Merck's Ervebo, the World's First Ebola Vaccine, Approved in Four African Countries for Prevention of Zaire Ebolavirus
Feb 15, 2020 13:45
CST Updated
13:45

MSD
Pharmaceutical R&D and Manufacturer
February 15, 2020 News /BioonBIOON/ -- Merck & Co. recently announced that the first four African countries, including the Democratic Republic of the Congo (DRC), have approved its Ebola vaccine Ervebo (rVSV∆G-ZEBOV-GP, V920, a live-attenuated vaccine). Ervebo was first approved in the European Union on November 11, 2019, and in the United States on December 20, 2019, for active immunization to prevent Ebola virus disease (EVD) caused by Zaire ebolavirus in individuals aged 18 years and older.
Ervebo is the first Ebola vaccine to receive regulatory approval globally, marking a historic milestone. It should be noted that the duration of protection provided by Ervebo is unknown, and the vaccine does not protect against other species of Ebola virus or Marburg virus. The efficacy of the vaccine when used concurrently with antiviral medications, immune globulin (IG), and/or blood or plasma transfusions is unknown.
The initial approvals in four African countries signify continued, groundbreaking progress toward strengthening global public health preparedness against Zaire ebolavirus disease. This achievement was facilitated by an unprecedented collaboration among the World Health Organization (WHO), the African Vaccine Regulatory Forum (AVAREF), African governments, the European Medicines Agency (EMA), and Merck Sharp & Dohme (MSD). These approvals result from the successful implementation of WHO’s strategic roadmap for introducing and rolling out MSD’s rVSV-ZEBOV Ebola vaccine in African countries. The roadmap aimed to coordinate actions and contributions related to the licensing and deployment of Ervebo, enabling near-parallel regulatory reviews and leading to vaccine approval in several at-risk countries within 90 days of WHO prequalification.
Kenneth C. Frazier, Chairman and Chief Executive Officer of MSD, stated: “We thank the World Health Organization for its leadership in paving the way for accelerated prequalification and licensure of this vaccine in the countries at greatest risk. This important milestone is another example of the partnerships formed to respond to the outbreak. Although our fight against Ebola is far from over, this milestone demonstrates what we can achieve when we work together to tackle the most challenging diseases threatening people and communities.”
Currently, Ervebo has been registered with the national health authorities in the following African countries: the Democratic Republic of the Congo, Burundi, Ghana, and Zambia. Approval from additional African countries is expected in the near future.
As previously announced, Merck Sharp & Dohme (MSD) is proceeding with the production of licensed doses and expects to begin market availability in the third quarter of 2020. MSD is working closely with the U.S. government, the World Health Organization (WHO), the United Nations Children's Fund (UNICEF), and Gavi, the Vaccine Alliance, to plan how the ultimately licensed doses will support future public health preparedness and response efforts against Ebola virus disease caused by the Zaire ebolavirus.During this transition period, MSD will continue to work urgently with the World Health Organization and partners to ensure an uninterrupted supply of the investigational Zaire ebolavirus vaccine (V920) to support international outbreak response efforts in the Democratic Republic of the Congo and neighboring countries.

Ebola virus is the causative agent of Ebola hemorrhagic fever (EHF), an acute viral hemorrhagic infectious disease. Symptoms include fever, headache, joint and muscle pain, fatigue, diarrhea, vomiting, abdominal pain, loss of appetite, and abnormal bleeding. These symptoms can appear 2 to 21 days after infection, most commonly within 8 to 10 days. Ebola is not a water-borne or food-borne disease, nor is it airborne. It is transmitted through direct contact with the bodily fluids of infected individuals or with virus-contaminated objects (such as needles).
