelial cells to express or secrete adhesion molecules, chemokines, and cytokines, which recruit and activate immune cells such as eosinophils. This results in further release of inflammatory mediators, sustaining and exacerbating the inflammatory response. Significant tissue edema of the nasal mucosa develops, leading to nasal congestion. This process is referred to as the late-phase reaction.
2 Clinical Classification
2.1 Classification by Onset Time of Symptoms (1) Intermittent AR: Symptoms occur <4 days/week, or for <4 consecutive weeks. (2) Persistent AR: Symptoms occur ≥4 days/week, and for ≥4 consecutive weeks.
2.2 Classification by Allergen Type (1) Seasonal AR: Symptoms occur seasonally, with common allergens including seasonal inhalant allergens such as pollen and fungi. Seasonal AR caused by pollen allergy is also known as hay fever. The timing of exposure to seasonal allergens in different regions is influenced by factors such as geographical environment and climatic conditions. (2) Perennial AR: Symptoms occur year-round, with common allergens including indoor perennial inhalant allergens such as house dust mites, cockroaches, and animal dander, as well as certain occupational allergens.
2.3 Classification by Symptom Severity (1) Mild AR: Symptoms are mild and do not significantly affect quality of life (including sleep, daily activities, and learning; hereinafter referred to as the same). (2) Moderate-to-Severe AR: Symptoms are moderate or severe, significantly affecting quality of life.
Classification based on the timing and severity of symptom onset is more applicable to children, according to the characteristics of disease onset.
3 Diagnosis
3.1 Clinical Manifestations
3.1.1 Family History of Allergy A family history of allergic diseases increases the risk of developing allergic rhinitis (AR) in children. If parents suffer from allergic diseases, the risk of their children developing AR is increased by 3.44-fold (OR = 3.44, P < 0.001). The risk of AR is also elevated in pediatric patients with a personal history of allergies (e.g., to animal dander, dust mites, etc.). Therefore, when diagnosing AR in children, clinicians should actively inquire about family history and typical allergy history, and combine this information with clinical manifestations and other diagnostic tests to ensure an accurate diagnosis.
3.1.2 Symptoms The four typical major symptoms of allergic rhinitis (AR) in children are sneezing, watery rhinorrhea, nasal pruritus, and nasal congestion. Infants and young children may present with nasal congestion, which can be accompanied by mouth breathing, snoring, wheezing, feeding difficulties, and nose and eye rubbing. In preschool-aged children, nasal congestion is the predominant symptom, which may be associated with ocular symptoms and cough. In school-aged children, watery rhinorrhea is the predominant symptom, which may be associated with ocular symptoms and epistaxis.
3.1.3 Physical Signs Typical physical signs that may occur during an episode of allergic rhinitis (AR) in children include pale and edematous bilateral nasal mucosa, and watery nasal secretions. Ocular signs mainly consist of conjunctival congestion and edema. Infants and young children often present with eczema and may have comorbid asthma. In addition, the following manifestations may occur: (1) “Allergic shiners” or “panda eyes”: refers to darkening of the lower eyelids due to chronic congestion, with the degree of darkness correlating with the duration and severity of the disease. This sign may be less apparent in young children with AR. (2) “Allergic salute”: refers to the action of rubbing the nose upward with the palm or fingers to relieve nasal itching and improve nasal patency. (3) “Allergic crease”: refers to the transverse wrinkles on the skin of the external nose caused by frequent upward rubbing of the nasal tip.
3.2 Laboratory Testing
3.2.1 Skin Tests Allergen skin testing is an important diagnostic tool for confirming IgE-mediated type I hypersensitivity reactions, referred to as in vivo allergen testing. The primary methods include the skin prick test (SPT) and intradermal testing. SPT demonstrates high sensitivity and specificity, generally exceeding 80%, providing valuable evidence for the diagnosis of allergic rhinitis (AR). This method is clinically recommended for diagnosing AR in children. The use of antihistamines, leukotriene receptor antagonists, or glucocorticoids within two weeks prior to testing may affect the results.
