Roche’s Risdiplam, the First Oral Therapy for SMA, Demonstrates Significant Motor Function Improvement in Phase III SUNFISH Trial for Type 2/3 Patients
Feb 07, 2020 14:48
CST Updated
14:48

Roche
Oncology Drug Research, Development, and Manufacturing

February 07, 2020 /Bio ValleyBIOON/ -- Roche recently announced one-year data from Part 2 of the Phase III SUNFISH trial for risdiplam, an oral medication for spinal muscular atrophy (SMA), at the 2nd International SMA Science and Clinical Conference held in Evry, France. SUNFISH is the largest placebo-controlled trial ever conducted in patients with Type 2 or Type 3 SMA (aged 2–25 years). The study population in Part 2 represented a broad, real-world SMA population. The results showed that after one year of treatment, patients receiving risdiplam demonstrated significant improvements in motor function compared to those in the placebo group. Notably, SUNFISH is the first placebo-controlled trial to include adult SMA patients, confirming that risdiplam improves or stabilizes motor function.
Risdiplam is a splicing modifier of the survival motor neuron 2 (SMN2) gene, developed for the treatment of all types (Type 1, Type 2, and Type 3) of spinal muscular atrophy (SMA). Currently, this drug is under review by the U.S.FDApriority review, with the agency expected to make a review decision this May. If approved, risdiplam will become the first oral medication for the treatment of all three types of SMA.
SUNFISH is a two-part, double-blind, placebo-controlled pivotal clinical study conducted in pediatric and young adult patients (aged 2–25 years) with type 2 or type 3 spinal muscular atrophy (SMA). Part 1 determined the dose for the confirmatory Part 2, with exploratory endpoints assessing efficacy. Part 2 is a large-scale, placebo-controlled trial evaluating risdiplam in patients with type 2 or type 3 SMA.
The results showed that after one year of treatment, patients in the risdiplam group demonstrated significant improvements in motor function compared with the placebo group, achieving clinically and statistically significant outcomes for both the primary and key secondary endpoints. For the primary endpoint, the change from baseline in the Motor Function Measure (MFM-32) score was significantly greater in the risdiplam group than in the placebo group (mean difference: 1.55 points; p=0.0156). For the key secondary endpoint, patients in the risdiplam group also showed improvement in upper limb function as measured by the Revised Upper Limb Module (RULM) compared with the placebo group (difference: 1.59 points; p=0.0028).
As expected, exploratory subgroup analyses demonstrated the strongest response to risdiplam versus placebo in the youngest age group (2–5 years), with 78.1% versus 52.9% of patients achieving an increase of ≥3 points on the MFM-32 scale. Importantly, disease stabilization was observed in the 18–25-year age group (57.1% versus 37.5%, with stabilization defined as an increase of ≥0 points), which represents a treatment goal for patients with more advanced disease.
The safety profile of risdiplam in this study was consistent with its known safety profile, and no new safety signals were identified. The adverse event profile of risdiplam was similar to that of placebo. To date, more than 400 patients have received risdiplam treatment across multiple trials, with no treatment-related safety findings leading to discontinuation from any trial.
Eugenio Mercuri, MD, Chief Investigator of the SUNFISH study and from the Department of Pediatric Neurology at the Catholic University of Italy, stated: “risdiplam is the first potential therapy to obtain key placebo-controlled data in a broad population of patients with SMA, including children, adolescents, and adults. The data indicate that risdiplam can maintain and potentially improve patient independence by enhancing motor function in patients with type 2 or non-ambulatory type 3 SMA.”
Levi Garraway, M.D., Chief Medical Officer and Global Head of Product Development at Roche, stated: “We are highly encouraged by the positive results achieved in this broad SMA patient population, many of whomClinical Trialsunderrepresented. These studies help us understand which measurement indicators are most relevant to patients and the importance of stabilizing the condition for patients with diagnosed diseases.”
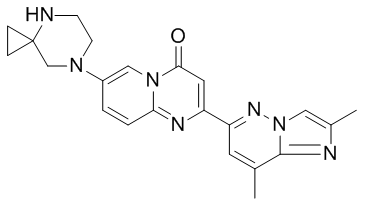
Chemical Structure of Risdiplam (Image Source: medchemexpress.cn)
Risdiplam is an oral liquid, a survival motor neuron 2 (SMN2) splicing modifier designed to continuously increase and maintain SMN protein levels in the central nervous system and peripheral tissues. Growing clinical evidence indicates that SMA is a multisystem disease, and the loss of SMN protein may affect many tissues and cells beyond the central nervous system. Following oral administration, risdiplam exhibits systemic distribution, sustainably increasing SMN protein levels in both the central nervous system and peripheral tissues, and has demonstrated improvement in motor function in patients with Type 1, Type 2, and Type 3 SMA.
