When Will a COVID-19 Vaccine Be Available? Insights from the Successful Launch of the Ebola Vaccine

Vir Biotechnology
Developer of Immunological Drugs

Gilead Sciences
Antiviral Drug Developer

Regeneron
Biopharmaceutical Manufacturer

Novavax
Innovative Vaccine Developer

Moderna
mRNA Therapeutics Developer

Inovio Pharmaceuticals
DNA Drug Developer

MSD
Pharmaceutical R&D and Manufacturer

Johnson & Johnson
Healthcare Product Manufacturers, Health Service Providers
Viruses are minute, structurally simple, non-cellular forms of life. They consist solely of a single type of nucleic acid (DNA or RNA) enclosed within a protein capsid. Lacking metabolic machinery, enzymatic systems, intelligence, or emotion, viruses cannot survive outside a host organism. Their sole purpose is reproduction, achieved by parasitizing living cells and generating nearly identical progeny through replication.
In terms of history, viruses have a far longer lineage than humans. Since the emergence of humankind, viruses have been our constant shadow, repeatedly triggering one catastrophic epidemic after another. Regrettably, humanity has almost invariably been on the losing side in its struggle against these pathogens. To date, vaccines remain among our most effective weapons in combating viral diseases.
So, when can we develop a vaccine for the virus causing the current outbreak? VCBeat (WeChat ID: Vcbeat) has reviewed the five major global viral infectious diseases of this century, as well as the development process of the Ebola vaccine, which was successfully brought to market from scratch. Perhaps we can draw our own conclusions.
The Five Major Infectious Diseases of This Century
2003 Severe Acute Respiratory Syndrome (SARS)
The first documented case of the disease later known as “atypical pneumonia” appeared on November 16, 2002, in Foshan City, Guangdong Province, China. As this was a previously unseen disease with symptoms distinct from those of typical pneumonia, it was named atypical pneumonia in China. The World Health Organization (hereinafter referred to as WHO) named it Severe Acute Respiratory Syndrome, abbreviated as SARS.
SARS subsequently swept across China with unprecedented speed—from April to May 2003, more than 6,000 new cases were reported within two months. The disease spread not only in China but also to other regions worldwide. In light of this, in April 2003, the World Health Organization (WHO) declared the outbreak, which was concentrated in China, Vietnam, parts of Canada, and Singapore, a Public Health Emergency of International Concern (hereinafter referred to as PHEIC).
By June 2003, the outbreak had gradually come under control, and on June 24, the WHO announced that it would no longer classify this outbreak as a PHEIC.
On July 13, 2003, the number of confirmed and suspected SARS cases worldwide ceased to increase. According to WHO statistics, as of August 7, 2003, a total of 8,422 confirmed cases and 916 deaths had been reported across 32 countries and regions globally, resulting in a case fatality rate of 10.87%.
In the spring of 2003, the Ministry of Science and Technology urgently launched a scientific and technological campaign to prevent SARS, initiating the development of vaccines against the SARS coronavirus. On May 22, 2004, four volunteers received an inactivated whole-virus SARS coronavirus vaccine developed and evaluated by the Institute of Laboratory Animal Science, Chinese Academy of Medical Sciences, at China-Japan Friendship Hospital. This was the world’s first inactivated whole-virus SARS coronavirus vaccine.
Subsequently, 36 additional volunteers began the immunization trial process. On December 5, 2004, the results of the Phase I study of the inactivated SARS vaccine were announced, revealing that all vaccinated participants had produced antibodies. However, due to the subsequent disappearance of the SARS coronavirus, further clinical research could not proceed, and the project was ultimately canceled.
2009 H1N1 Influenza
On April 15, 2009, the U.S. Centers for Disease Control and Prevention (CDC) identified a novel influenza A virus in samples submitted from a 10-year-old patient in California. This virus was later named the influenza A (H1N1) virus. It rapidly spread across the United States and quickly disseminated worldwide.
Studies have found that the genome of the influenza A(H1N1) virus is a reassortment of the genomes of North American swine-lineage H1N1 and Eurasian swine-lineage H1N1 influenza viruses; hence, it is also referred to as “swine flu.”
On April 25, 2009, the WHO declared the outbreak a Public Health Emergency of International Concern (PHEIC). Subsequently, on June 11, 2009, the WHO raised the influenza pandemic alert level to Phase 6. This marked the first time since 1968 that the WHO had raised the disease pandemic alert level to Phase 6.
The outbreak swept across 75 countries and regions, ultimately ending in April 2010.