3.2.2 Blood Tests Blood tests mainly involve IgE testing, including serum total IgE and serum specific IgE testing. (1) Serum total IgE testing: Since allergic diseases, parasitic infections, and other factors (such as ethnicity) can increase total IgE levels in the body, total IgE testing has limited diagnostic value for AR. Moreover, approximately one-third of patients with perennial AR have serum total IgE levels within the normal range. (2) Serum specific IgE testing: This refers to in vitro allergen testing, which is suitable for patients of any age and is not limited by skin conditions. It has similar diagnostic performance to SPT, but each has its own characteristics. Typically, a serum specific IgE level ≥0.35 kU/L is considered positive, indicating that the body is in a sensitized state.
In children under 2 years of age, food allergens are the primary cause; serological testing is more feasible in infants and young children.
3.2.3 Detection of Nasal Secretions This includes nasal secretion smears and measurement of allergen-specific IgE in nasal lavage fluid. Nasal secretion smears are stained with Wright’s stain (eosin-methylene blue staining); a proportion of eosinophils >0.05 under high-power microscopy is considered positive. Measurement of allergen-specific IgE in nasal lavage fluid has certain clinical value for the differential diagnosis of allergic rhinitis (AR) in children.
3.3 Other Diagnostic Methods Nasal Provocation Test: A specific allergen is directly applied to the nasal mucosa to observe whether it induces relevant clinical symptoms. Symptoms occurring after the provocation test are recorded and comprehensively evaluated in conjunction with objective examination results to obtain data of value for clinical diagnosis and differential diagnosis. However, this method is rarely used in clinical practice and is primarily employed for research purposes.
3.4 Diagnostic Criteria The diagnostic criteria for pediatric allergic rhinitis (AR) should be established based on the patient’s family history, typical allergy history, clinical manifestations, and consistent laboratory test results. (1) Symptoms: Presence of two or more of the following: sneezing, watery rhinorrhea, nasal itching, and nasal congestion. Symptoms persist daily or accumulate to more than 1 hour per day, and may be accompanied by other associated symptoms such as respiratory symptoms (e.g., cough, wheezing) and ocular symptoms (e.g., ocular itching, lacrimation, conjunctival injection, and burning sensation). (2) Signs: Common findings include pale and edematous nasal mucosa, and watery nasal secretions. (3) Laboratory Tests: Positive result for at least one allergen via skin prick test (SPT) and/or serum-specific IgE testing; eosinophil proportion >0.05 under high-power microscopy in nasal secretions is considered positive.
Given the high rate of negative results from skin prick tests or serum-specific IgE testing in infants and young children, along with the low incidence of non-allergic rhinitis (NAR) in this population, skin prick tests or serum-specific IgE testing are not required as mandatory criteria for diagnosing allergic rhinitis (AR) in infants and young children. A diagnosis can be made based solely on allergy history, family history, and typical symptoms and signs.