As part of its collaboration with the SMA Foundation and PTC Therapeutics, Roche led the clinical development program for risdiplam. The company is conducting four global, multicenter clinical studies—SUNFISH (NCT02908685), FIREFISH (NCT02913482), JEWELFISH (NCT03032172), and RAINBOWFISH (NCT03779334)—to evaluate the efficacy and safety of risdiplam in treating all types (Type 1, Type 2, and Type 3) of spinal muscular atrophy (SMA), as well as presymptomatic SMA in neonates.
In November 2019, the U.S. Food and Drug Administration (FDA) accepted the New Drug Application (NDA) for risdiplam and granted it Priority Review, with a Prescription Drug User Fee Act (PDUFA) target action date set for May 24, 2020. Previously,FDARisdiplam has been granted orphan drug designation and fast track designation. If approved, risdiplam will become the first oral medication for the treatment of all three types of SMA.
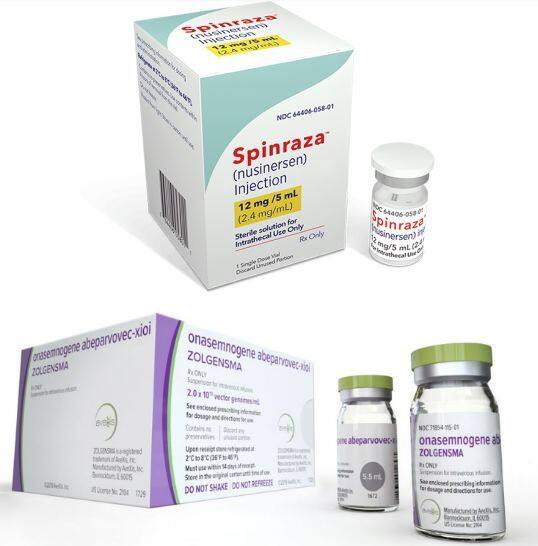
SMA Treatment: Two drugs have been approved globally, with Spinraza receiving approval in China in February 2019
Spinal Muscular Atrophy (SMA) is a motor neuron disease that causes muscle weakness and atrophy. It is an autosomal recessive genetic disorder caused by genetic defects, affecting muscles throughout the patient's body. Patients primarily present with generalized muscle wasting and weakness, progressively losing various motor functions, including breathing and swallowing. SMA is the leading cause of death in infants under the age of two.GeneticsSMA Killer: This disease is a relatively common "rare disease," with an incidence rate of 1 in 6,000 to 1 in 10,000 among newborns. According to relevant reports, there are currently approximately 30,000 to 50,000 SMA patients in China.
In December 2016, Spinraza (nusinersen), a drug developed by Biogen and its partner Ionis, was approved, becoming the first therapy worldwide for spinal muscular atrophy (SMA). This medication is an antisense oligonucleotide (ASO) administered via intrathecal injection, delivering the drug directly into the cerebrospinal fluid (CSF) surrounding the spinal cord. It modulates the splicing of SMN2 pre-messenger RNA (pre-mRNA), thereby increasing the production of full-length functional SMN protein. In patients with SMA, insufficient levels of SMN protein lead to the degeneration of motor neuron function in the spinal cord. Clinical studies have demonstrated that treatment with Spinraza significantly improves motor function in SMA patients.
May 2019, fromNovartisThe gene therapy Zolgensma (onasemnogene abeparvovec) was approved, becoming the world’s first gene therapy for the treatment of spinal muscular atrophy (SMA). Administered as a single, one-time intravenous infusion, the drug enables sustained expression of the SMN protein to halt disease progression, addresses the root cause of SMA, and holds promise for long-term improvement in patients’ quality of life.
In the Chinese market, Spinraza was approved in late February 2019 for the treatment of patients with 5q spinal muscular atrophy (5q-SMA). This approval made Spinraza the first drug for treating SMA in the Chinese market. 5q-SMA is the most common type of SMA, accounting for approximately 95% of all SMA cases. This type of SMA is caused by mutations in the SMN1 (survival motor neuron 1) gene on chromosome 5, hence the name 5q-SMA. (Bioon.com)