PulseMed Secures Nearly RMB 100 Million in Funding to Advance BIOMAGIC Bioresorbable Coronary Scaffold into First-in-Human Trials

BIOMAGIC
Developer of Implantable Medical Devices
For patients with coronary heart disease, cardiac stent implantation has become the gold standard of treatment. However, post-procedure, patients are required to take anticoagulant medications for life to prevent thrombus formation triggered by the metallic stents within the coronary arteries. Even after physical recovery, many patients continue to experience psychological distress, which adversely affects their daily lives and work.
Therefore, scientists have developed a bioresorbable scaffold that can dissolve spontaneously in vivo and be absorbed by the body. Made from polymeric materials, this scaffold provides vasodilation and structural support to blood vessels in cases of stenosis. Once drug elution is complete and vascular remodeling has occurred, the scaffold gradually degrades and disappears, thereby avoiding the risks of potential long-term local inflammatory responses and thrombosis.
BIOMAGIC specializes in the development of cardiovascular interventional products made from bioresorbable materials. Its first product, the BIOMAGIC sirolimus-eluting bioresorbable coronary stent system, took nearly eight years to develop.The product has entered the green channel for innovative medical devices and recently completed its first-in-human trial.. To gain a better understanding of bioresorbable coronary stents, VCBeat interviewed Miao Yongsheng, founder of BIOMAGIC. Let us take you through the past and present of coronary intervention therapy.
The Past and Present of Percutaneous Coronary Intervention
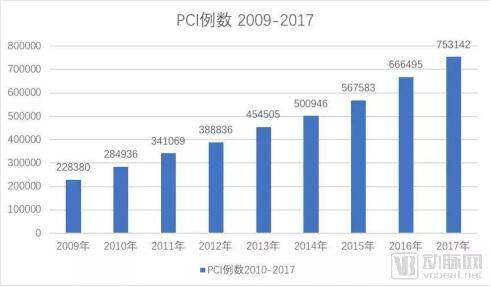
In China, the incidence of coronary heart disease (CHD) has been increasing year by year, and percutaneous coronary intervention (PCI) is the primary treatment modality for CHD. From 2009 to the present, the number of PCI procedures performed in China has continued to rise, with the total number of cases reaching 753,142 in 2017, representing a 13% increase compared to 2016. According to statistics, an average of 427 patients per million population in China undergo PCI treatment.
The “primary weapon” currently used in clinical coronary intervention is the metal drug-eluting stent (DES), known as the third-generation interventional technology. What is its development history? What issues exist with this type of stent?
In 1977, Dr. Gruentzig successfully performed the world’s first balloon angioplasty (i.e., PTCA, commonly known as “balloon dilation”) using a balloon catheter on a patient with proximal stenosis of the left anterior descending coronary artery, ushering in a new era of interventional therapy for coronary heart disease.
During PTCA, the physician advances the balloon at the catheter tip to the site of coronary artery stenosis and then inflates the balloon with fluid under pressure, thereby dilating the narrowed artery. Patients undergoing PTCA experience immediate relief from symptoms of myocardial ischemia.
However, the efficacy of this method was not durable, with over 50% of patients experiencing restenosis within one year. At the time, it was believed that elastic recoil of the vessel lumen led to restenosis. To address this, bare-metal stents (BMS) were invented in the 1980s.
Stent implantation involves delivering a stent pre-mounted on a balloon catheter to the site of coronary artery stenosis. After the balloon is inflated to expand the stent, the stent remains within the vessel, providing continuous and permanent support. However, following the implantation of bare-metal stents (BMS), the incidence of restenosis within one year (known as the restenosis rate) remained as high as over 35%. Further research revealed that the primary cause of restenosis after BMS implantation was not vessel collapse, but rather hyperplasia of vascular smooth muscle cells. This discovery ushered in the third phase of percutaneous coronary intervention: the "era of drug-eluting metal stents."
In 2002, drug-eluting stents (DES) were introduced.Drug-eluting stents (DES) are created by dissolving drugs that inhibit endothelial cell proliferation, such as paclitaxel or rapamycin and its derivatives, into a polymer coating applied to metal stents. The polymer controls the gradual release of the drug from the stent, thereby inhibiting vascular endothelial cell proliferation. The use of drug-eluting stents has reduced the rate of in-stent restenosis to 5-10%.
Subsequently, medical device companies further innovated drug-eluting stents (DES), primarily focusing on improvements in stent design (such as making the stent struts thinner and more flexible), the use of different alloy materials (such as cobalt-chromium or platinum-chromium alloys for the stent platform), the application of different drugs (such as sirolimus derivatives like everolimus and zotarolimus), and various drug-coating materials and technologies (such as single-sided drug coating or coating-free approaches).