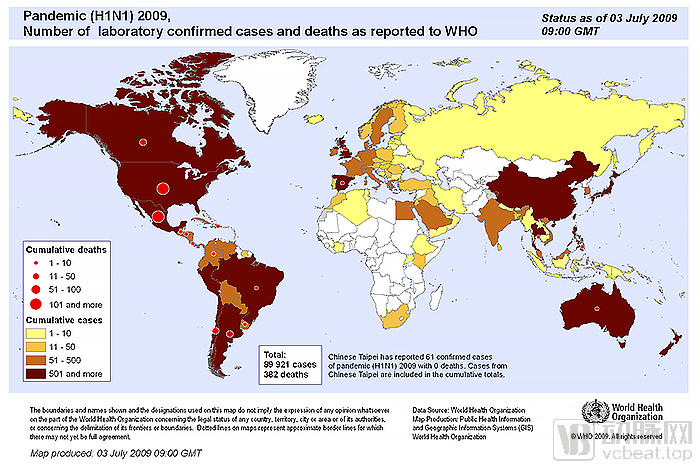
2009 H1N1 Virus Impact Scope (Image from WHO)
Due to the vast number of infections, which precluded individual case counting, the U.S. Centers for Disease Control and Prevention (CDC) could only provide estimates through mathematical modeling: From April 12, 2009, to April 2010, there were 60.8 million (range: 43.3 million–89.3 million) confirmed cases in the United States, nearly 274,000 (range: 195,000–402,000) hospitalizations, and 12,469 (range: 8,868–18,306) deaths. During the first year of viral spread, approximately 151,700 to 575,400 people worldwide died from this pandemic influenza.
On April 21, 2009, the U.S. Centers for Disease Control and Prevention (CDC) began developing virus strains for vaccine production and rapidly selected the vaccine virus strain for manufacturing, submitting it to countries worldwide and the World Health Organization (WHO). As influenza vaccine production technology had been well-established for many years, vaccines against the influenza A(H1N1) virus were promptly produced.
On September 2, 2009, the State Food and Drug Administration approved China’s first influenza A (H1N1) vaccine. On September 7, the first batch of qualified vaccine products ready for immunization was released. On September 8, the Ministry of Health announced that China had become the first country in the world to deploy the influenza A (H1N1) vaccine.
During this epidemic, rPT-PCR technology was also widely applied. Through nucleic acid testing using test kits, doctors can quickly confirm whether patients are infected with the virus. This has since become a powerful technological tool in humanity’s fight against viruses.
Ebola Virus in 2014 and 2018
The Ebola virus is a rare pathogen that causes Ebola hemorrhagic fever, currently the most lethal viral hemorrhagic fever. Patients ultimately succumb to systemic hemorrhaging, resulting in a gruesome demise.
Ebola virus is classified as Biosafety Level 4 (BSL-4). The incubation period ranges from 2 to 21 days, typically lasting 5–10 days. The virus exhibits low transmissibility in the early stages and is not airborne; it is primarily transmitted through bodily fluids. Among these, blood, excreta, and vomit from infected patients are highly infectious, while other bodily fluids also pose a certain risk of transmission. However, live virus has not yet been detected in patients’ sweat.
Ebola virus disease is primarily endemic, confined to the tropical rainforests of Central Africa and the tropical savannas of Southeastern Africa. The lack of adequate medical equipment and hygiene training in these regions constitutes the primary source of transmission.
In February 2014, a large-scale Ebola virus outbreak began in West Africa, primarily concentrated in Guinea, Liberia, and Sierra Leone, posing a serious threat to neighboring countries. On August 8, 2014, the WHO declared the outbreak a Public Health Emergency of International Concern (PHEIC).
As of June 9, 2016, when the outbreak in Liberia was declared over, there were a total of 28,646 confirmed cases and 11,323 deaths worldwide. The vast majority of these cases were concentrated in three countries: Guinea, Liberia, and Sierra Leone.
On May 8, 2018, a new Ebola virus outbreak emerged in the northwestern region of the Democratic Republic of the Congo. On July 24, the World Health Organization (WHO) declared the end of the outbreak, which had resulted in 53 confirmed cases and 17 deaths.
On August 5, 2018, a new round of the epidemic broke out in the country. On July 17, 2019, the WHO declared this outbreak a Public Health Emergency of International Concern (PHEIC). As of January 28, 2020, there were 3,302 confirmed cases and 2,242 deaths.
On November 11, 2019, Merck’s Ebola vaccine Ervebo (rVSV∆G-ZEBOV-GP, also known as V920), a live-attenuated vaccine, received approval from the European Commission, marking the first regulatory authorization for this vaccine. On December 21, the U.S. Food and Drug Administration (FDA) approved the vaccine in the United States.
2015–2016 Zika Virus
Zika virus was first discovered in East Africa in 1947. It is a virus primarily transmitted by Aedes mosquitoes, and can spread between humans through blood, mother-to-child transmission, and sexual contact. The main clinical manifestations include maculopapular rash, fever, and joint and muscle pain. Zika virus poses a significant threat to infants. Studies have shown that pregnant women infected with the virus are at a greatly increased risk of giving birth to infants with microcephaly and other neurological abnormalities.
Prior to the recent outbreaks, Zika virus cases occurred only sporadically worldwide. In May 2015, an outbreak of Zika virus was identified in Brazil, triggering a large-scale epidemic across South America that subsequently spread to 59 countries and regions globally. In February 2016, the World Health Organization (WHO) declared this outbreak a Public Health Emergency of International Concern (PHEIC).

Zika Virus Affected Areas (Image from WHO)
According to statistics, from May 2015 to February 2016, Brazil reported 1.5 million confirmed cases, with over 4,000 infected pregnant women giving birth to infants with microcephaly. On November 18, 2016, the WHO announced the end of the PHEIC.
In February 2016, the WHO announced that 15 companies and research groups were conducting research on Zika virus vaccines. Among them, DNA vaccines from the United States and inactivated vaccines from India were relatively more advanced. However, to date, vaccine development has not yet been completed. Meanwhile, there is still no specific therapeutic drug for the Zika virus.
