July 29, 2019 News /
BioonBIOON/ -- Bristol-Myers Squibb (BMS) recently announced that the Committee for Medicinal Products for Human Use (CHMP) of the European Medicines Agency (EMA) has issued a positive opinion, recommending approval of the immunostimulatory therapy Empliciti (elotuzumab) in combination with Pomalyst (pomalidomide) and low-dose dexamethasone (EPd regimen), for adult patients with relapsed or refractory multiple myeloma (R/R MM) who have received at least two prior therapies, including lenalidomide and a proteasome inhibitor (PI), and whose disease progressed on or after the last therapy.
Now, the CHMP’s assessment opinion will be submitted to the European Commission (EC), which will take the CHMP’s opinion into consideration and make a final review decision within the next 2–3 months. In the United States,FDAApproved the above indications for the EPd regimen in November 2018.
The CHMP’s positive opinion is based on the favorable data from the Phase II clinical study ELOQUENT-3. This randomized, active-controlled clinical trial evaluated the efficacy and safety of the three-drug regimen EPd versus the standard-of-care two-drug regimen (pomalidomide plus dexamethasone, Pd) in 117 patients with relapsed/refractory multiple myeloma (MM) who had failed at least two prior therapies, including lenalidomide and a proteasome inhibitor (PI). In the study, patients were randomly assigned to receive either the EPd regimen (n=60) or the Pd regimen (n=57) until disease progression or unacceptable toxicity.
Notably, the ELOQUENT-3 study is the first to evaluate the standard of care regimen (pomalidomide and low-dose dexamethasone) with or without a
Monoclonal Antibody Drugsrandomized study. The EPd regimen is also the first three-drug regimen approved based on data from a randomized clinical trial using Pd as the control regimen.
Data show that, compared with the Pd treatment group, the EPd treatment group had a significantly prolonged progression-free survival (PFS) (median PFS: 10.25 months [95% CI: 5.59 months–not estimable] vs. 4.67 months [95% CI: 2.83 months–7.16 months]) and a significant 46% reduction in the risk of progression or death (HR=0.54, 95% CI: 0.34–0.86, p=0.0078). Among patients randomized to the Pd treatment group, the PFS benefit was consistent in those who had previously received 2–3 prior therapies (HR=0.55, 95% CI: 0.31–0.98) and in those who had received ≥4 prior therapies (HR=0.51, 95% CI: 0.24–1.08). In terms of overall response rate (ORR), the EPd regimen was twice that of the Pd regimen (53.3% [n=32/60, 95% CI: 40.0–66.3] vs. 26.3% [n=15/57, 95% CI: 15.5–39.7]; p=0.0029), and a higher proportion of patients achieved a very good partial response or better (20% [n=12] vs. 8.8% [n=5]). Regarding safety, the incidence of serious adverse events was 22% in the EPd regimen group and 15% in the Pd treatment group. Due to
Adverse ReactionsThe discontinuation rates were 5.0% in the EPd treatment group and 1.8% in the Pd treatment group.
In June this year, Bristol-Myers Squibb announced the latest data from ELOQUENT-3 at the 24th Annual Congress of the European Hematology Association (EHA2019). In an unplanned analysis conducted, a descriptive evaluation of overall survival (OS) after extending follow-up for at least 18.3 months showed that patients in the EPd regimen group continued to experience sustained and clinically relevant OS and PFS benefits compared to the Pd regimen group.
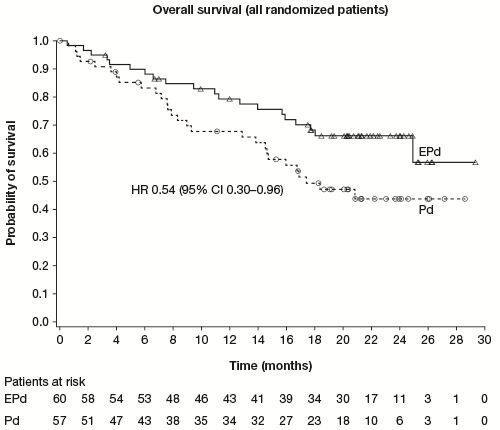
The specific results were as follows: Compared with the Pd regimen group, the EPd regimen group showed a significant 46% reduction in the risk of death (HR=0.54; 95% CI: 0.30–0.96). At 18 months, the overall survival rate was 68% in the EPd regimen group and 49% in the Pd regimen group. At the time of data analysis, the median OS had not been reached in the EPd regimen group (95% CI: 29.4 months–NE), whereas it was 17.4 months in the Pd regimen group (95% CI: 13.8–NE). At 18 months, the progression-free survival rate was 34% in the EPd regimen group and 11% in the Pd regimen group. In this study, the safety profile of the EPd regimen was consistent with that observed in the primary analysis and with previous results for the elotuzumab and pomalidomide regimen.
BMS
TumorFouad Namouni, Head of Development, stated: “The CHMP’s positive opinion further confirms that Empliciti-based combination regimens will help patients with multiple myeloma (MM) who are relapsed or refractory to prior therapies. Given that the majority of MM patients experience disease relapse, there is a particular need for additional treatment options.”
Empliciti was co-developed by Bristol-Myers Squibb and AbbVie, with commercialization activities solely managed by Bristol-Myers Squibb. Empliciti is an immunomodulatory antibody that targets signaling lymphocytic activation molecule family member 7 (SLAMF7, also known as CS1), a glycoprotein expressed on the surface of myeloma cells, as well as on natural killer (NK) cells and plasma cells. Additionally, it is expressed at lower levels in specific immune cell subsets within the hematopoietic lineage differentiation cells.
Empliciti has a dual mechanism of action: (1) Direct activation pathway: It directly activates the immune system via the SLAMF7 pathway through natural killer (NK) cells; (2) Antibody-dependent cellular cytotoxicity (ADCC): Empliciti can target and bind to SLAMF7 molecules on the surface of multiple myeloma cells, marking these malignant cells and enhancing the activity of natural killer cells in killing them through antibody-dependent cellular cytotoxicity. (Bioon.com)




