AstraZeneca's Third-Generation EGFR-TKI Tagrisso Achieves 54% Three-Year Survival Rate in First-Line Treatment of EGFR-Mutated NSCLC
Jan 08, 2020 14:13
CST Updated
14:13

AstraZeneca
Biopharmaceutical Manufacturer
January 08, 2020 News /BioValleyBIOON/ -- Recently, the evaluationAstraZenecaThe overall survival (OS) results from the Phase III FLAURA study (NCT02296125) of AstraZeneca’s targeted anticancer drug Tagrisso (Chinese brand name: Tairesha; generic name: osimertinib) as first-line treatment for EGFR-mutated advanced non-small cell lung cancer (NSCLC) were published in the prestigious international medical journal The New England Journal of Medicine (NEJM), under the title:Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC。
The study results showed that, compared with the control EGFR-TKI, Tagrisso treatment group had a longer overall survival (OS). In addition, Tagrisso also increased progression-free survival in patients with central nervous system metastases. Although the exposure time (treatment duration) to Tagrisso was longer, its safety profile was similar to that of the control EGFR-TKI.
FLAURA was a randomized, double-blind study conducted in 556 patients with previously untreated (treatment-naïve) epidermal growth factor receptor (EGFR) mutation-positive (exon 19 deletions or exon 21 L858R mutations) locally advanced or metastatic non-small cell lung cancer (NSCLC). The study evaluated the efficacy and safety of Tagrisso at a once-daily dose of 80 mg compared with standard-of-care EGFR tyrosine kinase inhibitors (TKIs)—Roche’s targeted therapy Tarceva [erlotinib; 150 mg orally once daily] and AstraZeneca’s targeted therapy Iressa [gefitinib; 250 mg orally once daily]—as first-line treatment. The primary endpoint was progression-free survival (PFS), and secondary endpoints included overall survival (OS), objective response rate (ORR), duration of response (DoR), disease control rate (DCR), safety, and health-related quality of life (HRQoL).
Previously reported PFS data demonstrated that the study met its primary endpoint: compared with the gefitinib or erlotinib (previous standard EGFR-TKI) treatment group, the Tagrisso treatment group showed a significantly prolonged median PFS (18.9 months vs. 10.2 months; HR=0.46, 95% CI: 0.37–0.57; p<0.0001). The ORR was similar between the two treatment groups: 80% in the Tagrisso group versus 76% in the standard EGFR-TKI group (odds ratio=1.27, 95% CI: 0.85–1.90; p=0.24). Regarding DoR, the Tagrisso group achieved 17.2 months (95% CI: 13.8–22.0), while the standard EGFR-TKI group achieved 8.5 months (95% CI: 7.3–9.8).
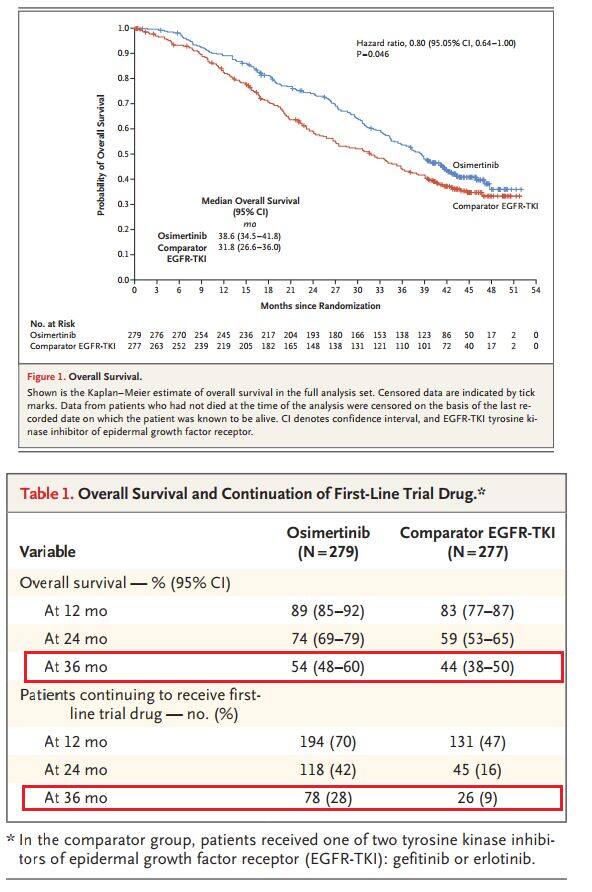
The OS data published in NEJM demonstrate that, compared with the gefitinib or erlotinib group (previous standard EGFR-TKI therapies), the Tagrisso group showed statistically and clinically significant improvements in the key secondary endpoint of overall survival (OS) (median OS: 38.6 months [95% CI: 34.5–41.8] vs. 31.8 months [95% CI: 26.6–36.0]; HR=0.80, 95% CI: 0.64–1.00, p=0.046). After three years of treatment, 28% (n=79/279) of patients in the Tagrisso group and 9% (n=26/277) of patients in the control group were still receiving first-line study treatment, with median exposure durations of 20.7 months and 11.5 months, respectively.