In addition to conventional measures such as improving sanitation and spraying insecticides, the WHO has also adopted other strategies to reduce viral transmissibility, such as using biological methods to eliminate the virus within Aedes aegypti mosquito populations.
Wolbachia is a bacterium that can inhibit the growth and replication of viruses such as dengue and Zika within mosquitoes. When Wolbachia-infected mosquitoes mate with wild mosquitoes, they can transmit Wolbachia to the next generation, thereby first eliminating these viruses from the mosquito population.
According to research, this bacterium poses little harm to humans. Although native Aedes aegypti populations do not carry this bacterium, its ecological impact is minimal, as it is found in more than 60% of common insects, including butterflies, fruit flies, and certain mosquito species.
Since September 2014, researchers have released 12,000 to 15,000 Wolbachia-infected male mosquitoes weekly into the Tubiacanga and Jurujuba suburbs of Rio de Janeiro over a 20-week period, and repeated this intervention one year later. Trial results indicated that this approach is promising, effectively facilitating the spread of Wolbachia-infected mosquitoes, thereby reducing the sources and routes of Zika virus transmission.
2012 and 2015 Middle East Respiratory Syndrome
In June 2012, Saudi Arabia identified a respiratory disease caused by an unknown coronavirus, which resulted in fatalities. This novel coronavirus, known as MERS, is believed to be transmitted by camels. It continued to spread across the Middle East in the following years and erupted in 2014, with confirmed cases reported in 12 countries and regions worldwide.
The outbreak was largely brought under control in 2015. As of May 10, 2015, Saudi Arabia had reported 976 confirmed cases and 376 deaths. From July 9, 2013, to June 17, 2015, the WHO convened its Emergency Committee and held nine meetings on the Middle East Respiratory Syndrome Coronavirus (MERS-CoV), but never declared the outbreak a Public Health Emergency of International Concern (PHEIC).
Starting with the identification of the first confirmed case on May 20, 2015, South Korea also experienced a MERS outbreak. The World Health Organization (WHO) declared the end of the outbreak on December 23, 2015. A total of 186 confirmed cases and 38 deaths were reported in South Korea.
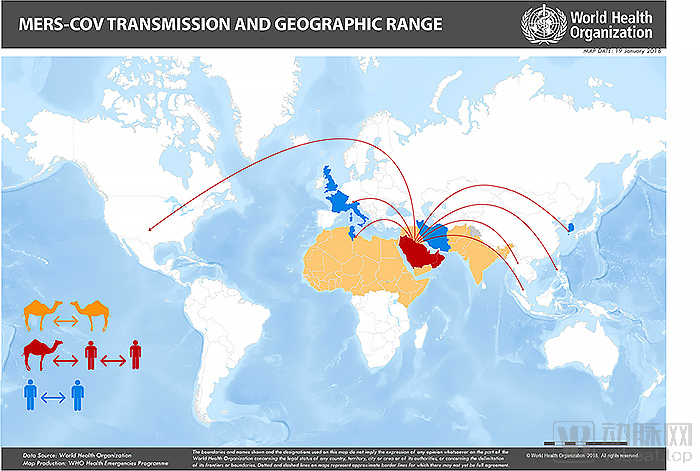
MERS Transmission Range (Image from WHO)
Sporadic cases of Middle East Respiratory Syndrome (MERS) are reported annually. From April 2012 to November 2019, there were a total of 2,494 confirmed cases and 858 deaths worldwide.
After seven years of research and development, MERS vaccine development has finally yielded certain results. In September 2019, The Lancet Infectious Diseases published a research paper reporting the results of the first Phase I clinical trial of GLS-5300, a DNA vaccine against the Middle East Respiratory Syndrome coronavirus (MERS-CoV), demonstrating its safety and efficacy. Currently, four MERS vaccines are undergoing Phase I clinical trials.
How Was the Ebola Vaccine, Marked by Numerous Setbacks, Developed?
An examination of the vaccine development progress for the five major infectious diseases of this century reveals that only vaccines against the H1N1 influenza A virus and Ebola virus are currently available. For influenza viruses, a highly mature system is already in place, enabling rapid market launch. In contrast, Ebola vaccine development had to start from scratch, making its progress more accurately described as fraught with twists and turns.
In the spring of 2014, as the Ebola virus erupted in West Africa, a scientist named Gary Kobinger was closely monitoring news from Canada.
Gary Kobinger is the head of the Special Pathogens Section at the National Microbiology Laboratory in Winnipeg, Canada. The Winnipeg laboratory has been dedicated to Ebola vaccine research for many years, and this vaccine has demonstrated remarkable efficacy in animal studies.
Gary Kobinger’s team even developed a human vaccine and hoped to obtain approval for clinical trials. However, as of April 2014, the vaccine had never undergone clinical testing—given that Ebola was primarily endemic in impoverished African regions, no major pharmaceutical companies were interested in developing such a vaccine.
Upon witnessing the rapid spread of the Ebola virus in Guinea, a country lacking an infectious disease control and prevention system, Koberg contacted the World Health Organization (WHO) to offer vaccine assistance. However, the WHO rejected this proposal.
“They believe it is still too early to move forward,” Koberger said, noting that the WHO had informed him Guinea lacked the infrastructure necessary to approve the use of experimental vaccines. “That is indeed true.”