4 Differential Diagnosis and Comorbidities
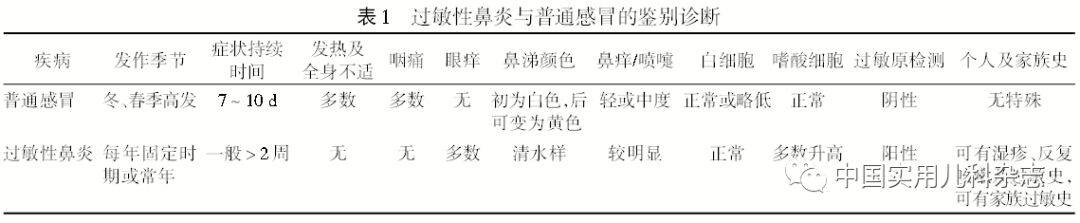
4.1 Common Cold The differential diagnosis with the common cold is shown in Table 1.
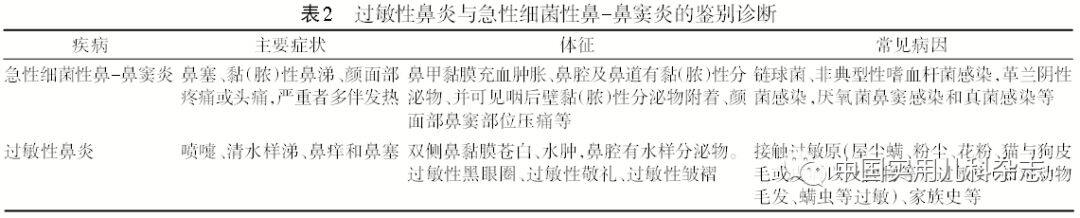
4.2 Acute Bacterial Rhinosinusitis The differential diagnosis with acute bacterial rhinosinusitis is shown in Table 2.
4.3 Other Diseases Causing Nasal Congestion Diseases that can cause nasal congestion include congenital choanal atresia, nasal stenosis, deviated nasal septum, and adenoid hypertrophy. These conditions can be differentiated from allergic rhinitis (AR) through imaging and nasal endoscopy. In particular, for infants and young children, differential diagnoses such as adenoid hypertrophy and structural abnormalities should be considered.
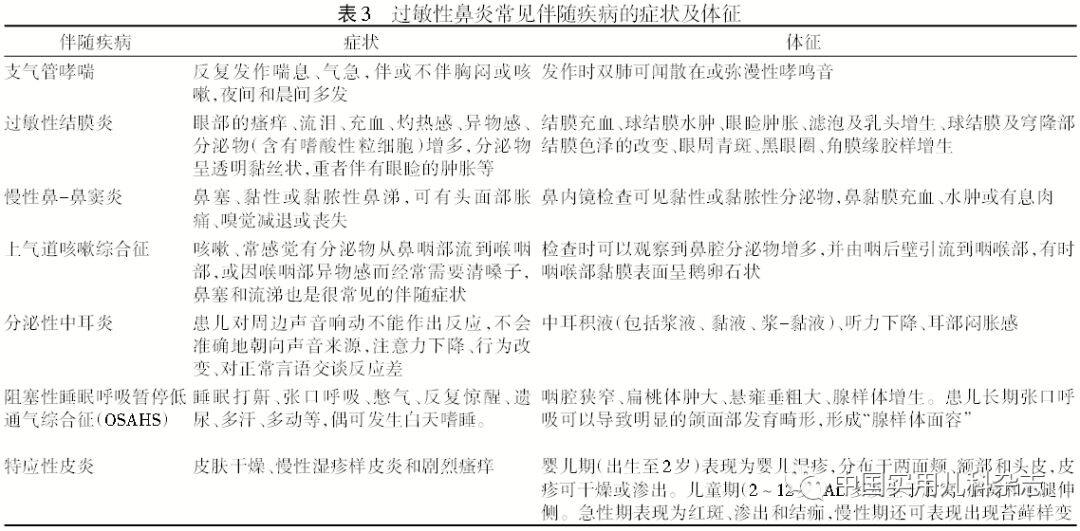
4.4 Common Comorbidities The common comorbidities of AR are shown in Table 3.
5 Prevention and Treatment
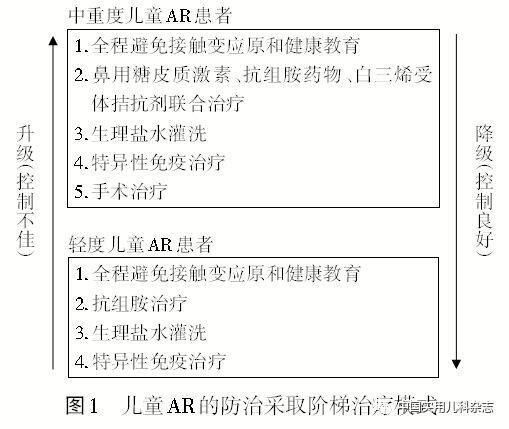
The management of allergic rhinitis (AR) in children requires an integrated approach combining prevention and treatment. The principles of prevention and treatment include environmental control, pharmacotherapy, immunotherapy, and health education. A stepwise treatment model should be adopted for the prevention and management of pediatric AR (see Figure 1).