Furthermore, Tagrisso reduced the risk of central nervous system (CNS) disease progression by 52% and prolonged survival without CNS disease progression or death in patients with CNS metastases (HR=0.48, 95% CI: 0.26–0.86, p=0.014). In this study, the safety and tolerability profiles of Tagrisso and standard EGFR-TKIs were consistent with the known properties of each drug; the incidence of grade ≥3 adverse events was 42% in the Tagrisso group and 47% in the control group.
Lung cancer is the leading cause of cancer death in both men and women, accounting for approximately one-fifth of all cancer deaths, surpassingBreast Cancer, the sum of prostate cancer and colorectal cancer. Lung cancer is broadly classified into non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC), with NSCLC accounting for 80–85%.
Approximately 10–15% of NSCLC patients in the United States and Europe, and approximately 30–40% in Asia, have EGFR-mutant (EGFRm) NSCLC. These patients are particularly sensitive to treatment with EGFR tyrosine kinase inhibitors (TKIs), which block the driverTumorgrowth-related cell signaling pathways. Approximately 25% of patients with EGFR-mutant NSCLC present with brain metastases at diagnosis, andDiagnosisincreasing to approximately 40% within two years. The presence of brain metastases typically reduces median survival to less than 8 months.
FLAURAIn the study, the median overall survival (OS) data for Tagrisso exceeding 3 years has established a new benchmark for the clinical treatment of EGFR-mutated NSCLC. These groundbreaking data reaffirm the therapeutic benefits of Tagrisso and further support its use as the standard first-line care for patients with EGFR-mutated NSCLC.
Tagrisso is a third-generation EGFR-TKI that can overcome resistance to first- and second-generation EGFR-TKIs, including Roche/Astellas Tarceva, AstraZeneca Iressa, and Boehringer Ingelheim Gilotrif (afatinib).
Tagrisso inhibits EGFR sensitizing and EGFR T790M resistance mutations, demonstrating clinical activity against central nervous system metastases. To date, Tagrisso 40 mg and 80 mg once-daily oral tablets have been approved in more than 70 countries, including the United States, Japan, and the European Union, for first-line treatment of EGFR-mutated metastatic NSCLC. Additionally, the drug has been approved in more than 80 countries, including the United States, Japan, China, and the European Union, for second-line treatment of advanced NSCLC with EGFR T790M mutation-positive status.
Currently, AstraZeneca is also developing Tagrisso for adjuvant therapy (ADAURA study), locally advanced unresectable disease (LAURA study), in combination with chemotherapy (FLAURA2), and potential new indications (SAVANNAH study, ORCHARD study). (Bioon.com)