For years, scientists studying the Ebola virus have been fully dedicated to developing vaccines and therapeutics to combat these deadly scourges. However, this work of immense significance to humanity has hit an insurmountable wall. Pharmaceutical companies face no realistic prospect of recouping their R&D costs; meanwhile, Ebola outbreaks occur only sporadically, offering little opportunity to rigorously test experimental vaccines.
However, viruses clearly do not confine their devastation to a single location as humans might wish. If not contained in a timely manner, they will inevitably become a nightmare for all of humanity. Dr. Heinz Feldmann, the predecessor of Kobinger and leader of the Ebola vaccine development effort, believes that the 2014 Ebola outbreak made people realize that this virus poses a significant threat to humanity.

Ebola Virus Under Electron Microscopy
Like many scientific advances, the success of the Ebola vaccine also began with a flash of inspiration and a bit of luck.
In the early 1990s, John "Jack" Rose of Yale University attempted to use vesicular stomatitis virus (VSV), an animal virus, as a vaccine vector. Although VSV can infect humans, it is harmless to the human body. The human immune system responds to VSV very rapidly, thereby inducing surprisingly high levels of antibodies.
Rose believed that if genes from other viruses were added to VSV, the harmless virus would teach the immune system to recognize harmful potential invaders, thereby becoming a cornerstone of vaccine development. However, after approximately six years, the experiment still had not succeeded.
In 1994, Rose learned that researchers in Germany had successfully performed this procedure. Following this approach, Rose’s team incorporated proteins from a certain influenza virus into VSV and successfully administered vaccination in mice. In the same manner, other laboratories worldwide, including Rose’s laboratory, began to use VSV as the backbone for experimental vaccines against avian influenza, measles, Zika, and other pathogens.
Unfortunately, researchers were unable to study the Ebola virus due to the lack of high-containment laboratories required for handling hazardous viruses. Nevertheless, Rose believed that VSV could also play a role in the development of an Ebola vaccine.
Yale University patented Ross’s VSV vector and licensed it to Wyeth Pharmaceuticals. Ross estimates that the VSV vector has been shared with at least 100 laboratories worldwide, including the Marburg Laboratory in Germany.
In 1967, staff at the Marburg laboratory were infected with an unknown virus via imported Ugandan green monkeys, which was later named the Marburg virus. Nine years later, scientists traced the Marburg virus to discover the Ebola virus, which also belongs to the Filoviridae family.
Subsequently, under the guidance of his mentor Hans-Dieter Klenk, Heinz Feldmann, then a researcher at the Marburg Laboratory, began in-depth research on filoviruses and employed Rose’s VSV system.
Feldman’s team replaced the protein on the surface of vesicular stomatitis virus (VSV), known as glycoprotein (also referred to as G protein), with the glycoprotein of the Ebola virus. Later, the group further substituted VSV’s glycoprotein with that of the Marburg virus. As the team lacked access to high-containment laboratories for animal studies, they were unable to test the potential of using these chimeric VSV viruses as vaccines against Ebola or Marburg viruses.
At that time, Canada was constructing a new National Microbiology Laboratory, namely the National Microbiology Laboratory in Winnipeg. This facility included a Biosafety Level 4 (BSL-4) laboratory, the highest containment level, capable of meeting the safety requirements for Ebola virus research. In 1999, Feldman was hired to lead the Special Pathogens Team at the National Microbiology Laboratory in Winnipeg. With Klenk’s approval, he brought VSV with him.
After arriving in Canada, Feldman believed that Dr. Gary Nabel (then Director of the Vaccine Research Center at the U.S. National Institutes of Health) held incorrect views regarding the Ebola virus. Nabel had posited that the glycoprotein was responsible for the extensive damage caused when the Ebola virus infects animals and humans.
Also sharing Feldman’s view was Tom Geisbert, an Ebola virus expert then serving at the U.S. Army Medical Research Institute of Infectious Diseases.
Feldman and Geisbert believed they could collaborate to demonstrate this using the VSV vector.
At the Winnipeg laboratory, Feldman’s team conducted experiments on mice using a vesicular stomatitis virus (VSV) vector expressing the Ebola glycoprotein. If Nabel’s theory were correct, this recombinant VSV would have caused disease in the mice. However, the animals remained unharmed.
The research team then exposed the mice to the Ebola virus. They found that all mice not previously exposed to the VSV virus died, whereas those infected with VSV carrying the Ebola virus glycoprotein remained unharmed.
With the support of the Winnipeg laboratory, Geisbert subsequently agreed to conduct studies in non-human primates, such as monkeys, which are considered the optimal animal model prior to human clinical trials. The good news is that monkeys vaccinated with the VSV-based mixed virus did not become infected with the Ebola virus.
In 2005, a paper on this study was published in Nature Medicine. It suddenly became apparent that the modified VSV vector loaded with the Ebola glycoprotein was not only safe but could also serve as a foundation for vaccine development.
However, the cost of developing a vaccine is approximately $1 billion. The pharmaceutical industry has little interest in producing a vaccine that prevents a virus appearing only occasionally in poor countries. By 2005, the Ebola virus had caused approximately 1,300 deaths.
“No one was interested in Ebola,” Feldman recalled. He simply went to the bar next door, had a beer, and then continued working.
In 2008, Feldman left the Winnipeg Laboratory to become the head of the Virology Program at the Rocky Mountain Laboratories of the National Institutes of Health (NIH) in the United States.