Ervebo (V920) utilizes a defective vesicular stomatitis virus capable of infecting livestock, in which one viral gene has been replaced by a gene from the Ebola virus. V920 was initially developed by the Public Health Agency of Canada (PHAC) and subsequently licensed to NewLink Genetics in 2010. In late 2014, when the Ebola outbreak in West Africa reached its peak, Merck Sharp & Dohme (MSD) entered into a global exclusive licensing agreement with NewLink Genetics to acquire this Ebola vaccine. Since then, MSD has worked closely with various external partners to conduct an extensive clinical development program, partially funded by the U.S. government, including the Biomedical Advanced Research and Development Authority (BARDA) within the U.S. Department of Health and Human Services, the Defense Threat Reduction Agency (DTRA) of the U.S. Department of Defense, and the Joint Vaccine Acquisition Program (JVAP). The investigational supply activities for V920 have received partial federal funding support from BARDA under Contract No. HHSO100201700012C. MSD is responsible for the research, development, manufacturing, and regulatory affairs of V920, and the company has committed to working closely with other stakeholders to accelerate the continued development, production, and distribution of the vaccine.
In addition to Ervebo, Johnson & Johnson’s preventive Ebola vaccine regimen—a two-dose immunization schedule (Ad26.ZEBOV, MVA-BN-Filo)—entered accelerated assessment in the European Union in early November 2019. The vaccine regimen consists of: (1) Ad26.ZEBOV as the first dose, developed based on Janssen’s AdVac technology; and (2) MVA-BN-Filo as the second dose, administered approximately eight weeks later, developed based on Bavarian Nordic’s MVA-BN technology. Currently, Johnson & Johnson is collaborating with the World Health Organization (WHO) to register this vaccine regimen in African countries.
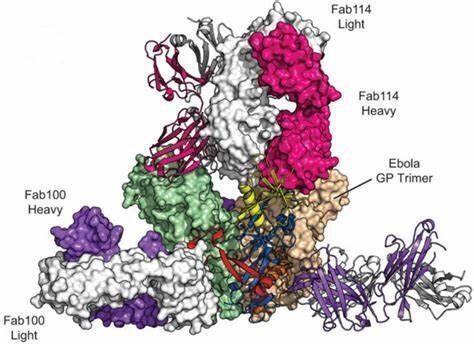
Image source: labiotech.eu
In addition to preventive vaccines, multiple biotechnology companies are developing therapeutic drugs. Of particular note is Ridgeback Biotherapeutics’Monoclonal Antibody DrugsmAb114, as well as the monoclonal antibody cocktail therapy REGN-EB3 from Regeneron Pharmaceuticals.
mAb114 is a therapeutic monoclonal antibody, which originated from the Ebola outbreak in Kikwit, Democratic Republic of the Congo, in 1995. During that outbreak,SurvivorIn Ebola infectionPersistence of Anti-Ebola Antibodies for Up to 11 Years, researchers from theseAntibodies were isolated from survivors., among which mAb114 is the most promising one.REGN-EB3is composed ofThree fully human IgG1 monoclonal antibodiesComposed ofMixture, developed by Regeneron for the treatment of Ebola virus infection.
In 2019, both mAb114 and REGN-EB3 were approved by the U.S.FDABreakthrough Therapy Designation (BTD) was granted. BTD was awarded to two drugs, both based on interim data from the Pamoja Tulinde Maisha (PALM, “Together Save Lives”) study. This study evaluated four therapies, including three antibody-based treatments (the ZMapp antibody cocktail, the triple monoclonal antibody mixture REGN-EB3 [Regeneron Pharmaceuticals], and the monoclonal antibody mAb114) and one antiviral drug, remdesivir (Gilead Sciences), with ZMapp serving as the control. Preliminary results from 499 participants, released in August of this year, showed that participants treated with REGN-EB3 and mAb114 had a greater chance of survival compared to those in the other two groups. The specific data were as follows: (1) remdesivir, ZMapp, mAb114, and REGN-EB3 were 53%, 49%, 34%, and 29%, respectively; (2) among patients treated early after infection with low blood viral loads, the data were more robust, with mortality rates of 33%, 24%, 11%, and 6%, respectively.
Currently, the overall case fatality rate of the Ebola outbreak is 67%. Based on the aforementioned data, the PALM trial was terminated early, and REGN-EB3 and mAb114 were selected as the interventions for randomized treatment of all future patients in the extension phase, to further evaluate safety until final results are obtained.Clinical TrialResults. (Bioon.com)
Original Source: ERVEBO (Ebola Zaire Vaccine, Live) Now Registered in Four African Countries Within 90 Days of Reference Countryapproval and WHO Prequalification