5.1 Avoidance of Allergen Exposure While outdoor allergens cannot be completely avoided, indoor allergens can be. For pediatric patients with allergic rhinitis (AR) who are frequently exposed to high concentrations of indoor allergens, a multifaceted approach to allergen avoidance is recommended following environmental assessment. For AR patients allergic to pollen, it is advisable to avoid peak periods of allergenic pollen dissemination to reduce symptom exacerbation.
5.2 Pharmacological Treatment Mild intermittent pediatric allergic rhinitis (AR) is treated with antihistamines, while moderate-to-severe intermittent and persistent pediatric AR is managed with combination therapy involving intranasal corticosteroids, antihistamines, and/or leukotriene receptor antagonists.
5.2.1 Antihistamines Histamine is a neurotransmitter with pro-inflammatory effects that is widely present in human tissues. Antihistamines share the ethylamine group with histamine and can bind to H1 receptors, causing the conversion of active receptors to inactive forms, thereby antagonizing the biological effects of histamine.
5.2.1.1 Oral Antihistamines Second-generation antihistamines are first-line therapeutic agents for pediatric allergic rhinitis (AR) and are clinically recommended for the treatment of pediatric patients. These medications have a rapid onset of action and a prolonged duration of effect, significantly improving nasal symptoms such as pruritus, sneezing, and rhinorrhea. They are also effective for concomitant ocular symptoms, but their efficacy in relieving nasal congestion is limited. Generally, once-daily dosing is sufficient, with a treatment course of no less than two weeks. Syrup formulations are recommended for young children under five years of age. Currently, the oral second-generation antihistamines commonly used in clinical practice for pediatric AR are loratadine and cetirizine.
Second-generation oral antihistamines can effectively control mild and some moderate-to-severe intermittent pediatric allergic rhinitis (AR). For children with severe, persistent symptoms, they can be combined with nasal corticosteroids. Antihistamines not only treat allergic diseases but also reduce the frequency of respiratory viral infections and wheezing episodes, playing a crucial role in the secondary prevention of asthma. Oral antihistamines are particularly suitable for children accompanied by eczema and ocular allergic symptoms.
5.2.1.2 Intranasal Antihistamines Intranasal antihistamines have a rapid onset of action and are suitable for pediatric patients with seasonal, perennial, or intermittent symptoms.
5.2.2 Intranasal Glucocorticoids Glucocorticoids exert significant anti-inflammatory, anti-allergic, and anti-edema effects. Their anti-inflammatory action is non-specific, effective against various inflammatory diseases, and capable of sustaining control over the inflammatory response.
Intranasal corticosteroids are the first-line treatment for pediatric allergic rhinitis (AR), providing significant improvement in most nasal symptoms, including sneezing, rhinorrhea, nasal pruritus, and nasal congestion. They are primarily indicated for moderate-to-severe pediatric AR. For moderate-to-severe intermittent pediatric AR, each course of intranasal corticosteroid therapy should, in principle, last no less than 2 weeks. For moderate-to-severe persistent pediatric AR, combination therapy with antihistamines should be administered for more than 4 weeks per course. Proper administration techniques can reduce the incidence of epistaxis; patients should be instructed to avoid directing the spray toward the nasal septum.
5.2.3 Leukotriene Receptor Antagonists Leukotriene receptor antagonists selectively bind to the cysteinyl leukotriene CysLT1 receptor and exert their effects by competitively blocking the biological activity of cysteinyl leukotrienes. They are more suitable for preschool-aged children with severe nasal congestion. For pediatric patients with moderate-to-severe allergic rhinitis (AR), leukotriene receptor antagonists can be used as part of combination therapy, particularly in conjunction with intranasal corticosteroids. A subset of pediatric patients with comorbid asthma may benefit from this medication.
5.2.4 Mast Cell Membrane Stabilizers Mast cell membrane stabilizers are second-line therapeutic agents for pediatric allergic rhinitis (AR) and should be used based on clinical judgment. Among them, sodium cromoglicate and tranilast are more commonly used in clinical practice and have certain efficacy in alleviating symptoms of sneezing, rhinorrhea, and nasal pruritus in children with AR.