In March 2009, an unexpected crisis served as a catalyst. A German researcher accidentally punctured three layers of protective gloves with a needle containing the Ebola virus while conducting an experiment. Although there was no bleeding from the wound, her skin had been breached.
She was sent to the University Medical Center Hamburg, where German authorities urgently contacted Ebola researchers in the United States and Canada to explore potential solutions.
Ebola experts and field workers on the other side of the globe agree that the VSV vaccine should be administered as soon as possible. Although it remains unclear whether it will produce the same effects in humans as observed in animal studies, it is still better than doing nothing and waiting for death.
The Canadian government hastily dispatched “vaccines.” Of course, these were merely materials produced by laboratories for animal studies and did not even qualify as formal vaccines.
Approximately 48 hours after the incident, the researcher received the vaccine. The following day, she developed a fever. Fever is not an uncommon reaction to live-virus vaccines such as rVSV-ZEBOV and is, in fact, a sign of immune system activation. Of course, fever can also be the initial symptom of Ebola virus infection. As a precaution, doctors decided to transfer her to a specially constructed biological isolation treatment unit.
Encouragingly, after her fever subsided, she did not exhibit any obvious symptoms of Ebola virus infection. It is difficult to determine whether the vaccine was effective or if she had not actually been infected; Feldmann and others believe that the latter scenario is more likely. Nevertheless, this incident at least demonstrates that the vaccine has no adverse effects in humans, thereby alleviating concerns about its use in future emergency situations.
Beyond scientists, funding is also indispensable for vaccine research and development. The $2 million grant provided by the Canadian Defense Program to the Winnipeg laboratory, though a drop in the bucket, was nevertheless critical. After all, the project had been unable to secure funding.
This project, funded by the Department of National Defence of Canada, supports research into tools for combating bioterrorism. The grant will be used to produce and test large quantities of human-grade VSV vaccines targeting the Zaire ebolavirus species.
The German contract manufacturer IDT Biologika was selected to produce the vaccine. However, the Winnipeg laboratory had to manufacture the starting materials required for vaccine production. In this context, it is essential to mention Judie Alimonti, a humble immunologist who single-handedly oversaw the production of these materials and conducted testing and quality control on IDT’s final product.
“Judy did it. ... I think she spent two years on it, alone,” recalled Korbinger. “She devoted all her energy to this work, which was actually quite monotonous and tedious.”
Alimonti died of cancer in 2017, and her former colleagues called her the unsung hero of the Ebola vaccine.
After securing patents for its vaccine platform and obtaining a license from Wyeth Pharmaceuticals to use the platform for producing vaccines against Ebola and other hemorrhagic fever viruses, the Winnipeg laboratory engaged in negotiations with various pharmaceutical companies, both large and small, to identify development partners.
The only company of interest is BioProtection Systems, a small firm spun off from the cancer vaccine biotechnology company NewLink Genetics.
This has nothing to do with the Ebola virus and infectious disease vaccine platform (which BioProtection Systems will license). It is simply a business decision to enhance the investment portfolio in order to attract funding.
Unexpectedly, it turned out to be a major deal.
The company agreed to pay the Canadian government, the official holder of the viral vaccine patents, approximately $156,000 for the development of each product. An amendment several years later increased this amount to approximately $360,000. Although the Canadian government could theoretically receive revenue from patent sales, these patents were never expected to generate any significant benefits.
The company was later merged into Lumos Pharma and then shelved, until the Ebola outbreak erupted in Guinea, West Africa, in 2013.
The outbreak may have begun in late 2013 and spread rapidly. By March 23, 2014, the WHO had recorded 49 cases and 29 deaths; the following day, an additional 86 cases and 59 deaths were reported. Soon afterward, investigators confirmed cases in an urban setting for the first time, while neighboring Liberia and Sierra Leone also began to face emergencies, leading to a rapid deterioration of the situation.
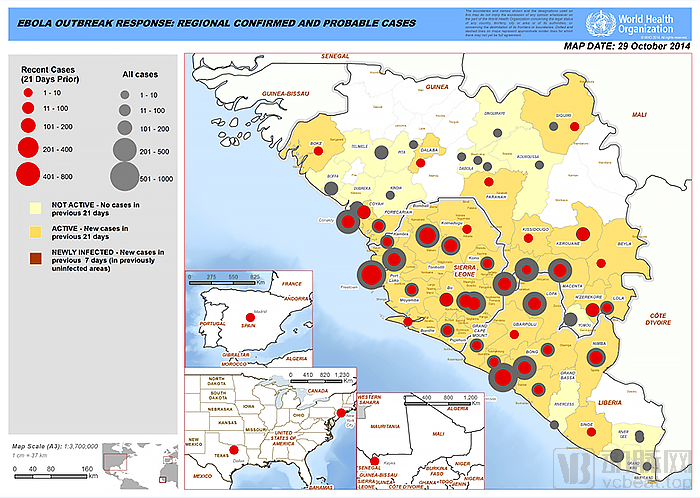
2014 Ebola Virus Affected Areas (Image from WHO)
Witnessing this human tragedy, Koberg offered vaccines to the WHO, but was rejected. A few weeks later, GlaxoSmithKline (GSK), which was developing an Ebola vaccine, also provided vaccines to the WHO, but was likewise rejected.
