Darzalex (Daratumumab) Plus Lenalidomide and Dexamethasone Demonstrates Significant Progression-Free Survival Benefit in Transplant-Ineligible Newly Diagnosed Multiple Myeloma: Long-Term MAIA Trial Results
Dec 12, 2019 09:29
CST Updated
09:29

Johnson & Johnson
Healthcare Product Manufacturers, Health Service Providers

Janssen Pharmaceuticals
Pharmaceutical R&D Developer

December 12, 2019 News /Bio ValleyBIOON/ -- The 61st Annual Meeting of the American Society of Hematology (ASH 2019) was recently held in Orlando, Florida, USA. ThisMeetingAt the conference, Janssen Pharmaceuticals, a subsidiary of Johnson & Johnson (JNJ), announced long-term follow-up data from the Phase III clinical study MAIA (MMY3008). The study was conducted in patients ineligible for autologousStem CellsThe study was conducted in patients with newly diagnosed multiple myeloma (NDMM) eligible for autologous stem cell transplantation (ASCT) to evaluate the efficacy and safety of the three-drug regimen Darzalex (daratumumab) combined with lenalidomide and dexamethasone (D-Rd), compared with the two-drug regimen of lenalidomide plus dexamethasone (Rd). The results showed that, compared with the Rd regimen, the D-Rd regimen significantly reduced the risk of disease progression or death and significantly improved the overall response rate (ORR).
MAIA (MMY3008) is a randomized, open-label, multicenter phase III study that enrolled a total of 737 newlyDiagnosiswho are not suitable for high-dose chemotherapy and autologousStem CellsPatients with multiple myeloma eligible for autologous stem cell transplantation (ASCT) (aged 45–90 years; median age, 73 years). In the study, patients were randomly assigned to receive either the three-drug regimen of Darzalex plus lenalidomide and dexamethasone (D-Rd) or the two-drug regimen of lenalidomide and dexamethasone (Rd). In the D-Rd treatment group, patients received Darzalex at a dose of 16 mg/kg: once weekly during cycles 1–2, once every 2 weeks during cycles 3–6, and once every 4 weeks from cycle 7 onwards until disease progression. The primary endpoint was progression-free survival (PFS).
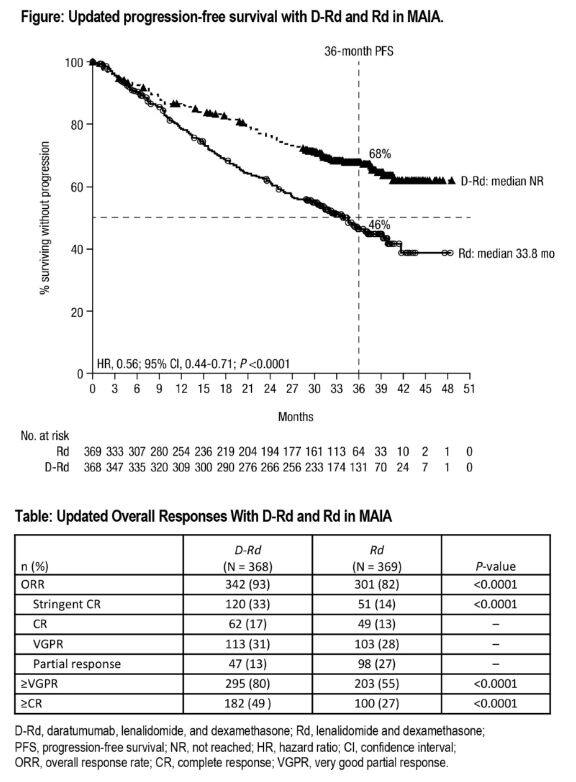
Additional long-term follow-up data (median 36.4 months) presented at this year’s ASH meeting demonstrated that, compared with the Rd regimen, the D-Rd regimen continued to significantly reduce the risk of disease progression or death by ≥44% (HR=0.56; 95% CI: 0.44–0.71; p<0.0001). After three years of follow-up, no new safety concerns emerged in the D-Rd group. Furthermore, time from randomization to next-line treatment or death (PFS2) favored the D-Rd arm (HR=0.69; 95% CI: 0.53–0.91; p=0.0079). Updated overall response rates (ORR) were 93% for the D-Rd group versus 82% for the Rd group (p<0.0001); stringent complete response (sCR) rates were 33% versus 14% (p<0.0001); rates of very good partial response or better (≥VGPR) were 80% versus 55% (p<0.0001); and rates of complete response or better (≥CR) were 49% versus 27% (p<0.0001).
In terms of safety, common grade 3/4 treatment-emergent adverse events (TEAEs) occurring in ≥10% of patients in the D-Rd treatment group compared with the Rd treatment group included: neutropenia (51% vs 35%), lymphopenia (15% vs 11%), pneumonia (15% vs 9%),Anemia(14% vs 21%), leukopenia (11% vs 6%), and hypokalemia (10% vs 10%). The most common serious TEAEs in the D-Rd treatment group compared with the Rd treatment group were pneumonia (14% vs 9%). The incidence of grade 3/4 infections was 36% in the D-Rd treatment group and 27% in the Rd treatment group. Treatment discontinuation due to TEAEs occurred in 9% of patients in the D-Rd treatment group and 18% in the Rd treatment group.