5.2.5 Decongestants For pediatric patients with allergic rhinitis (AR) presenting with severe nasal congestion, topical decongestants may be used short-term for no more than 7 consecutive days. Oral decongestants (e.g., pseudoephedrine) are not routinely recommended for the clinical management of AR.
5.2.6 Traditional Chinese Medicine Certain components of Chinese herbal medicines possess anti-allergic, anti-inflammatory, and immunomodulatory effects; among them, geraniol exhibits anti-allergic and anti-inflammatory activities.
5.3 Nasal Irrigation Nasal irrigation with saline or seawater is a safe and convenient therapeutic method, commonly used as an adjunctive treatment for inflammatory conditions of the nose and sinuses. It is particularly suitable for infants and young children and is generally performed before the administration of other intranasal medications. Irrigation with isotonic saline, hypertonic saline, or seawater can remove nasal irritants, allergens, and inflammatory secretions, alleviate nasal mucosal edema, and improve mucociliary clearance function.
5.4 Immunotherapy This therapy is a causative treatment for IgE-mediated type I hypersensitivity disorders, involving the administration of gradually increasing doses of allergen extracts (therapeutic vaccines) to induce immune tolerance in the body. This enables patients to experience significantly reduced symptoms, or even remain asymptomatic, upon re-exposure to the corresponding allergens. Immunotherapy should be selected for patients with a clear history of allergic rhinitis (AR) and positive allergen tests, namely those with allergen-induced AR. Subcutaneous injection reduces compliance and acceptance rates of immunotherapy among school-age and preschool children. The advantages of immunotherapy include modifying the natural course of the disease, controlling symptoms, reducing medication use, decreasing complications such as asthma, and preventing sensitization to additional allergens. Its disadvantages include high costs, potential systemic and local adverse reactions, frequent administration, pain, and slow onset of action.
5.4.1 Subcutaneous Immunotherapy Initiating subcutaneous immunotherapy early in children with allergic rhinitis (AR) is of significant importance for disease prognosis. In addition to marked improvement in nasal symptoms, patients receiving subcutaneous immunotherapy develop significantly fewer new allergen sensitizations compared to those treated with pharmacotherapy alone. Notably, the dosing of different types of allergen vaccines has not been standardized, and their efficacy and safety profiles vary. Therefore, treatment regimens should be individualized based on the child’s clinical condition, with priority given to ensuring treatment safety to avoid systemic and local adverse reactions.
Subcutaneous immunotherapy is not recommended for children under 5 years of age, primarily due to communication difficulties and the invasive nature of immunotherapy injections, which are difficult for younger children to tolerate.
5.4.2 Sublingual Immunotherapy Sublingual immunotherapy is a specific immunotherapy method that administers allergen vaccines via the oral mucosa to gradually induce immune tolerance in patients. Extensive domestic and international clinical studies, as well as systematic reviews and meta-analyses, have confirmed its efficacy and safety for allergic rhinitis (AR) and asthma. Allergen vaccines for sublingual immunotherapy are available in two formulations: drops and tablets. Currently, the only standardized sublingual allergen vaccine available for clinical use in China is the Dermatophagoides farinae drops. Therefore, targeted immunotherapy is not yet available for AR patients sensitized to other types of allergens, such as pollen.
5.5 Surgical Treatment For older children with allergic rhinitis (AR) who do not respond to conservative pharmacological treatment, particularly those with worsening nasal obstruction requiring surgical intervention, bilateral submucosal low-temperature plasma radiofrequency ablation of the inferior turbinates is recommended to alleviate nasal obstruction. Studies have confirmed that low-temperature plasma radiofrequency ablation yields significant therapeutic efficacy in treating perennial pediatric allergic rhinitis. This technique helps reduce postoperative stress responses in children with snoring and allergic rhinitis, improves ventilatory function, and is characterized by minimal trauma, mild pain, rapid recovery, safety, and effectiveness.