Kobinger proposed the idea of distributing vaccines to Dr. Armand Sprecher, an Ebola virus expert at Doctors Without Borders, who is a staunch advocate of the VSV vaccine. At Sprecher’s urging, Doctors Without Borders began promoting the use of the VSV vaccine.
On August 8, 2014, the WHO declared the outbreak a global public health emergency. A few days later, the Canadian government announced it would donate vaccines to the organization.
However, it was widely considered unethical at the time to use untested drugs or vaccines in Africa. Clinical safeguards were often lacking locally, and memories of the 1996 medical incident in which Pfizer’s use of a meningitis drug led to the deaths of 11 children remained vivid.
The WHO convened a meeting and concluded that, given the significant threat posed by the Ebola virus, it was “ethically imperative” to attempt experimental vaccines and therapies. The meeting also determined that clinical trials must first assess safety and appropriate dosing. Clearly, NewLink, the holder of the vaccine license, lacked the expertise and capacity required for this task.
Researchers from the U.S. National Institutes of Health and the Walter Reed Army Institute of Research (WRAIR) have begun planning Phase I clinical trials to determine the appropriate vaccine dosage. Other researchers have also initiated trials in Switzerland, Germany, Gabon, and Kenya.
The WHO and other relevant agencies began seeking partnerships with more experienced pharmaceutical companies or opting to purchase vaccines from NewLink.
Reliable partners are scarce, and Sanofi Pasteur is not interested; Novartis has already sold its vaccine division to GlaxoSmithKline (GSK), which is accelerating the testing of its own experimental Ebola vaccine; Johnson & Johnson’s vaccine arm, Janssen, is also developing a vaccine, but it is less mature than those from GSK or Newlink. Only Merck Sharp & Dohme (MSD) has experience in producing vaccines using the cell types employed in the VSV-based vaccine.
Exploratory negotiations began in October 2014, and it took only one month until November 2014, when Merck (MSD) announced its agreement to pay NewLink Genetics $50 million for the manufacturing license of the rVSV-ZEBOV vaccine. This pace is considered exceptionally fast in pharmaceutical deals.
Meanwhile, researchers from the National Institutes of Health and the Walter Reed Army Institute of Research have also reached an agreement on the appropriate vaccine dosage. The situation appears to be improving.
As the saying goes, good things take time. Koberg suddenly discovered that there were significant changes in key characteristics between the vaccine initially used for trials and the final vaccine product.
Since its earliest iterations, the vaccine has been formulated using the glycoprotein from the Zaire ebolavirus strain (Mayinga). However, the human vaccine manufactured by the German contractor IDT Biologika contains glycoproteins from a different strain of the Zaire ebolavirus.
Kobinger’s investigation revealed that Alimonti, who prepared materials for IDT Biologika, used a different type of glycoprotein under the direction of a supervisor. No one noticed that the vaccine tested in humans was not identical to the vaccine that had been thoroughly studied in animals.
Kobinger promptly sent an email to the U.S. Food and Drug Administration (FDA) but received no response. Although clinical trials had already been conducted, Kobinger urgently shipped a new batch of vaccines to Feldman as a precautionary measure, enabling him to test them on monkeys to ensure that this change would not compromise the vaccine’s efficacy.
While researchers analyze data from Phase I and II clinical trials, others are preparing for the pivotal Phase III clinical trials, which will determine whether the vaccine is truly effective.
Meanwhile, logistics and storage issues also need to be considered. Due to the lack of sufficient time typically required to develop heat-stable formulations, rVSV-ZEBOV requires refrigeration in an ultra-low temperature environment below -80℃ to -60℃. This is an impossible task in African regions with scarce power grids and extreme heat, posing a challenge no less difficult than vaccine development itself.
The good news is that Bill Gates, who recognized this issue many years ago (yes, the Bill Gates you know), has been recruiting partners worldwide through Global Good, a research institution he invested in, to collaboratively develop a portable and powerful vaccine storage device. They found Aucma, based in Qingdao, China.
-80℃ to -60℃ ultra-low temperatures mean that the vacuum strength of each tank must be at least 100 times that of ordinary vacuum containers. Meanwhile, the built-in ice block insulation property requires the equipment to have perfect thermal insulation, achieving optimal performance in all three heat transfer methods: radiation, conduction, and convection.
In 2010, Global Good identified a space-grade thermal insulation material capable of protecting spacecraft under extreme temperature conditions for use in thermal barrier layers, thereby addressing some of the challenges.
Both parties encountered difficulties in manufacturing a key component designed to minimize the reverse transmission of cooling capacity from within the equipment—the bimetallic ring located inside the cavity. Experts from both sides determined that a composite material of stainless steel and aluminum alloy was the most suitable option; however, these two materials are among the most difficult to weld together. Ultimately, after repeated research and development efforts, the objective was achieved through the aggressive technique of explosive welding.
In 2014, Global Good and Aucma finally collaborated to manufacture a cold-chain storage device named Arktek for conventional vaccines. This beer-keg-sized device was strapped to camel backs, traversing scorching deserts to reach epidemic areas. In the event of a power outage, it could store vaccines at 2°C–8°C for over a month using just one batch of ice packs, thereby meeting the needs of a community of approximately 6,000 people.