Darzalex is the first CD38-mediated, cytolytic antibody drug approved globally, with broad-spectrum killing activity. It can target and bind to the CD38 molecule, a transmembrane extracellular enzyme highly expressed on the surface of multiple myeloma cells and various solid tumor cells. Through multiple immune-mediated mechanisms of action, it induces rapid death of tumor cells, including complement-dependent cytotoxicity (CDC), antibody-dependent cell-mediated cytotoxicity (ADCC), antibody-dependent cellular phagocytosis (ADCP), and viaApoptosis(apoptosis). In addition, Darzalex has also been shown to targetTumorImmunosuppressive cells in the microenvironment thus exhibit immunomodulatory activity.
Darzalex was licensed by Janssen Biotech, Inc. from Genmab in 2012, granting it exclusive global rights. This drug is a key product heavily developed by Johnson & Johnson. In addition to multiple myeloma, Darzalex also holds potential for treating other types of cancers with high expression of the CD38 molecule.Tumor, including diffuse large B-cell lymphoma (DLBCL), chronic lymphocyticLeukemia(chronic lymphocytic leukemia [CLL]), acute lymphoblastic leukemia (ALL), plasma cell leukemia (PCL), acute myeloid leukemia (AML), follicular lymphoma (FL), and mantle cell lymphoma (MCL), etc.
Darzalex was approved for market launch in November 2015 and has since been approved for multiple therapeutic indications, which vary by country and region, including: (1) Darzalex in combination with bortezomib, thalidomide, and dexamethasone (D-VTd) as a first-line treatment for eligible autologousStem Cells(1) newly diagnosed multiple myeloma (MM) patients eligible for autologous stem cell transplantation (ASCT); (2) Darzalex in combination with lenalidomide and dexamethasone (DRd) as a first-line treatment for newly diagnosed MM patients ineligible for ASCT; (3) Darzalex in combination with bortezomib, melphalan, and prednisone (D-VMP) as a first-line treatment for newly diagnosed MM patients ineligible for ASCT; (4) Darzalex in combination with lenalidomide and dexamethasone, or with bortezomib and dexamethasone, for adult MM patients who have received at least one prior therapy; (5) in combination with pomalidomide and dexamethasone, for adult MM patients who have received at least two prior therapies, including lenalidomide and a proteasome inhibitor (PI); (6) as monotherapy, for adult MM patients who have received at least three prior therapies, including a proteasome inhibitor (PI) and an immunomodulatory drug (IMiD), or who are double-refractory to PIs and IMiDs.
In February this year, a split-dose regimen of Darzalex also receivedFDAApproved. This protocol will allow healthcare professionals to choose, as needed, when treating MM patients, to split the first intravenous infusion of Darzalex from a single one-time infusion into divided intravenous infusions over two consecutive days.
In July this year, the subcutaneous formulation of Darzalex was submitted for marketing approval in the United States and Europe. Phase III clinical study data demonstrated that the subcutaneous formulation of Darzalex was non-inferior to the intravenous formulation in terms of efficacy (overall response rate: 41% vs. 37%; ratio=1.11, 95% CI: 0.89–1.37) and pharmacokinetics (daratumumab trough concentration [Ctrough]: 499 mg/mL vs. 463 mg/mL; ratio=108%, 90% CI: 90%–122%). Additionally, the subcutaneous administration required significantly less time (5 minutes vs. more than 3 hours) and was associated with a lower incidence of infusion-related reactions (13% vs. 35%).
According to Johnson & Johnson’s 2019 performance report, Darzalex achieved sales of $2.168 billion in the first three quarters of this year, representing a 50.4% year-on-year increase. EvaluatePharma, a pharmaceutical market research firm, previously predicted that Darzalex’s global sales would reach $6.033 billion by 2024, positioning the drug as a key product driving Johnson & Johnson’s future growth. (Bioon.com)