Glanzmann's Thrombasthenia Moves Towards "Once-a-Month Injection," Hemab Therapeutics' Bispecific Antibody Phase II Data Stuns, Receives FDA Breakthrough Designation

Hemab Therapeutics
Rare Bleeding Disorders Therapeutics Developer
When a hemostatic drug that meets the needs of two core medical scenarios — “prevention + treatment” — receives FDA Breakthrough Therapy Designation, for patients with bleeding disorders, it is no less than a “preventive reassurance.” Administering the drug as an intervention before the “risk of bleeding” escapes from the “black box” writes a new narrative in preventive treatment for bleeding. And sutacimig is the key player in this narrative.
Recently, Hemab Therapeutics, which focuses on the development of innovative preventive therapies for coagulation disorders, announced that its self-developed drug sutacimig has received FDA Breakthrough Therapy Designation (BTD) for the prevention and treatment of bleeding episodes in Glanzmann Thrombasthenia (GT).
1Dual-antibody design holds promise to fill the gap in GT preventive treatment
Glanzmann Thrombasthenia (Glanzmann thrombasthenia, GT), first reported by Glanzmann in 1918, is also known as Glanzmann disease. It is an autosomal recessive inherited platelet dysfunction disorder, clinically characterized by a lifelong bleeding tendency, often involving the skin and mucous membranes, with episodes of disabling and potentially life-threatening severe bleeding.
Results from the international Glanzmann's 360 (GT360) study indicate that 88% of 117 participants reported at least one bleeding episode within a week, and 65% were hospitalized due to bleeding-related issues within six months. These bleeding events significantly impacted patients' mental health and quality of life, butTo date, there is no effective preventive treatment for GT.
GT is caused by quantitative or qualitative mutations in glycoprotein (GP) IIb/IIIa (αIIbβ3) of the platelet membrane, a protein that is crucial for platelet aggregation and coagulation. αIIbβ3 serves as the receptor for fibrinogen on platelets. In normal platelets, fibrinogen binds to αIIbβ3 through a bridging mechanism, triggering aggregation, a necessary step for normal platelet aggregation and subsequent hemostatic plug formation. In GT patients, a defect in αIIbβ3 leads to the absence of fibrinogen-mediated platelet bridging, resulting in platelet dysfunction and manifesting as a severe bleeding phenotype.
Mechanism of action studies suggest that recombinant coagulation factor VIIa (rFVIIa) may function through the synergistic effects of tissue factor (TF)-independent and TF-dependent pathways. In coagulation therapy, research proposes that recombinant coagulation factor VIIa drives the activation of coagulation factor X (FX) on the surface of activated platelets in a TF-independent manner, resulting in an enhanced thrombin burst at the site of vascular injury. Thrombin generation mediated by rFVIIa leads to fibrin formation on activated platelets, subsequently triggering fibrin-dependent but αIIbβ3 receptor-independent platelet aggregation and hemostatic plug formation.
Recombinant factor VIIa has a short systemic half-life (2-3 hours), low subcutaneous bioavailability, and weak affinity for binding to activated platelets. These characteristics collectively indicate that, to treat persistent bleeding, multiple dosing of rFVIIa is required to achieve the target plasma peak concentration. Studies have confirmed,By extending the systemic half-life, enhancing activity, or both, the hemostatic efficacy of rFVIIa can be significantly improved.One strategy to enhance FVIIa activity is to increase its affinity for activated platelets, which can be achieved by localizing FVIIa to receptors on the surface of activated platelets.
Triggering Receptor Expressed on Myeloid Cells-Like Transcript-1 (TLT-1) precisely meets all the aforementioned criteria and is an ideal receptor.TLT-1 as a membrane-bound protein is only present in the intracellular pools of resting platelets and megakaryocytes. Upon platelet activation, TLT-1 redistributes from α-granules to the platelet surface, where it becomes exposed to blood at sites of vascular injury. Studies have shown that conjugating anti-TLT-1 Fab fragments (antigen-binding fragments) with FVIIa significantly enhances the affinity of FVIIa for activated platelets, resulting in a marked increase in its in vivo activity compared to free recombinant FVIIa.