Therefore, drug-eluting stents (DES) are primarily used in percutaneous coronary intervention, while bare-metal stents (BMS) are selected only in limited circumstances, such as when patients have a high bleeding risk and cannot tolerate prolonged dual antiplatelet therapy, or when antiplatelet therapy needs to be discontinued shortly after stent implantation to undergo other surgical procedures.
Regardless of the type of metallic stent implanted, it will inevitably impact the original structure and function of the blood vessel, and lifelong anticoagulant therapy is required.Therefore, the development of bioabsorbable vascular scaffolds (BVS) represents another innovation in the history of coronary stent evolution. These scaffolds are fabricated from materials that can be fully degraded within the body (such as polylactic acid). After being implanted for a certain period, they can be completely degraded, leaving no foreign stent material in the body and allowing the blood vessel to restore its "original state."
Ideal BVS Requires the Following Characteristics:It provides sufficient mechanical support to diseased vessels during the early post-implantation phase, does not induce intimal inflammation or hyperplasia after implantation, and yields degradation products that are non-toxic and harmless to the human body (biocompatibility). The degradation rate of the stent matches the time required for autologous repair and remodeling of the vessel at the implantation site (biodegradability). Additionally, it should ideally possess favorable characteristics such as good radiopacity, excellent maneuverability, small outer diameter, and hemodynamic compatibility.。
Currently, poly-L-lactic acid (PLLA) is the most commonly used biomaterial for the fabrication of bioresorbable vascular scaffolds (BVS), owing to its favorable biocompatibility and ultimate degradation into water and carbon dioxide in vivo. The strut thickness of earlier PLLA-based BVS devices typically ranged from 150 to 200 μm.
Miao Yongsheng told VCBeat that if restenosis occurs after DES stent implantation, it is very troublesome to deal with because there is already a metal stent in the blood vessel.However, this issue does not exist with bioresorbable scaffolds, allowing physicians to treat them in the same manner as vessels with primary stenosis. Furthermore, vasodilatory function in vessels implanted with metallic stents is impaired, making it difficult to fully restore normal physiological status.
The world’s first bioresorbable vascular scaffold (BVS) to receive U.S. FDA approval was Abbott’s Absorb GT1. However, sales were discontinued in September 2017, one year after its launch in the United States, due to commercial reasons. In February 2019, Lepu Medical’s bioresorbable stent, NeoVas, received certification from the China Food and Drug Administration (CFDA) and was approved for sale in China.
BIOMAGIC's Bioresorbable Stent
As a latecomer in the field of bioresorbable scaffolds, BIOMAGIC has drawn on the experience gained from earlier generations of products developed by other companies. According to Miao Yongsheng, compared with first-generation BVS, BIOMAGIC’s BIOMAGIC BVS is a new-generation, polylactic acid-based, thin-walled bioresorbable scaffold. It employs novel design and manufacturing processes that further enhance the scaffold’s mechanical properties while reducing its thickness to approximately 130 μm.
Since 2013, BIOMAGIC has completed product development and validation, as well as various biological, physical, and chemical tests, and animal experiments.
In 2017,The company’s products have been admitted to the CFDA “Green Channel for Innovative Medical Devices.” In 2018, it obtained CFDA approval to conduct clinical studies in humans. Phase I human trials are currently underway at Peking University First Hospital, Zhongshan Hospital of Fudan University, and Wuhan Asia Heart Hospital. Phase II, involving larger-scale human trials, is scheduled to commence next year.
BIOMAGIC’s medical technology team boasts extensive experience. Robert, the company’s co-founder, has over 35 years of expertise in product development and management. He previously served as a Senior Product Development Engineer and Project Manager at Boston Scientific, Medtronic, and Abbott, where he directly participated in the development of products representing every milestone in interventional cardiology. The company’s core R&D personnel possess profound expertise in biomaterials, structural mechanics, and the development of bioresorbable stents.
Founder Miao Yongsheng possesses extensive management experience in the medical device industry. After earning his MBA from the University of Chicago Booth School of Business, he joined Johnson & Johnson in the United States, serving as the Marketing Manager for cardiovascular stents in the Hong Kong and China regions. Subsequently, he served as General Manager for Abbott in China, where he led the integration of the Chinese operations of Guidant, a U.S. company acquired by Abbott.
Regarding funding, Miao Yongsheng told reporters that BIOMAGIC has secured nearly RMB 100 million in financing from professional investment institutions.


Zhongshan Hospital, Fudan University, Completes First Human Implantation of BIOMAGIC Bioresorbable Scaffold: The Patient Had a 90% Stenosis in the Proximal Segment of the Left Anterior Descending Coronary Artery, and a 3.0 x 24 mm BIOMAGIC Scaffold Was Implanted. Post-procedural Optical Coherence Tomography (OCT) Imaging Demonstrated Good Scaffold Apposition, Complete Lesion Coverage, and Restoration of Normal Lumen Diameter in the Lesion Segment.