6 Health Education
Health education plays a crucial role in the prevention and management system of pediatric allergic rhinitis (AR). Health education for children with AR can be categorized into three aspects: initial consultation education, reinforcement education (follow-up education), and education for families and caregivers. The main content includes: (1) popularization of allergy-related knowledge to help patients understand the etiology, risk factors, disease progression, and potential hazards of AR; (2) informing patients about the necessity of allergen testing and the primary detection methods; (3) guiding patients or guardians on effective environmental control measures to avoid or minimize exposure to allergens; (4) introducing the efficacy, treatment duration, and potential adverse reactions of pharmacological and immunotherapeutic interventions, and providing guidance on medication administration and adjustment of treatment plans.
7 Efficacy Evaluation
The therapeutic efficacy of allergic rhinitis (AR) in children includes both short-term and long-term outcomes. Short-term efficacy is evaluated at the end of treatment (except for immunotherapy), while long-term efficacy is assessed at least one year after treatment completion. For immunotherapy, efficacy evaluation should be conducted after two years of continuous treatment with standardized allergen vaccines.
7.1 Subjective Assessment Before, during, and after treatment, the pediatric patient or their guardian shall conduct self-assessments of relevant symptoms, medication usage, and quality of life. This may be done by maintaining a daily "diary card," from which daily, weekly, and monthly average scores are calculated to reflect the severity of symptoms and the degree of improvement.
7.1.1 Symptom Scoring The primary outcome measures include four nasal symptoms (sneezing, rhinorrhea, nasal itching, and nasal congestion) and two ocular symptoms (ocular itching, foreign body sensation, ocular redness, and lacrimation). If asthma is comorbid, asthma symptom scores for wheezing, coughing, shortness of breath, and chest tightness should be recorded separately. The Visual Analogue Scale (VAS) may be used to evaluate the improvement in individual symptom scores and/or the total scores for nasal, ocular, and asthma symptoms before and after treatment.
VAS: Patients mark their scores for various symptoms on a 0–10 cm scale, which is then evaluated on a scale of 0 to 10, where “0” indicates no symptoms and “10” indicates the most severe symptoms. The VAS scoring method is simple and easy to perform, allowing for quantitative assessment of AR severity.
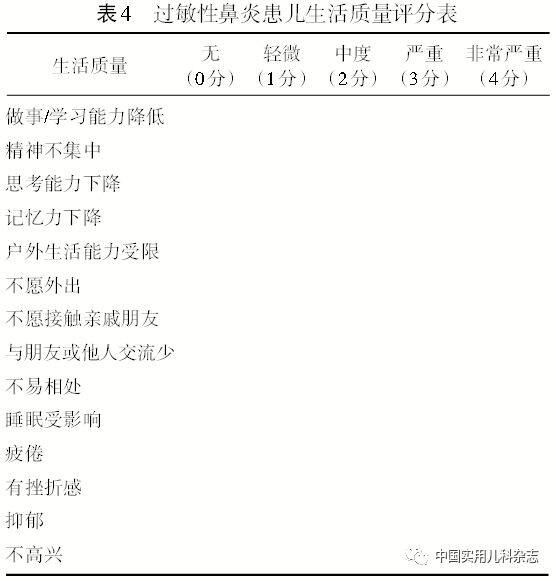
7.1.2 Quality of Life Scores The quality of life scores for pediatric patients are shown in Table 4. This scoring scale is simple and easy to administer. Pediatric patients or their guardians mark the corresponding boxes based on the impact of the disease on daily life over the past 1–2 weeks; a higher score indicates poorer quality of life.
7.2 Objective Evaluation Nasal function tests are used to assess the degree of nasal patency and improvement in nasal obstruction in pediatric patients before and after treatment, demonstrating certain clinical value. (1) Rhinomanometry. (2) Acoustic rhinometry. (3) Nasal endoscopy combined with the Lund-Kennedy scoring system: Endoscopic examination combined with the Lund-Kennedy scoring system and expert clinical experience can serve as an objective scoring method for pediatric allergic rhinitis (AR). The scoring range is 1–10, with higher scores indicating more severe symptoms.
Original Title: Guidelines · Standards · Consensus │ Diagnosis and Treatment of Allergic Rhinitis in Children — Clinical Practice Guidelines