Based on the potential of targeted therapy and the advantages of low-frequency subcutaneous administration, Hemab Therapeutics has adopted an engineered bispecific antibody design to develop sutacimig (HMB-001) through the DuoBody platform. Sutacimig mimics the mechanism of action of rFVIIa to restore hemostatic function but largely relies on the proteolytic activity of endogenous coagulation factor VIIa.
One antigen-binding arm of sutacimig binds to endogenous FVIIa with high affinity. The half-life of sutacimig is much longer than that of endogenous FVIIa. Therefore, after sutacimig binds to FVIIa, it can prolong the half-life of endogenous FVIIa, leading to the continuous accumulation of plasma FVIIa in the circulatory system until a new steady-state level is reached. The other arm of sutacimig binds to the TLT-1 receptor on the surface of activated platelets. When blood vessels are damaged, the expression of TLT-1 on the surface of activated platelets recruits the sutacimig:FVIIa complex to the site of injury. At this point, the FVIIa delivered by sutacimig drives the activation of coagulation factor X (FX), thereby enhancing local thrombin generation and promoting the formation of hemostatic plugs.
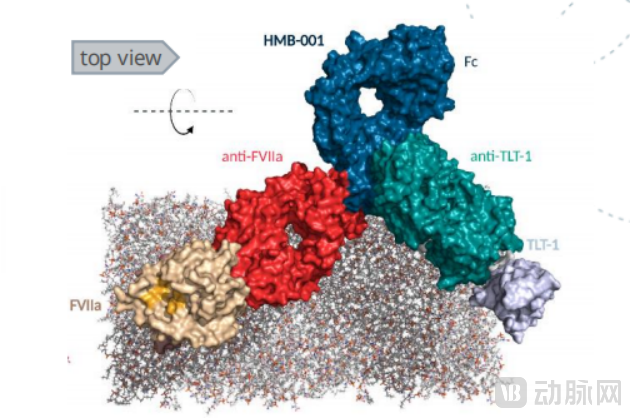
Structural diagram of sutacimig (Source: Hemab Therapeutics official website)
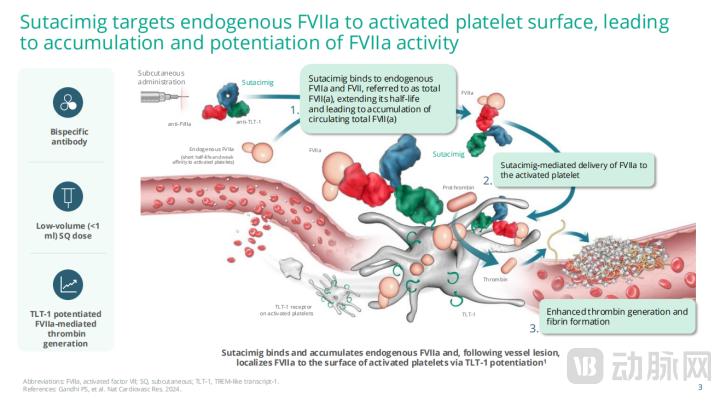
Mechanism of Action of Sutacimig (Source: Hemab Therapeutics)
Overall,Sutacimig innovates on the mechanism of recombinant FVIIa, with its uniqueness lying in acting solely through endogenous FVIIa. It becomes a model for antibody-mediated activation of endogenous protein aggregation and targeted therapeutic intervention, and is expected to become the world's first preventive therapy for Glanzmann's thrombasthenia.
2One Subcutaneous Injection Per Month, Farewell to Hundreds of Infusions
Bleeding management in GT patients is often complicated by the lack of treatment options and evidence-based guidelines. Recommendations for managing minor bleeding include compression, elevation of the affected area, systemic tranexamic acid therapy, and the use of topical antifibrinolytic agents. For major bleeding and surgical interventions, platelet transfusion is one of the optional treatments.