In 2015, Arktek underwent another upgrade—the device can maintain an ultra-low temperature freezing environment of -80°C to -60°C for up to 120–144 hours in the event of a power outage, thereby resolving the transportation issues associated with the V920.

Healthcare workers retrieve vaccines from Arktek (Image source: Arktek.org)
Back in 2014, the U.S. National Institutes of Health had already reached an agreement with Liberia to test GlaxoSmithKline’s vaccine and Merck’s VSV vaccine. Meanwhile, the U.S. Centers for Disease Control and Prevention would test these vaccines in Sierra Leone.
Guinea also hoped to participate in clinical trials, but the country’s weak health infrastructure lacked the capacity to conduct them. The WHO was compelled to announce that the trials would be carried out in Guinea with the assistance of Médecins Sans Frontières (Doctors Without Borders).
The plan adopts a “ring vaccination” strategy. Individuals who have had direct contact with Ebola patients, as well as their contacts, will be vaccinated. This approach not only protects individuals in the chain of transmission but also helps curb the spread of the virus.
The study participants were randomly assigned to two control groups: one receiving immediate vaccination and the other receiving vaccination after a 21-day delay. If more infection cases occurred in the group with the 21-day delayed vaccination, it would indicate that the vaccine was effective.
This method differs from classical trials. In classic experiments, participants are randomly selected to receive either the drug or a placebo, with neither the researchers nor the participants aware of whether the actual drug or the placebo is being administered. Ultimately, empirical evidence is obtained through blinded testing.
In June, the Data and Safety Monitoring Board for the trial concluded that it was unlikely that sufficient additional cases would accrue to alter the study results. The vaccine is indeed effective.
Starting from 10 days post-vaccination (the time required for the immune system to respond to the vaccine), no further cases occurred among those who received immediate vaccination, whereas new cases emerged in the group with delayed vaccination. Therefore, the Data and Safety Monitoring Board recommended that healthcare workers should be vaccinated as soon as possible after identification of Ebola infection.
On July 31, 2015, less than a year after the Canadian government donated the vaccine, The Lancet published the trial results: within a period of less than 12 months, a total of 12 clinical trials were conducted, ranging from first-in-human dose-finding studies to Phase III clinical trials. Prior to this, Guinea had never undertaken clinical trials on such a large scale; this represented an extraordinary scientific and logistical achievement.
The trial in Guinea was the only one to reach a conclusion; the trials conducted in Sierra Leone and Liberia were terminated early due to insufficient patient enrollment.
Although everyone wants an effective Ebola vaccine, there has been intense debate over whether adaptive design studies are sufficient to demonstrate the efficacy of MSD’s vaccine.
Almost simultaneously with the release of the experimental results, some argued that this was not a study but merely a randomized controlled trial. Both the findings and the methodology have been criticized and continue to be questioned by experts to this day. In 2017, the U.S. National Academies of Sciences, Engineering, and Medicine released a report on research conducted during the Ebola virus outbreak, raising doubts about the trial’s methods and results.
The report suggests that the vaccine may provide “substantial protection” to vaccinated individuals, as indicated in preliminary reports; however, the magnitude of its efficacy remains uncertain. In fact, the vaccine’s effectiveness could be quite low, or even nil.
The trial found the vaccine to be 100% effective. However, the number of participants in the trial was limited, and no vaccine is effective in every instance. Nevertheless, this was sufficient to persuade Merck & Co.’s vaccine R&D team.
Merck’s plan has received support from the Biomedical Advanced Research and Development Authority (BARDA), an agency under the U.S. Department of Health and Human Services. BARDA began funding rVSV-ZEBOV during the West African Ebola outbreak and has spent approximately $175 million to support vaccine production and to validate Merck’s vaccine manufacturing facility in Germany.
In the spring of 2018, when the Ebola virus broke out in the Democratic Republic of the Congo, the country agreed to use the vaccine under a “compassionate use” protocol. A “compassionate use” protocol is an agreement that allows unapproved therapies to be used in clinical trials.
Eight days after the outbreak was declared, the Democratic Republic of the Congo began vaccination campaigns, with more than 260,000 people vaccinated.
November 11, 2019,rVSV∆G-ZEBOV-GPIt received approval from the European Commission, marking the first time the vaccine had been authorized by a regulatory agency. On December 21, the FDA approved the vaccine in the United States.
Beth-Ann Coller, the project lead at Merck Sharp & Dohme (MSD), is another unsung hero of this vaccine. She was moved to tears upon its approval, saying, “We are thrilled and proud.”
If luck holds, the 2019-nCoV vaccine could be completed in as little as 16 weeks
Not long ago, Regeneron Pharmaceuticals, based in New York, received a cardboard box containing a single reagent vial. Inside the vial was a fragment of the genetic code of 2019-nCoV (the novel coronavirus). Rest assured, this is merely a small segment of the complete genome and therefore poses no risk of infection.
These materials are not difficult to obtain nowadays; biotechnology companies can acquire them simply by paying synthetic genome suppliers. This is now the standard process for developing biopharmaceuticals, which is fundamentally no different from buying snacks on an e-commerce platform. Of course, you cannot purchase them on JD.com or Tmall.
Star pharmaceutical company Gilead Sciences has shipped remdesivir to China for clinical trials to assess its efficacy in curbing the virus.
