OCC 2026 | K-Clip® Shines with Successful Completion of Three Live Demonstrations, Showcasing the Power of Physiological Tricuspid Repair

H&H Healthcare
R&D and Producer of Interventional Medical Devices for Heart Disease

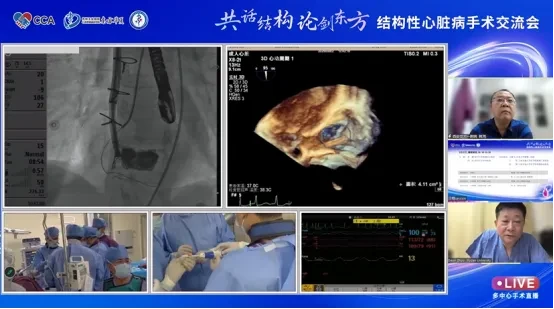
The 20th Oriental Cardiology Conference (OCC 2026) was recently held in Shanghai. Transcatheter tricuspid annuloplasty, as another focal point in the field of interventional therapy for structural heart disease, attracted significant attention at the conference. During the event, HuiHe Healthcare broughtK-Clip®Transcatheter Tricuspid Annuloplasty System, fully demonstrating the significant efficacy and application prospects of “physiological repair” in the treatment of complex tricuspid regurgitation through multi-center surgical demonstrations.
Experts from major medical centers across China engaged in in-depth discussions on surgical strategy formulation, key points of imaging assessment, and instrument operation techniques, providing attendees with rich practical experience through real-time interaction.
Professor Zhou Daxin’s Team
Zhongshan Hospital, Fudan University

Basic Information:78-year-old female
Preoperative Imaging:Ultrasound assessment revealed massive (5+) tricuspid regurgitation, a tricuspid annulus area of 17 cm², and Type IIIc leaflet classification. Preoperative CT assessment showed a tricuspid annulus perimeter of 18.3 cm and an area of 25.9 cm².2, the right coronary artery is偏向房侧 (atrial side), with a minimum systolic distance of 4.6 mm between the TA and RCA; the risk to the coronary arteries during anchoring and clipping is low.
Surgical Strategy:Plan to implant 2 K-Clips
Intraoperative transesophageal echocardiography (Under TEE guidance, at the posterior-septal commissure of the tricuspid valve,At the anterior and posterior junctions, respectivelyImplantation of a 14T and 16T K-Clip resulted in an immediate postoperative reduction of regurgitation from severe (5+) to moderate (2+), demonstrating significant efficacy.
Preoperative Ultrasound
Postoperative Ultrasound
Professor Han Ke's Team
The First Affiliated Hospital of Xi'an Jiaotong University
Basic Information:72-year-old female with intermittent chest tightness and shortness of breath for over 10 years, and lower extremity edema for four months
Preoperative Imaging:Preoperative Assessment ShowsEnlargement of both atria and the right ventricle(Right atrium 42x57mm, right ventricle 42x73mm), TAPSE: 8mm; the tricuspid annulus is slightly enlarged with acceptable opening but poor closure, exhibiting a coaptation gap of approximately 4mm; severe tricuspid regurgitation (4+).
Surgical Strategy:Plan to implant 2 K-Clips
Under the guidance of transesophageal echocardiography, the surgical teamImplantation at the posterior-septal commissure and the anterior-posterior commissure of the tricuspid valve annulus, respectively12T K-Clip, reduces the annulus and increases leaflet coaptation,Immediate postoperative reflux from severe (4+) Decreased toMildDegree (1+),Tricuspid Annular Area13.7 cm² reduced to 7.25 cm². Significant improvement in regurgitation.
Preoperative Ultrasound
Postoperative Ultrasound
Professor Xiang Rui’s Team
The First Affiliated Hospital of Chongqing Medical University
Basic Information:84-year-old male with bilateral lower extremity edema for over 20 days and recurrent fever for 12 days
Preoperative Imaging:Severe tricuspid regurgitation (4+),Tricuspid Annulus Area: 2243 mm²2, significant annular dilation.A coaptation gap of approximately 3 mm in width is visible between the anterior and posterior leaflets of the tricuspid valve,The shortest distance between the right coronary artery and the tricuspid annulus is 2 mm.
Surgical Strategy:Planned implantation of 2 K-Clips
Under transesophageal echocardiography guidance, the surgical team implanted one 16T K-Clip at the posterior aspect of the posterior septum and another at the junction of the anterior and posterior annuli, respectively, avoiding the coronary arteries without causing any impact. Immediately post-procedure, regurgitation decreased significantly from severe (4+) at baseline to trace (1-).
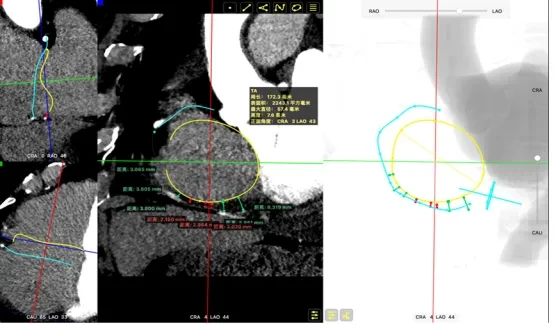
Preoperative CTA: Annulus area 2243 mm²2, minimum distance to coronary artery 2 mm
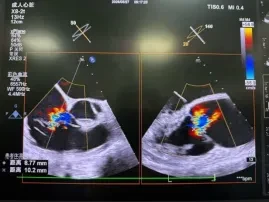

Preoperative Ultrasound:VCW9.5mm,EROA0.47CM2,RVol46ml
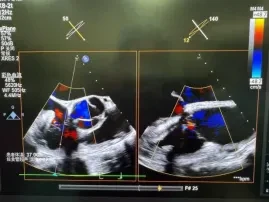

Postoperative Ultrasound:VCW1.1mm,EROA0.06CM2,RVol 6ml
The attending experts unanimously agreed that K-Clip®The key to successful surgery lies in precise preoperative imaging assessment, flexible clipping strategies, and accurate intraoperative manipulation, thereby achieving physiological repair of the tricuspid annulus. The safety of this approach has been confirmed in three high-difficulty cases, with significant efficacy particularly observed in patients with complex anatomy or those at high coronary risk. This technique provides a new and effective option for patients with tricuspid regurgitation who are at high surgical risk, and further long-term follow-up evidence is anticipated to support its widespread application.

K-Clip®Transcatheter Tricuspid Annuloplasty System:
1. Transvascular puncture approach with minimal trauma; sheath outer diameter is 18 Fr.
2. Simple operation, all performed on the atrial side, with a short learning curve.
3. All procedural steps prior to dissociation are reversible, and the surgical outcomes are controllable.
4. Physiological annuloplasty technique, preserving native valve leaflets without damage.