However, platelet transfusions are often difficult to obtain, especially for patients positive for anti-αIIbβ3 antibodies, and carry the risk of alloimmunization, leading to resistance to subsequent transfusions. Recombinant factor VIIa (rFVIIa) has been approved for the management of acute bleeding in GT patients who are unresponsive to platelet transfusions and lack access to platelet resources. While it can effectively control bleeding,Recombinant Factor VIIa, due to its short half-life, requires frequent intravenous infusions, with the number of infusions possibly reaching up to hundreds per year, significantly impacting the patient's quality of life and posing challenges to long-term treatment adherence.
The only potentially curative option available today is allogeneic hematopoietic stem cell transplantation, which, despite its potential for cure, carries a high risk of mortality and morbidity.
On the basis of achieving hemostatic effectiveness, sutacimig has also innovatively upgraded its dosing frequency and administration route.Provide preventive treatment options for subcutaneous administration, with a dosing frequency as low as once a week to once a month.The clinical goal is clear: to improve patient compliance compared to current traditional treatments and alternative treatment options. Notably, HMB-001 is also suitable for bleeding prevention in patients with other rare bleeding disorders.
3Annual total bleeding rate decreased by an average of 100%, significant reduction in severe bleeding events
The breakthrough therapy designation for sutacimig is based on the support of clinical datasets, including positive results from the completed Phase II multi-dose escalation stage of the ongoing HMB-001-CL101 Phase I/II clinical trial.
In a single ascending dose Phase I study, seven patients received subcutaneous doses of 0.2 mg/kg (n=1), 0.5 mg/kg (n=3), and 1.25 mg/kg (n=3), respectively. During the 56-day follow-up period, all subjects tolerated HMB-001 well.
In terms of safety, the most common adverse events (AEs) were mild or moderate. No adverse events or serious adverse events related to HMB-001 occurred. No dose-limiting toxicity or thromboembolic events were reported.
In the multi-dose escalation Phase II trial (N=34), all dose groups significantly reduced the annual total bleed rate (ATBR). In the overall efficacy population (N=31), the mean ATBR was reduced by approximately 50%. The weekly dosing group achieved an estimated 87% reduction in ATBR (95% CI: 80%, 92%). Adverse events were primarily mild to moderate and were either non-specific or common adverse reactions in GT patients.
More importantly, the efficacy was consistent across all major bleeding sites (including nasal, gingival/oral, and gastrointestinal) and demonstrated high effectiveness for both traumatic and spontaneous bleeding events.
The above clinical data collectively reveal one of the core highlights of sutacimig.Significantly and continuously reduces the risk of bleeding, with a marked decrease in severe bleeding events requiring high-intensity treatment (defined as the need for rFVIIa, platelet transfusion, plasma, cryoprecipitate clotting factors, or medical intervention), and an average ATBR reduction of 100%.Of great clinical significance.
It is worth noting that the sample size of current clinical studies on sutacimig does not exceed 100 cases. Further validation of its efficacy and safety still relies on the supplementation of data from larger-scale trials. However, based on the existing clinical study results, Hemab Therapeutics has planned to advance the pivotal Phase III registrational study of sutacimig in 2026.
In addition to the Breakthrough Therapy Designation, the FDA has also granted sutacimig Fast Track Designation and Orphan Drug Designation for the treatment of GT; it has simultaneously received multiple designations from other authoritative regulatory agencies worldwide, including the designation granted by the UK Medicines and Healthcare products Regulatory Agency (MHRA) through the Innovative Licensing and Access Pathway (ILAP) and the Orphan Drug Designation for GT treatment in the European Union.
Current therapies face ongoing challenges in effectively controlling bleeding, while preventive treatment represents an even more difficult hurdle to overcome. The unmet medical needs of patients with Glanzmann's thrombasthenia are evident. Sutacimig’s recent designation as a Breakthrough Therapy by the FDA marks a crucial step forward toward better treatment options in this field.