In addition, multiple pharmaceutical companies have responded swiftly, attempting to develop vaccines against the 2019-nCoV virus. Besides Regeneron and Gilead Sciences, Johnson & Johnson, Moderna, Inovio Pharmaceuticals, Novavax, and the San Francisco-based startup Vir Biotechnology are also developing vaccines.
Although traditional vaccine preparation is time-consuming, past experience suggests that vaccines can be developed in as little as 16 weeks.
However, developing drugs and vaccines during the initial phase of an epidemic is extremely difficult, as insufficient leads often render most of these efforts futile. A key reason is that interventions effective in laboratory mice frequently fail in humans.
Therefore, Regeneron has been attempting to genetically engineer mice to possess a fully functional human immune system. In this way, once researchers inject foreign substances into the mice, their immune systems will produce human antibodies, which will significantly alter the trajectory of drug development. Regeneron’s eczema drug Dupixent and cancer immunotherapy Libtayo were developed using this approach.
If this approach proves effective, Regeneron’s transgenic mice may help us develop a vaccine for the 2019-nCoV virus as quickly as possible.
According to a paper published in the top academic journal Nature on February 3, on December 26, 2019, the Shanghai Public Health Clinical Center routinely collected a specimen from a patient with fever of unknown origin as part of its research project, sourced from Wuhan Central Hospital and the Wuhan Center for Disease Control and Prevention.
In the early hours of January 5, 2020, the research team detected a novel SARS-like coronavirus from clinical specimens and obtained its complete genome sequence through high-throughput sequencing (GenBank: MN908947).
On January 11, the research team published the full genome sequence of the novel coronavirus on the Virological website (virological.org), becoming the first team globally to release the viral sequence. This milestone was critical for subsequent tracing and identification of the novel coronavirus.
On January 14, the WHO officially named the virus causing this outbreak of pneumonia as the 2019 Novel Coronavirus (2019-nCoV).
Like SARS and MERS, 2019-nCoV is also a coronavirus that utilizes its surface spike proteins to invade host cells and cause infection. Therefore, any definitive treatment must prevent these proteins from reaching their targets.
After studying the viral genome sequence, Regeneron’s R&D team decided to focus on 10% of the approximately 30,000 base pairs of 2019-nCoV. Within a short period, the team cloned the genetic code encoding the spike protein and used it to modify the surface of originally harmless viral particles, creating a pseudovirus.
This pseudovirus can mimic the cell-penetrating biology of 2019-nCoV, but it does not self-replicate or cause disease.
Subsequent work will involve the use of transgenic mice. Scientists at Regeneron will immunize the mice using pseudoviruses bearing spike proteins, thereby generating antibodies that can block the entry of this coronavirus into cells.
This process is estimated to take several weeks and may generate thousands of antibodies with slight variations. Subsequently, researchers will screen each antibody to isolate the most effective ones. These antibodies will then undergo Phase I clinical trials, which are animal studies.
Meanwhile, researchers also select backup antibodies that target the same epitope but do not compete with each other, thereby increasing the likelihood that the vaccine will remain effective despite viral mutations.
In the face of a severe epidemic, pharmaceutical companies that develop viral vaccines first will gain a significant advantage, while latecomers will likely be forced to exit the market. Of course, this premise hinges on the successful completion of development; historically, vaccine development has been far more likely to fail than to succeed, with failed R&D efforts resulting in total loss. Furthermore, as was the case with SARS vaccine development, the epidemic may end before the vaccine is fully developed, leaving pharmaceutical companies with substantial unrecoverable losses.
Given the enormous risks involved, why are so many still flocking to this field? While saving humanity is certainly one factor, pharmaceutical companies are clearly not charities—as evidenced by the tumultuous development process of Ebola treatments. It is precisely China’s vast market and purchasing power that provide sufficient incentive for these companies to act swiftly.
However, there is no need to stigmatize commerce in the context of disease. We must acknowledge that it is precisely due to commercial forces that pharmaceutical companies are willing to assume these significant risks. The development of commerce has enabled it to play a more powerful and diversified role in combating the epidemic, not only by providing financial and material support but also by leveraging its own business models and technological capabilities.
Meanwhile, we should draw a more profound lesson from history: reverence for nature. After all, humanity is truly insignificant in the face of nature.
Stay strong, Wuhan! Stay strong, China! Stay strong, humanity!
Fortune China: A Brief History of the Struggle Between Business Power and Epidemics
Fortune China, January/February 2019: “Minus Eighty Degrees”
Everbright Securities: “A Century of Pandemics: What Has Changed? — The Fifth in the Macroeconomic Analysis Series on Pandemics”
STATNEWS.com:“Against all odds”: The inside story of how scientists across three continents produced an Ebola vaccine
STATNEWS.com:How fast can biotech come up with a vaccine for the latest outbreak?
WHO:Summary table of SARS cases by country, 1 November 2002 - 7 August 2003
WHO:MERS Situation Update November 2019
"Health Times," January 13, 2005: Unveiling the Development of China's SARS Vaccine
STATNEWS.com:In the race to develop a coronavirus treatment, Regeneron think it has the inside track
Nature:A new coronavirus associated with human respiratory disease in China
PR Newswire:Coronavirus (2019-nCoV): The Facts
Clinical Infectious Diseases: Estimating the burden of 2009 pandemic influenza A(H1N1) in the United States(April 2009- April 2010)
CDC: Ten years of gains: A look back at progress since the 2009 H1N1 Pandemic